


1Department of Dermatology, Center for Chronic Pruritus, University Hospital of Münster, Münster, 2DtoD – Data to Decision (DtoD) – AG, Hamburg, 3WIG2 GmbH Wissenschaftliches Institut für Gesundheitsökonomie und Gesundheitssystemforschung, Leipzig, 4ZEG Berlin GmbH, Berlin, 5Kantar GmbH, Munich, Germany and 6Galderma S.A./Rx Strategy & Innovation Group, La Tour-de-Peilz, Switzerland
Prurigo nodularis is an itchy skin disease with unknown epidemiology. This study aimed to describe the epidemiology of prurigo nodularis compared with that of psoriasis. The German sickness fund claims database, with 2,783,175 continuously insured patients, included 1,720 patients diagnosed with prurigo nodularis and 51,390 with psoriasis. Patients with prurigo nodularis were averagely 8 years older than psoriasis patients and more often were women (p < 0.001). Annual incidence was a constant 0.02% in prurigo nodularis, and decreased steadily from 0.53 to 0.42% in psoriasis; cumulative incidence was 0.1% for prurigo nodularis and 1.9% for psoriasis. Prevalence was 0.1% for prurigo nodularis and 4.7% for psoriasis, with a one-year mortality of 5.4% for prurigo nodularis and 1.2% for psoriasis (p < 0.001). The most frequent pre-existing comorbidities in patients with prurigo nodularis were inflammatory dermatoses and depression. This epidemiological study found a low prevalence of prurigo nodularis, manifesting different demographics and comorbidities compared with psoriasis.
Key words: prurigo nodularis; psoriasis; epidemiology; sickness fund database; real-world evidence; retrospective observational study.
Accepted Oct 2, 2020; Epub ahead of print Oct 6, 2020
Acta Derm Venereol 2020; 100: adv00309.
doi: 10.2340/00015555-3655
Corr: Sonja Ständer, Department of Dermatology, Center for Chronic Pruritus, University Hospital of Münster, Von-Esmarch-Straße 58, DE-48149 Münster, Germany. Email: Sonja.Staender@ukmuenster.de
Prurigo nodularis is an itchy skin disease of unknown origin. This study reports the occurrence and distribution of prurigo nodularis compared with psoriasis in Germany between 2012 and 2015. Among 2,783,175 continuously insured patients, 1,720 were diagnosed with prurigo nodularis and 51,390 with psoriasis. Patients with prurigo nodularis were not only older than those with psoriasis, but included more women. The cumulative incidence and prevalence of prurigo nodularis was 0.1% compared with 1.9% (incidence) and 4.7% (prevalence) for psoriasis. Annually, more patients died with prurigo nodularis (5.4%) compared with psoriasis (1.2%). Both diseases show characteristic differences among patients in Germany.
Prurigo nodularis (PN) is a chronic, highly pruritic dermatological disease, characterized by the presence of several hyperkeratotic and erosive papules and nodules that are itchy and usually symmetrically distributed (1–3). PN is a subtype of chronic prurigo, defined as “a skin disease due to neuronal sensitization to itch and development of an itch-scratch cycle” (1).
The pathogenesis of PN is not completely understood, although cutaneous inflammation and neuronal plasticity appear to play important roles (4). Various medical conditions have been reported to be associated with PN, including atopic eczema (5), systemic and neurological diseases (6), chronic kidney disease (CKD) (7), diabetes mellitus, infections (especially HIV (8)) and mental disorders (1, 9–11). Patients with PN experience continuous itching, which, in combination with the appearance of the skin lesions, has a severe impact on their quality of life, and may lead to sleep disorders, psychological and behavioural disorders, as well as social isolation (12). Epidemiology data regarding the incidence and prevalence of PN are lacking (13).
This study aimed to describe the real-world demographics and epidemiological characteristics of PN in patients identified in the German Statutory Health Insurance (SHI)-insurance database for the years 2012 and 2015. In order to benchmark against another frequent dermatosis in Germany, data for PN were compared with those for psoriasis (PsO), which does not show overlapping pathophysiology or clinics with PN, but which occurs in a similar age population with similar comorbidities.
This retrospective longitudinal study used an excerpt of a routinely collected anonymized administrative claims data pool (Source: WIG2 Ltd., Scientific Institute for Health Economics and Health System Research, Leipzig, Germany) for patients with PN from different German Statutory Health Insurance providers (SHIs). PsO is a well-studied, common chronic dermatological disease that represents a major health problem. PsO affects at least 100 million individuals of all ages and in all countries worldwide, and shows, like PN, significant comorbidities, including arthritis, cardiovascular diseases, metabolic syndrome, inflammatory bowel disease and depression (14). PsO data were therefore assessed and compared with PN data (14). The claims database contained approximately 4.3 million insured individuals between January 1, 2010 and December 31, 2016. This database was representative of age, sex, and morbidity, and can thus allow for extrapolation into the total German SHI (“Gesetzliche Krankenversicherung”; GKV) population, which constituted nearly 90% of all German inhabitants. The independent ethics committee (IEC) was waivd; however, data usage was approved by the respective health insurance companies (SHI/GKV) and all patient-level data in the database were anonymized in compliance with the German data protection regulations. Patients with PN and PsO were identified using the standard codes for diagnosis based on the International Classification of Diseases, 10th Revision, German Modification (ICD-10-GM).
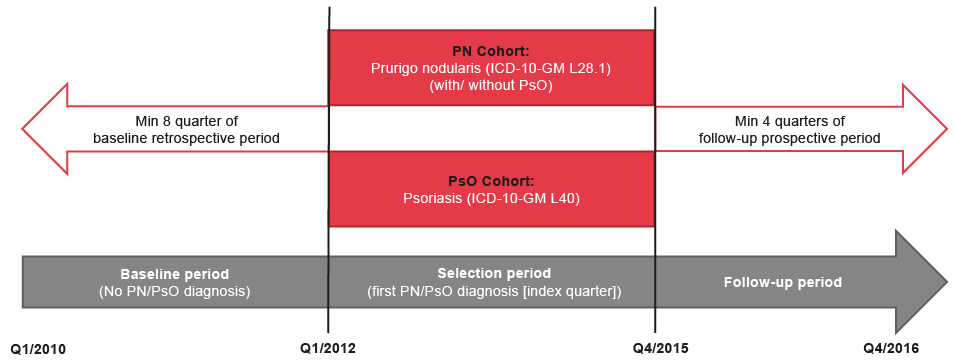
A benchmark analysis was conducted to assess the representativeness of the SHI-insured population compared with the whole German statutory health system (GKV) in the year 2015. This assessment was based on looking at the population distribution by age, sex, and comorbidity structure. Rates were calculated and tested for statistical significance between both populations. Anonymized sampled data from the SHI database was later screened for patients with at least a single PN diagnostic code of ICD-10-GM L28.1 with or without PsO codes (ICD-10-GM: L40) for the first cohort. The second cohort was made up of patients with at least one diagnostic code of PsO (ICD-10-GM: L40) and with no PN diagnosis. The code L28.1 for PN allows the clear identification of patients with PN, while other types of prurigo can be coded L28.2. Eligible patients were those continuously insured in SHI during the whole analysis period (January 1, 2010, to December 31, 2016), including decedents, who met the following inclusion criteria (see Fig. 1): (i) at least one first PN and/or PsO diagnosis during Q1/2012 and Q4/2015 (selection period); (ii) at a minimum of 4-quarters of follow-up after index quarter (follow-up period); and (iii) at least 8-quarters before index quarter (baseline period). Hence, there was a 2-year baseline period without any record of PN and PsO for both cohorts, a 4-year selection period with first PN or PsO record (representing the index quarter), and a minimum of a 1-year follow-up period for each eligible patient.
Fig. 1. Study design for patients’ selection. PN: prurigo nodularis; PsO: psoriasis.
For epidemiological comparison between PN and PsO, the incident cases were defined as all newly diagnosed patients during the selection period (1 January 2012 and 31 December 2015), with no PN and/or PsO diagnosis at baseline period. Prevalent cases were defined as all patients with at least one PN and/or PsO diagnosis recorded in each separate year (with and without the year/s before). Mortality rates included all persons who had died (without cause of death) in each study cohort within the follow-up period of a minimum of 4-quarters. Patient demographics and clinical characteristics (age, sex, and comorbidities (HIV, dermatological diseases, depression/anxiety, sleep disorders, and further relevant comorbidities)) were assessed during the baseline period for both cohorts.
For data analysis, descriptive statistics were used in describing patient characteristics, and epidemiological outcomes in each cohort. To detect differences between the cohorts, chi-square testing was used on categorical variables, which were analysed by count and percentage of patients per cohort; Wilcoxon rank-sum testing was used for continuous variables, which were summarized by the mean, standard deviation (SD) and median. Estimates for both incidence and prevalence were percentages. The incidence of the disease (PN and PsO) was calculated by use of the proportion of new (in the index quarter) occurrences of each disease divided by the population at risk before the index quarter. Two methods were used in the calculation of disease prevalence: method-one (classical prevalence calculation) took into consideration the proportion of all persons with at least one diagnosis for PN or PsO divided by the total population separately per each year. Method-two (adjusted prevalence calculation) considered counts of persons with at least one diagnosis for the disease per year and the year(s) before divided by the total population; within this method, the incident cases were consequently regarded as prevalent in the following year(s). The adjusted prevalence rate for each disease was calculated per 10,000 person-years based on the number of person-years up to the first diagnosis of disease in 2015. Comorbidity analysis in PN and PsO cohorts were calculated using the ICD-10-codes of the comorbid conditions during the 2-year baseline period. The threshold for all statistical significance was set a priori at p ≤ 0.05. For the benchmark analysis, the effect sizes (between “0”=none and “2”=huge) of the standardized differences were analysed.
Benchmark analysis
Between 1 January and 31 December 2015, a sample of 3,605,451 individuals were insured in the different SHI funds, compared with the records of 70,384,507 insured persons in the German statutory health system (GKV). Age and sex of the 2 populations (SHI vs GKV) were comparable in terms of sex-independent age groups, sex-dependent age groups, as well as sex distribution (Fig. S1). The SHI-sample appeared to be representative of the German population for the top 15 comorbidities, which including hypertension, diabetes, depression, anxiety, heart diseases, heart failure, specified arrhythmias, acquired heart valve diseases and rheumatic heart disease, polyneuropathy, chronic obstructive pulmonary disease (COPD) without permanent medication, severe bacterial infections of the subcutaneous tissue, hypertensive and/or chronic renal disease, COPD with long-term treatment, insulin therapy and angina pectoris from resolved old myocardial infarction (Fig. S2). Irrespective of the small study sample size (SHI-insured population), the effective sizes of the standardized differences for the parameters, age-, sex-, and morbidity were structurally similar to that of the GKV.
Patient selection and characteristics
Out of 4,377,381 insured persons with at least one day between the years 2010 and 2016 in the SHI database, 2,783,175 (63.58%) were continuously insured during that analysis period. Of the continuously insured persons, 1,720 (0.06%) and 51,390 patients (1.85%) were, respectively, diagnosed with first PN and PsO, identified between the study period 1 January 2012 and 31 December 2015. The mean ± SD age of patients at diagnosis in the PN cohort was significantly higher than those of patients in the PsO cohort (PN 58.23 ± 17.47 years vs PsO 50.19 ± 18.53 years, p < 0.001). However, the mean ± SD age distribution of males and female patients at diagnosis in each cohort was comparable (PN 58.28 ± 16.35 years (males) vs 58.20 ± 18.36 years (females) and PsO: 50.55 ± 17.88 years (males) vs 49.80 ± 19.21 years (females)) regarding the year of each index quarter (Table I). Likewise, there was a significantly higher proportion of women in the PN cohort (54.83%) compared with the PsO cohort (47.93%) (p < 0.001).
