


1Department of Oncology and Pathology, Karolinska Institute, 2Department of Oncology, 4Department of Pathology and Cytology and 5Department of Dermatology, Karolinska University Hospital, 3Skin Cancer Center, Theme Cancer, Karolinska University Hospital, Stockholm, Sweden, 6Department of Dermatology, 7Department of Melanoma Medical Oncology, 8Department of Systems Biology, 9Department of Translational and Molecular Pathology, and 10Department of Pathology, The University of Texas MD Anderson Cancer Center, Houston, TX, USA. E-mail: hanna.eriksson.4@ki.se
Accepted Sep 24, 2020; Epub ahead of print Sep 28, 2020
Acta Derm Venereol 2020; 100: adv00334.
doi: 10.2340/00015555-3648
Bullous pemphigoid (BP) is a rare acquired autoimmune skin disease characterized by urticarial rash, pruritus and blistering. BP histopathology demonstrates a subepidermal cleft with an eosinophil-rich inflammatory infiltrate. Direct immunofluorescence (DIF) from perilesional skin usually shows a linear band of IgG and/or C3 deposits along the epidermal–dermal junction. Indirect immunofluorescence (IIF) allows the detection of serum IgG autoantibodies targeting the basement membrane zone (BMZ), primarily against antigen-BP180 and/or antigen-BP230 (1, 2). Drug-induced BP is usually associated with oral therapies (3) and has been recognized as an infrequent therapy-related autoimmune skin toxicity of immune checkpoint blockade (ICB) (4–6). Drug-induced BP is extremely uncommon in association with targeted therapy for melanoma (TT; e.g. BRAF- and MEK-inhibitors) (5, 7).
We report here 3 cases of patients with metastatic BRAFV600 mutated melanoma that developed eosinophil-rich BP-like eruptions during TT.
Case 1. A 50-year-old woman with metastatic BRAFV600 mutated cutaneous melanoma who started full-dose vemurafenib (960 mg twice daily (b.i.d)) in March 2012, at the Department of Oncology, Karolinska University Hospital (KS), Sweden, developed urticaria one week later. Vemurafenib in 50% dose and oral prednisone 20 mg daily were initiated. The urticaria resolved rapidly and full-dose vemurafenib was re-introduced one week later. In April 2012, oedema, erythema, and localized tense bullae appeared on her left leg. Vemurafenib was discontinued. Oral prednisone, 20 mg daily, was given for 5 weeks, followed by oral betamethasone, 3 mg daily, for 5 days. Her blood eosinophils were normal (0.0–0.5 K/µl) at referral, but increased to 4.6 K/µl in May 2012. Oral steroids were tapered over 2 weeks and the bullae healed. Computed tomography (CT) scan showed partial response to vemurafenib, May 2012. Treatment with dabrafenib 75 mg b.i.d in the first week and then full-dose (150 mg b.i.d) was initiated, in June 2012. The bullae neither relapsed during TT nor during the subsequent ICB therapy (i.e. ipilimumab 5 mg/ml; 3 mg/kg iv, every 3 weeks (Q3W)) followed by pembrolizumab 200 mg iv, Q3W; MK 3475-002/NCT01704287 trial) given at progression. The patient’s metastatic disease subsequently progressed on ICB therapy, and she died in December 2013.
Case 2. A 75-year-old man with metastatic BRAFV600 mutated cutaneous melanoma received full-dose dabrafenib (150 mg b.i.d) and trametinib (2 mg daily) in December 2017 after progression on pembrolizumab (25 mg/ml; 2 mg/kg iv, 3QW), Department of Oncology, KS. Four weeks later, pruritus with normal blood eosinophils (0.0–0.5 K/µl) occurred. Initially he was treated with topical steroids. Bullous eruptions on the upper body and lower extremities appeared in February 2018. His blood eosinophils increased to 0.6 K/µl. The patient had complete response to TT, but treatment was discontinued due to BP. Low-dose methotrexate (5–10 mg weekly) was initiated. The eosinophils normalized as the bullae healed in May 2018. The patient developed central nervous system (CNS) metastases in April 2018, and underwent neurosurgery and stereotactic radiation. The disease progressed off treatment and the patient died in November 2018.
Case 3. A 73-year-old woman with metastatic BRAFV600 mutated mucosal melanoma started nivolumab (10 mg/ml; flat dose of 240 mg iv, every second week) in August 2017. At progression ICB was followed by full-dose dabrafenib (150 mg b.i.d) and trametinib (2 mg daily), in November 2017, at the Department of Melanoma Medical Oncology, MD Anderson Cancer Center, USA. Three weeks later generalized pruritus, rash, bullae and inflammatory polyarthralgia appeared, with no relief on treatment with methylprednisolone (4 mg daily). TT was discontinued. Treatment with oral prednisone, 30 mg daily, followed by intravenous solu-medrol (Methylprednisolone (Pfizer, USA)), 30 mg b.i.d. was started. The eosinophils in blood increased to 0.99 K/µl. Due to uncontrolled diabetes 1.5 months later, she received 1 dose of infliximab (5 mg/kg i.v.) with oral steroid tapering. The bullae and polyarthralgia improved in January 2018, but the BP relapsed in May 2018. Eosinophils in blood increased to 0.72 K/µL and IgG to 0.06 K/µl. She received 1 dose of rituximab (375 mg/m2; 1,016 mg iv) with healing of blisters. The eosinophils in the blood decreased, but IgG remained slightly elevated, in July 2018. TT (encorafenib (450 mg daily) and binimetinib (45 mg b.i.d.)) were introduced 2 months later with off-treatment disease progression. Therapy response was not evaluated before the patient died in November 2018.
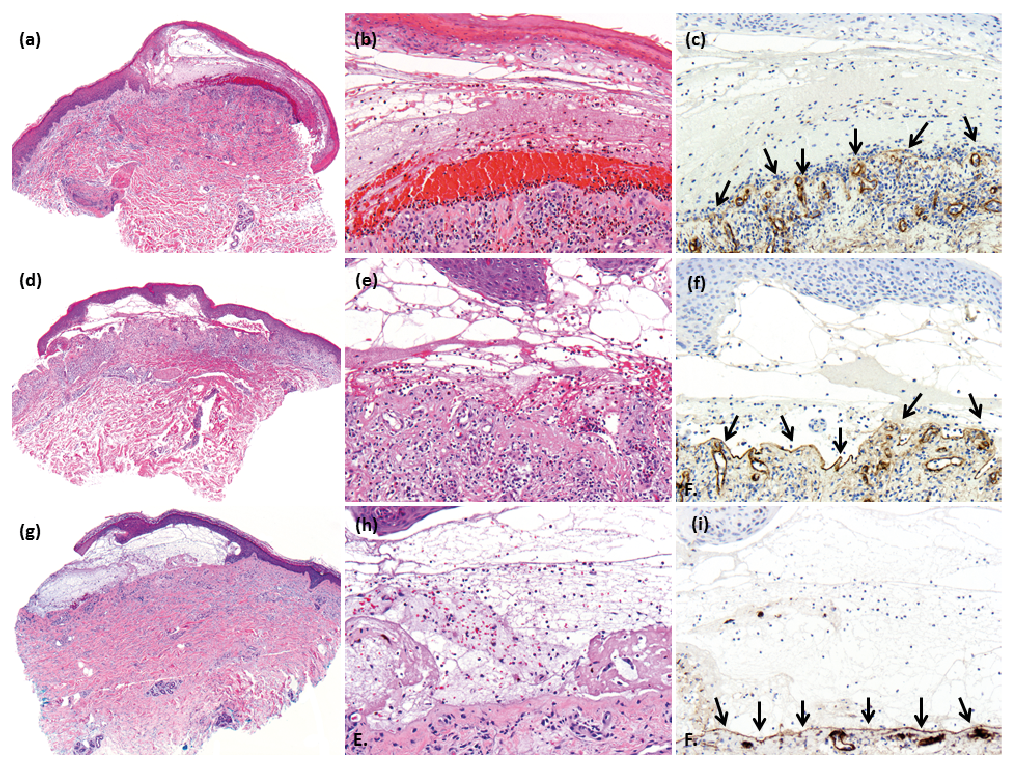
In all cases routine histology showed a subepidermal blister with eosinophil-rich inflammation within the split and in the underlying dermis (Fig. 1 a, b, d, e, g, h). In Case 1 neither DIF nor IIF were performed. In Case 2 DIF was negative and IFF detected elevated antibodies to BP180 and BP230 (2.4 and 1.2, respectively; reference < 1.0) in February 2018. BP180 remained elevated (1.4) one month later whereas BP230 was normalized (0.73). In Case 3 DIF showed linear IgG and C3 deposits at the dermal–epidermal junction and IIF showed elevated IgG antibodies. Serology for BP180 and BP230 were normal. In all cases anti-collagen IV immunohistochemistry was performed in retrospect. This labelled the floor of the blister cavity, indicating that cleavage occurred above the lamina densa of the cutaneous BMZ, supporting involvement of target antigens (BP antigens) above the lamina densa of the BMZ (Fig. 1 c, f, i).
