


1Department of Dermatology and Allergology, University Hospital, Ludwig Maximilian University, Frauenlobstr. 9–11, DE-80337 Munich, 2Department of Dermatology, Allergology and Environmental Medicine, Munich Municipal Hospital, Munich, Germany, 3Division of Dermatology, Queen’s University Hospital, Kingston, Canada, and 4Department of Dermatology, Venerology and Dermato-oncology, Semmelweis University, Budapest, Hungary. E-mail: markus.reinholz@med.uni-muenchen.de
#These authors contributed equally.
Accepted Aug 21, 2020; Epub ahead of print Aug 27, 2020
Acta Derm Venereol 2020; 100: adv00259.
Cantharidin is a well-tolerated drug, used for topical treatment of common warts and molluscum contagiosum (1). Cantharidin is extracted from beetles (genera Mylabris and Lytta, family Meloidae) (2). The species M. phalerata and M. cichorii are used widely in Chinese medicine, and Lytta vesicatoria L. (“Spanish fly”) is used in complementary medicine in Europe as an aphrodisiac. Recent studies have shown potential applications for cantharidin in post-herpetic neuralgia and leishmaniasis (3).
As a vesicant, cantharidin induces the degeneration and dissolution of desmosomal plaques, resulting in destruction of the tonofilament-desmosome-complex. While topical application of the drug is painless, it causes acantholytic blistering associated with a mild burning sensation approximately 24 h later. Skin changes resolve in 4–6 days with shedding of the wart.
Reported side-effects are erythema, pain, and post-inflammatory hyperpigmentation. Scarring, lymphangitis, cellulitis, and varicelliform dermatitis have also been reported occasionally (4–6). Cantharidin is of limited use in Germany, due to strict import requirements. In other countries, such as Canada, it is available either as mono-therapy (0.7%, 1.0%) or as combination-therapy with podophyllotoxin and salicylic acid (3, 7).
HPV-induced anogenital warts (AGW) is the most common sexually transmitted disease worldwide. HP-viruses are non-enveloped, double-stranded DNA viruses infecting keratinocytes. HPV induces activation of the AIM2 inflammasome and IL1-beta release (8). Low-risk virus subtypes (HPV 6, 11, 40, 42, 43, 44, 54, 61, 70, 72, 81, etc.), in particular, can lead to highly contagious and stigmatizing anogenital warts, which are long-lasting and often subject to frequent recurrences in immunocompromised patients.
Several treatment options are available for AGW. Some treatments are performed directly by physicians (surgical/laser removal, trichloroacetic acid, interferon, cidofovir, photodynamic therapy, cryotherapy), while others are performed by the patient (topical podophyllotoxin, imiquimod, sinecatechins). Patient discomfort and relapse are frequent shortcomings (9–11). New treatments, using mono- or combination therapy, are therefore necessary. Effective follow-up is also necessary to diagnose recurrences early, reduce their burden and the spread of infection. Since clinical examination with the naked eye might miss early recurrences, especially in the early phase, non-invasive diagnostic methods, such as dermoscopy or optical coherence tomography (OCT), can support the clinician’s evaluation. OCT enables the painless and real-time visualization of architectural changes down to the middle dermis, but without cellular resolution.
Based on our experience as a reference centre for sexually transmitted diseases, we report here a case of a patient with recurrent genital warts (GW), who was treated with cantharidin solution in an individual off-label approach.
A 32-year-old heterosexual, Caucasian man presented with a 5-year history of multiple condylomata acuminata on his penis and mons pubis (Fig. 1). He had previously undergone multiple therapeutic attempts, including 0.5% podophyllotoxin and 5% imiquimod, as well as CO2-laser therapy, electrocautery and cryo-therapy, all resulting in incomplete remission or early relapse. Due to a high level of psychological discomfort, he was avoiding sexual relationships and even social contacts.
Written informed consent for the off-label treatment was ob-tained. Cantharidin (Canthacur® solution 0.7%, Paladin Labs Inc., Montreal, Canada) was applied to the affected area (25 mm2), left under occlusive tape for 8 h, then removed.