Table I. Age/sex distribution (selection period) and most frequent special comorbidities (baseline period) of patients with prurigo nodularis and those with psoriasis
At baseline, patients with PN were associated with significantly higher morbid manifestations compared with those with PsO. Hypertension, back pain, and special screening examination for neoplasm were the most frequent comorbidities reported in both cohorts. The prevalence rate of special conditions in both cohorts (PN vs PsO) at baseline were all statistically significant; the 3 most frequently recorded PN- and PsO-related comorbidities in both cohorts at baseline were: dermatological diseases other than PN/PsO (PN 69.13% vs PsO 54.14%, p < 0.001), followed by depression (PN 27.79% vs PsO 16.89%, p < 0.001), and atopic dermatitis (PN 15.35% vs PsO 10.83%, p < 0.001) (see Table I). Moreover, patients with PN showed statistically significant overlapping comorbidities (i.e. with more than one comorbidity) in comparison with the PsO cohort (p < 0.001), except for chronic hepatitis C, where the overlapping was marginally higher in patients with PsO (p = 0.019) (see Fig. 2). There was a non-statistically significant difference between patients diagnosed with HIV in both cohorts (0.29% (n = 5/1,720) of patients with PN vs 0.14% (n = 70/51,390) of patients with PsO, p = 0.1) at baseline. All HIV-positive patients within the PN cohort were receiving antiretroviral drug therapy (ARDT), compared with 57.14% (n = 40/70) of PsO HIV-positive diagnosed patients on ARDT (p < 0.001).
Fig. 2. Prurigo nodularis (PN) and psoriasis (PsO) patients with overlapping comorbidities (i.e. with > 1 comorbidity) at baseline.
Epidemiology and mortality
The recorded cumulative incidence rates between January 1, 2012 and December 31, 2015 were 0.06% for PN and 1.85% for PsO. The annual incidence rate of PN patients was a constant 0.02%, whereas that of PsO patients declined steadily (from 0.53% in 2012 to 0.42% at the end of the study period). The sex-related incidence rates per year and per study cohort were comparable with those of the whole study population (see Fig. 3).
Fig. 3. Annual incidence rates of prurigo nodularis (PN) and psoriasis (PsO) in patients between the years 2012 and 2015.
In 2015, the number of all SHI-insured persons with one or more PN diagnoses per year was 884, corresponding to 3.32/10,000 person-years (0.03%) compared with that of patients with one or more PsO diagnoses, which was 69,133, corresponding to 260/10,000 person-years (2.60%). However, it was observed that many diagnoses of PN in the database were only coded once; hence PN codes did not appear again in subsequent years, leading to an underestimation of the prevalence rate. Therefore, the prevalence of PN was re-assessed to include all SHI-insured persons with one or more PN diagnosed between 2012 and 2015 and/or the year(s) before, meaning that the incident cases were regarded as prevalent in the following years. With this adjusted prevalence calculation (method-two), 2,954 PN cases were identified, corresponding to 11.10/10,000 person-years (0.11%), and 125,167 PsO cases, corresponding to 470/10,000 person-years (4.70%). The age-sex adjusted prevalence rates for PN (males vs females) in the year 2015 was 9.31/10,000 men-years (MY) vs 13.12/10,000 women-years (WY) and that of PsO was 466.22/10,000 MY vs 475.12/10,000 WY for males and females, respectively (see Fig. S3).
The one-year mortality rates (not including the cause of death) during the follow-up period showed a statistically significant difference between the 2 cohorts (PN 5.41% vs PsO 1.24%; p < 0.001).
This retrospective analysis of a claims database is a detailed epidemiological study reporting the prevalence and incidence of PN patients compared with PsO patients in a large German population. In the benchmark analysis, age-, sex-, and morbidity distribution in the study population (SHI) had similar architecture to that of the German statutory system (GKV), suggesting the study sample size was representative of the German population as seen in other claims database studies (15, 16).
This study showed that PN is, as expected, less incident, and prevalent than PsO. In fact, the recorded cumulative incidence rates to PN and PsO between 2012 and 2015 were very low (0.06% vs 1.85%, respectively) and the annual incidence of PN was 0.02% throughout the study period, and that of PsO declined steadily from 0.53% to 0.42% (see Fig. 3). A prevalence of 11.10/10,000 person-years (0.11%) and 470/10,000 person-years (4.70%) was reported for PN and PsO, respectively. The current data did not reveal PN as a defined/explicit rare (European Union (EU) definition: < 5/10,000 patients) but as a low prevalent disease (with the tendency to an orphan disease); however, this must be confirmed in prospective studies.
The incident PN cases were significantly older than PsO patients. Female patients more frequently had PN, while male patients were slightly more susceptible to PsO. However, the age distribution by sex in each cohort was comparable. No sex preference has been documented so far for PN (1, 17), which also concurs with the presented data. Both diseases are more common in older patients, with a median age of 61.9 years (18, 19). PN has been reported to occur in all age groups, most commonly in older adults, with a mean age of onset at 62 years (1, 17), which is close to the mean age of 58 years for newly diagnosed patients in the current study. In addition, PN and PsO have been reported to be associated with multiple comorbidities (2, 20).
In this study, patients with PN reportedly had a highly significant association with comorbidity rates compared with patients with PsO. The most frequent comorbidities in both groups were dermatological diseases, depression, and atopic dermatitis, whereas HIV prevalence was very low in both cohorts. Boozalis et al. (2) have reported that patients with PN are more susceptible to HIV infection, a consequence of the high prevalence of HIV in patients with PN (27.20%) in the USA. In the current analysis, the HIV rate in patients with PN was 0.29% compared with a reported HIV incidence rate of 0.03 (0.02–0.04)/1,000 population for all ages in Germany in 2018 (21).
Within the benchmark analysis, it was shown that, in general, the HIV/AIDS rate plus long-term medication (HMG001) was comparably low in Germany, at 0.07% in both the SHI-insurance sample and the GKV population. Thus, though highly relevant in the USA, HIV is not a frequent predisposing factor for PN in Germany.
Various inflammatory dermatoses have been associated with PN, the most frequent being atopic eczema (1). High rates of dermatological diseases and atopic eczema as comorbidities were found in the PN cohort. Similarly, chronic kidney disease, depression, and anxiety were among frequently observed comorbidities in the presented study, as well as in other trials (1, 2, 23, 24).
In Fig. 2, among overlapping comorbidities, the highest calculated risk ratio (RR) was seen in the comorbidity CKD, which was reportedly more common in patients with PN compared with patients with PsO (RR 3.17). Since PN is a clinical phenotype with pruritus of different aetiologies including CKD, as seen in the study, CKD has also been reported in previous literature reviews to be strongly associated with patients with PN (6, 22).
Subjects with PN were associated with a 4-fold higher mortality risk compared with PsO. The mortality results should, however, be interpreted with caution, since no information was available in the claims database with regards to the possible cause of death.
Notwithstanding, these findings are representative of the entire German population, as was shown by the benchmark analysis. Data on PsO incidence are limited (14), and that available worldwide range from 0.60 to 15.04 per 1,000 person-years (25, 26). PsO prevalence in Germany has been reported to range between 2.1% (point prevalence) to 2.5% for sick fund claims data, population-based and web-based surveys (27), whereas, in our study, it was 1.8%. According to the World Health Organization (WHO) report on PsO (14), these fluctuations and differences should be interpreted with caution, since they are based on studies with different methodologies and definitions in various countries (14). Many studies report comorbidities associated with PsO, including dermatological diseases, cardiovascular diseases, and metabolic syndrome, whereas the current results showed a high prevalence of dermatological diseases and depression in these patients (28, 29). This might be explained by the fact that, despite a high number of studies reporting the association of psoriasis with comorbidities, the causality, and independence of some associated diseases remain unclear and need further research (14).
Study limitations
The following limitations should be considered when interpreting the study findings. Health insurance fund data are primarily generated for financial reimbursement transactions, not for clinical research purposes. The analysis is based completely on secondary data; thus, there might be a selection bias for the detection of the different indication groups. The German claims database used in the current study does not include information on a patient’s ethnicity, incoming level, and possible cause of death. Accordingly, there are subject to data coding limitations and data entry errors. In the presented study, however, the prevalence of PN and PsO was adjusted, by including counts of previously diagnosed PN and PsO in the year(s) before to complement missing diagnostic codes and overcome this limitation. The PN prevalence might be overestimated due to integrating incident PN cases of the previous year(s) in the prevalent ones and due to identifying PN cases only with ICD-10-codes with no verifying by any PN specific therapy. Furthermore, due to a lack of clinical information within reimbursement data, the severity grade of the diseases could not be depicted via claims codes, hence the different cases might have constituted both mild and severe PN. Considering that PN was comparatively rare and its cohort was smaller in contrast to PsO, this prompt careful interpretation of relevant findings. Despite the above-mentioned limitations, the presented study is a valuable contribution to the epidemiology of PN and PsO in Germany.
Conclusion
This is one of the first large-population epidemiological studies on PN in Europe to highlight the formerly missing incidence and prevalence data of PN in comparison with PsO. PN was shown to occur with low prevalence among German statutory insured individuals, which matches clinical experience. Although patients with PN are less frequent than those with PsO, making the diagnosis on clinical grounds is easy, as the disease has a typical appearance. Interestingly PN has different demographic characteristics compared with PsO, as extrapolated to the German SHI population. Due to low prevalence and lack of approved therapies, PN is considered a disease with a high unmet need. Thus, further research is warranted to better understand the burden of the disease and its management.
Funding sources. Galderma Pharma.
Conflicts of interest. SS is a consultant and participant in advisory boards of Almirall, Bayer, Beiersdorf AG, Bellus Health, Bionorica, Cara, Celgene GmbH, Clexio, DS Biopharma, Galderma, Menlo Therapeutics Inc., Novartis, Nuformix, Perrigo, Pfizer, Sanofi, Sienna, Trevi Therapeutics, and Vifor and has been an investigator for Dermasence, Galderma, Kiniksa, Menlo, Trevi, Novartis, Sanofi, and Vanda Pharmaceuticals.


 Click to show fullsize
Click to show fullsize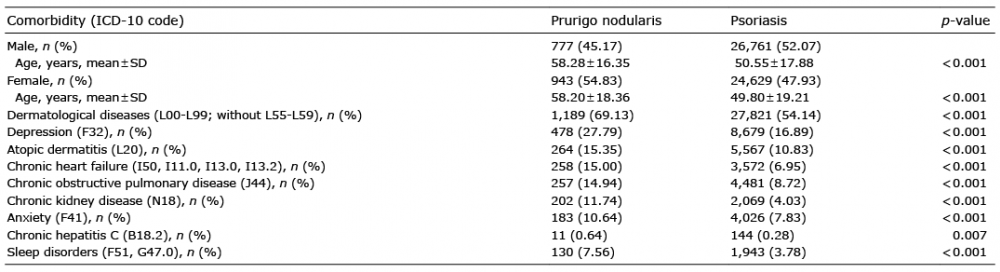 Click to show fullsize
Click to show fullsize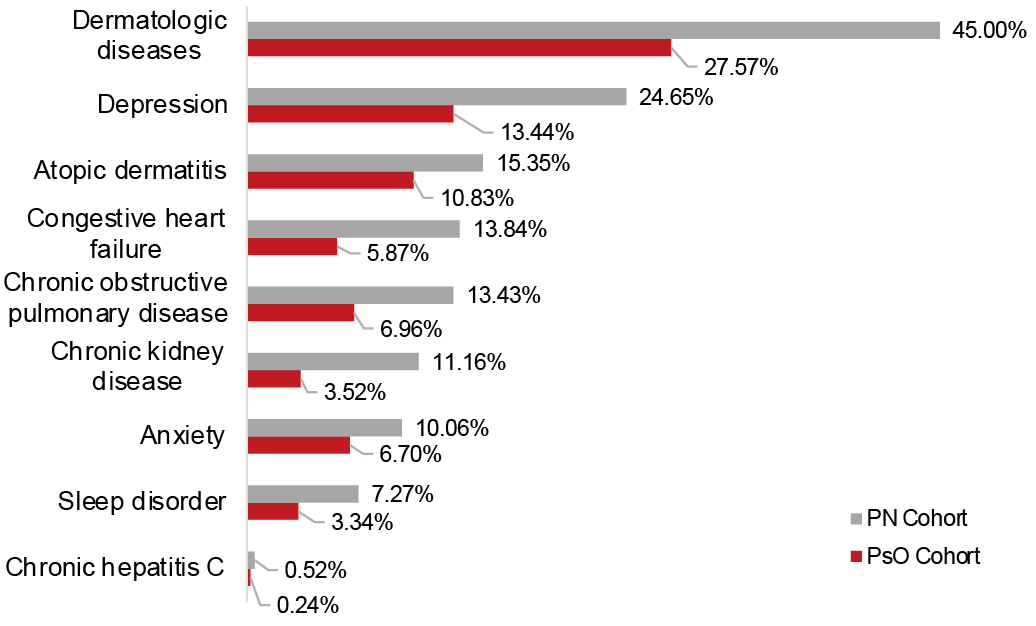 Click to show fullsize
Click to show fullsize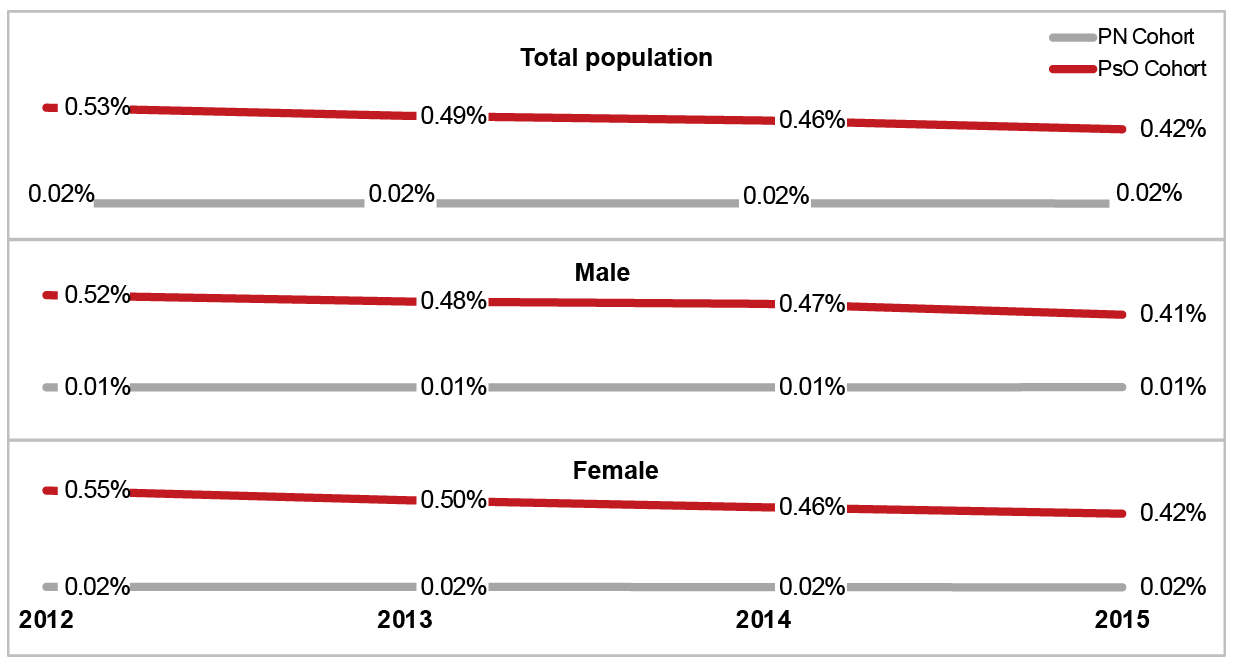 Click to show fullsize
Click to show fullsize