Fig. 1. Case reports. (a–c) Case 1. (a) Routine histopathology with haematoxylin and eosin (H&E) staining (40×): Subepidermal blistering with numerous eosinophils and fibrinoid precipitation in the blister cavity. (b) Close-up (200×) view; H&E. (c) Linear reactivity of collagen IV along the basement membrane zone (BMZ) (arrows) at the floor of the blister cavity (immunohistochemistry, anti-collagen IV). (d–f) Case 2. (d) Routine histopathology (40×) with subepidermal blistering and eosinophils in the blister cavity. (e) Close-up (200×). (f) Positive labelling of collagen IV along the BMZ (arrows) at the floor of the blister cavity for Case 2 (immunohistochemistry, anti-collagen IV). (g–i) Case 3. (g) Routine histopathology (40×) with subepidermal blistering and eosinophils in the blister cavity. (h) Close up (200×) view. (i) Positive labelling of collagen IV along the BMZ (arrows) at the floor of the blister cavity for Case 3 (immunohistochemistry, anti-collagen IV).
These 3 case reports highlight that TT may be associated with BP-like skin toxicity, and that re-introduction of TT may be feasible in patients with drug-induced BP-like eruptions responding to BP treatment. However, the full criteria for diagnosis of BP were not met for Cases 1 and 2, as no DIF nor IIF were performed and DIF was negative, respectively. The morphological features of BP were present and, in a concordant clinical context, were diagnostic for drug-induced BP-like eruptions. DIF is positive in approximately 96% of regular cases of BP. BP with negative DIF occurs occasionally even when histopathological and clinical characteristics suggest BP, as in Case 2 (6, 8). A negative DIF may be due to, for example, incorrect sampling, ongoing steroid therapy, technical problems, or depositions of autoantibodies that target non-BP180- and non-BP230- antigens (1, 8, 9).
Jour et al. (6) have reported BP related to ICB or TT in metastatic melanoma. A risk for BP-like eruptions during TT and a putative additive risk of BP following treatment with ICB therapy is reflected by different clinical courses (1). Drug-induced BP usually resolves rapidly upon withdrawal of the causative medication, as in Case 1. In BP associated with anti-PD-1 therapy, skin toxicity often persists for several months after discontinuation of treatment. Cases 1 and 3 tolerated a re-introduction of TT.
The potential role of TT in BP is not clear, but these drugs may modulate the immune response through upregulation of melanoma-specific antigens, cytokines, and by increasing the infiltration of CD4+ and CD8+ lymphocytes (10, 11). BP is considered a humoral mediated autoimmune disease, but autoreactive T-cells/T regulatory cells may be involved (12, 13). Expression of BP180 has been described along the BMZ and on melanoma cells which could imply a cross-reaction against the skin in drug-induced BP-like eruptions in our report (14).
This report shows that re-introduction of TT was feasible after drug-induced BP-like eruptions. This is important if the patient is still deriving clinical benefit from TT. Referral for early BP diagnostic work-up, close monitoring and multidisciplinary management are crucial.
The authors thank the patients and their families for contributing to this report.


 Click to show fullsize
Click to show fullsize