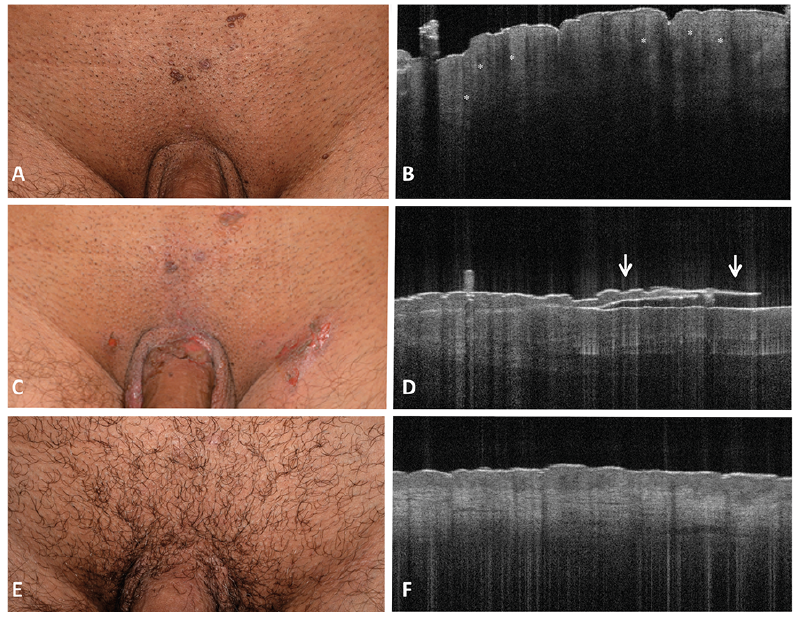
Clinical and optical coherence tomography (OCT) images (Vivosight, Michelson Diagnostics Ltd, Maidstone, Kent, UK) were collected immediately before, 1 and 28 days after treatment (Fig. 1). GW appeared on OCT as exophytic lesions with an undulated, broadened acanthotic epidermis; bright intratumoural structures, possibly indicating clusters of coilocytic keratinocytes were also visible (Fig. 1).
Twelve to 24 h after treatment, a strong inflammatory reaction, with erythema, swelling, blistering and erosions developed. Large areflective acanthotic blisters with detachment of the bright epidermal layer were visible on OCT (Fig. 1). The local skin reaction resolved after 7 days with no systemic side-effects. At follow-up (day 28), no relapse was observed; the treated area in OCT showed
o scarring, and a normal epidermis with mild remaining vasodilatation was observed (Fig. 1).
Fig. 1. Clinical and optical coherence tomography (OCT) imaging of a 32-year-old male patient with therapy-resistant genital warts undergoing local treatment with cantharidin. (A, B) Baseline, (C, D) day 1, and (E, F) day 28 (Vivosight®; scan area 6 x 6 mm, depth of focus 1.0 mm, optical resolution < 7.5 μm lateral, < 5 μm axial). In untreated genital warts, exophytic lesions present a broadened, acanthotic epidermis with an undulated appearance (papillomatosis), and bright intratumoural structures, possibly indicating clusters of coilocytic keratinocytes (*). Day 1: the blistering reaction causes detachment of the epidermal layer (D, arrows). At follow-up (F), the local skin reaction resolved with no scarring, leaving a normal epidermis with mild vasodilatation.
A recent meta-analysis of randomized controlled trials reported surgery, ablative therapy + imiquimod, and electrosurgery as the most efficacious therapies for AGW, with podophyllotoxin 0.5% as the most effective patient-administered therapy (11). Although combination approaches especially are often successful, it is known that conventional topical therapies for AGW often require a long-term approach, repeated application, and are mostly associated with discomfort, while interventional therapies can result in scarring and infections and are less effective in widely scattered warts (9–11). Thus, available treatments tend to result in reduced compliance and lower the expected therapeutic success. Introducing an effective single application topical therapy might be helpful in improving the chances of successful treatment.
At the same time, frequent relapses represent a major matter in the treatment of AGW. OCT has already proven itself useful in monitoring subclinical lesions in the field cancerization (12), as it is able to non-invasively detect epidermal alterations. It might, therefore, be of use in the follow-up of AGW. In particular, measure of epidermal thickness at baseline and follow-up, presence of OCT criteria, such as papillomatosis and intratumoural bright structures and vascularization through dynamic OCT at baseline and follow-up, should be taken into account for an objective evaluation of treatment response.
Cantharidin is an interesting alternative for the local therapy of AGW, with the advantage of a single application at the cost of an extensive local skin reaction. Larger randomized controlled studies, as for molluscum contagiosum (13, 14), are needed to better determine the treatment success and recurrence rate of AGW with cantharidin treatment. Moreover, non-invasive diagnostic techniques, such as OCT, may be useful to monitor topical treatment.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize