


Departments of 1Dermatology and Venereology, 3Infectious Disease and 5General Internal Medicine, Peking Union Medical College Hospital, 2Epidemiology and Statistics, Institute of Basic Medical Sciences at Chinese Academy of Medical Sciences & School of Basic Medicine at Peking Union Medical College and 4Center for AIDS Research, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, China
#These authors contributed equally.
Syphilis, human immunodeficiency virus (HIV), hepatitis B virus (HBV) and hepatitis C virus (HCV) share transmission routes. Syphilis infection can increase the risk of acquiring and transmitting HIV in key populations. The aims of this study were to investigate the risk factors and co-infection patterns for HIV, HBV and HCV in patients with syphilis. A retrospective study was conducted of 2,412 patients with syphilis (1,922 (79.68%) with latent syphilis, 336 (13.93%) with secondary syphilis, 78 (3.23%) with primary syphil-is, 72 (2.99%) with tertiary syphilis, and 4 (0.17%) with congenital syphilis). Positive results were observed in 8.21% (134/1,620) of patients tested for HIV, 5.75% (82/1,427) for HBV, and 1.02% (14/1,374) for HCV, respectively. Multivariate logistic regression analysis found that male sex (adjusted odds ratio (AOR) 26.03; 95% confidence interval (CI) 10.37–65.36), age < 55 years, especially age group 25–34-years (AOR 8.06; 95% CI 4.16–15.61), diagnosed at the Department of Infectious Disease (AOR 19.16; 95% CI 9.74–37.69), patients from Southern China, which is a geographical area south of the Qinling-Huaihe line (AOR 1.86; 95% CI 1.06–3.26) and having a rapid plasma reagin titre ≥1:32 (AOR 1.88; 95% CI 1.12–3.15) were independently associated with HIV infection. Risk factors for HBV co-infection in patients with syphilis, including male sex (AOR 1.78; 95% CI 1.12–2.83) and living in Southern China (AOR 4.66; 95% CI, 2.36–9.17) were also identified.
Key words: syphilis; HIV; HBV; HCV.
Accepted Oct 2, 2020; Epub ahead of print Oct 7, 2020
Acta Derm Venereol 2020; 100: adv00296.
doi: 10.2340/00015555-3657
Corr: Jun Li, Department of Dermatology and Venereology, Peking Union Medical College Hospital, No. 1 Shuaifuyuan Wangfujing Dongcheng District, Beijing, China, 100730; Xia Wan, Epidemiology and Statistics, Institute of Basic Medical Sciences at Chinese Academy of Medical Sciences & School of Basic Medicine at Peking Union Medical College, Beijing, China, 100005. E-mails: lijun35@hotmail.com; xiawan@ibms.pumc.edu.cn
Syphilis, human immunodeficiency virus (HIV), hepatitis B virus and hepatitis C virus share transmission routes. Syphilis infection can increase the risk of acquiring and transmitting HIV in key populations. It is not known whether syphilis infection also increases the risk of hepatitis B and C virus infection. This study aimed to further disentangle the association between syphilis and HIV/hepatitis B virus/hepatitis C virus, and to assess the risk factors associated with co-infection in attendees of sexually transmitted disease clinics. It was found that HIV co-infection is high in patients with syphilis. Male sex, younger, and having a higher rapid plasma reagin titre were risk factors for HIV co-infection in patients with syphilis. The hepatitis B and C virus infection rate among patients with syphilis and the general population is almost the same.
Syphilis is a chronic bacterial infection caused by Treponema pallidum subspecies pallidum. T. pallidum is an obligate human pathogen, characterized by helical shape and corkscrew motility (1), which can spread by sexual transmission, mother-to-child transmission, and blood transfusion. Without treatment, the disease can progress over years through a series of clinical stages, leading to irreversible neurological, ocular, cardiovascular, and internal organ damage, and even death. According to the estimates from the WHO (2), there were approximately 6 million new cases of syphilis worldwide in 2016, despite the existence of effective prevention and control measures. In China, the incidence of syphilis has increased dramatically during the last 30 years (3), and syphilis is now among the top 3 reported communicable diseases in China (4).
The increase in rates of syphilis is concurrent with an increase in the rate of human immunodeficiency virus (HIV) infection (5–9). It is well recognized that there is a significant association between syphilis and HIV infection (1). A systematic review of studies from the USA revealed that 15.7% of patients with syphilis were co-infected with HIV. Co-infection with HIV usually leads to atypical and aggressive evolution of syphilis (10, 11). The importance of syphilis as a co-infection in HIV-infected individuals stems not only from the negative effect of syphilis on the natural course of HIV infection, but also from an increase of HIV transmission (12–14).
Syphilis, HIV, HBV and HCV share common routes of transmission (sexual transmission, mother-to-child transmission, and blood transfusion). In addition, there are a few key populations, such as men who have sex with men (MSM), commercial sex workers, and injection drug users, who have high rates of co-infection (15–21). Some studies have focused on analysing co-infections with HBV, HCV and syphilis in patients with HIV (16, 24), but there are limited studies (6, 21) of co-infections and risk factors for HIV, HBV, and HCV in patients with syphilis. The aims of the current study were to investigate the patterns and risk factors for co-infection with HIV, HBV and HCV in patients with syphilis.
Study design and setting
This retrospective study reviewed the medical records of all outpatients diagnosed with syphilis in Peking Union Medical College Hospital (PUMCH), Beijing, China, from January 2013 to December 2017. The STD clinic at PUMCH is one of the largest in China. The clinic often receives patients from distant areas within mainland China. Routine screening and treatment for STDs are avail-able at the clinic. Information on sociodemographic and medical characteristics (including clinical information, laboratory testing data, etc.) were extracted. Information on sociodemographic characteristics included sex, age, ethnicity, residence, and occupation, and clinical data included stage of diagnosis, symptoms present at the time of diagnosis, treatment information, and follow-up clinical symptoms. Laboratory results for syphilis included rapid plasma reagin (RPR); Shanghai Kehua Bio-engineering Co., Ltd, China), particle agglutination assay for antibody to T. pallidum (TPPA; Fujirebio Inc., Japan), and fluorescent treponemal antibody absorption (FTA-ABS; EUROIMMUN AG, Inc., Germany) results. Data on HIV, HBV and HCV status and co-infection with other STDs (including genital warts (diagnosis of genital warts was clinically made by visual inspection), Chlamydia trachomatis infection, genital herpes, and gonorrhoea) were also collected. The study was approved by the ethics committee of PUMCH (S-K653).
Definitions
Chinese national guidelines (22) define primary syphilis as a clinically compatible case characterized by one or more chancres and inguinal lymphadenopathy in combination with laboratory confirmation of T. pallidum in clinical specimens by any 2 of the following methods: direct detection of T. pallidum (i.e. silver staining, dark-field microscopy, direct fluorescence antibody test-ing and nucleic acid amplification tests), RPR and TPPA, and/or FTA-ABS. Secondary syphilis is defined as a clinically compatible case characterized by maculopapular rash and, in many cases, lymphadenopathy, in combination with a laboratory test confirmation as for primary syphilis. Latent syphilis is defined as an asymptomatic case with a possible history of infection supported by reactive RPR and a reactive treponemal test. Tertiary syphilis is defined as a case with a history of primary, secondary, or latent syphilis with clinical manifestations involving the cardiovascular, ocular, or central nervous system in combination with laboratory confirmation by reactive RPR or cerebrospinal fluid abnormalities characterized by higher than normal amounts of white blood cells (> 8 × 106 cells/l) or protein (> 0.45 g/l).
Statistical analysis
SPSS version 25.0 (SPSS, Inc., IBM Co., Armonk, NY, USA) was used for data analysis. Frequency (proportion) and mean (standard deviation; SD) were applied to describe participant characteristics and HBV, HCV and HIV infection status. Univariate analyses, including t-test, χ2 test and Fisher exact test, were then used to examine the differences between the characteristics of each infection. Multivariate logistical regression models were applied to determine risk factors for co-infection with HBV, HCV and HIV among patients with syphilis, respectively. p-values < 0.05 were considered to indicate statistical significance.
General description of participants
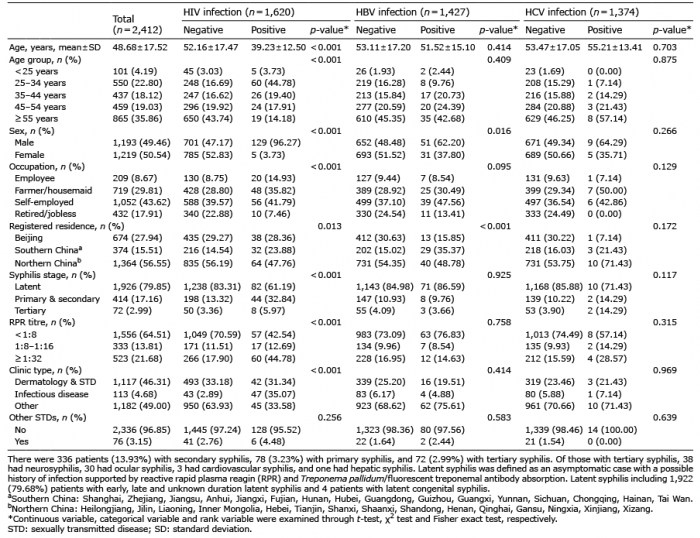
A total of 2,412 patients diagnosed with syphilis in various stages were enrolled in the study. Demographic and clinical characteristics for the participants are shown in Table I. Among the 2,412 patients with syphilis, 1,922 (79.68%) had latent syphilis, 336 (13.93%) had secondary syphilis, 78 (3.23%) had primary syphilis, 72 (2.99%) had tertiary syphilis, and 4 (0.17%) had congen-ital syphilis. Of those with tertiary syphilis, 38 had neuro-syphilis, 30 had ocular syphilis, 3 had cardiovascular syphilis, and one had hepatic syphilis. Co-infection with other STDs was found in 76 (3.15%) patients; among these patients there were 34 HSV2 infections, 27 cases of condyloma acuminatum, 10 cases of C. trachomatis, and 9 gonococcal infections.
Table I. Univariate analysis of various characteristics and their influence on hepatitis B virus (HBV), hepatitis C virus (HCV), and HIV co-infection status in patients with syphilis
HIV/HBV/HCV co-infection and associated co-infection factors
Of 2,412 patients with syphilis, 1,620, 1,427, and 1,375 received HIV, HBV, and HCV tests, respectively. Co-infection with HIV was found in 8.21% (134/1,620) of tested subjects. In a univariate analysis, all the variables except co-infection with other STDs listed in Table I were statistically significant for the incidence of HIV infection (p < 0.05). Multivariate logistic regression analysis found that male sex (AOR 26.03; 95% CI 10.37–65.36), age less than 55 years, especially age group 25–34-years old (AOR 8.06; 95% CI 4.16–15.61), diagnosed at Department of Infectious Disease (AOR 19.16; 95% CI 9.74–37.69), patients from Southern China, which is a geographical area south of the Qinling-Huaihe line (AOR 1.86; 95% CI 1.06–3.26), and having a RPR titre of ≥ 1:32 (AOR 1.88; 95% CI 1.12–3.15) were each independently associated with HIV infection (Table II).
Table II. Multivariate logistical regression for risk factors for HIV co-infection in patients with syphilis
HBV co-infection was found in 5.75% (82/1,427) of tested subjects. Multivariate logistical regression (data not shown) for risk factors of HBV co-infection in patients with syphilis showed that male sex (AOR 1.78; 95% CI 1.12–2.83) and living in Southern China (AOR 4.66; 95% CI 2.36–9.17) were associated with HBV infection. HCV co-infection was found in 1.02% (14/1,374) of tested subjects. Neither univariate analysis (Table I) nor multivariate logistical regression (data not shown) identified any factors associated with HCV co-infection status.
This study revealed the co-infection pattern of HIV, HBV and HCV in patients with syphilis from a national integrated healthcare organization, and identified certain high-risk populations for HIV and HBV co-infection. Co-infection with HIV was found in 8.21% of patients with syphilis, which was much higher than the 0.058% seroprevalence of HIV in healthy individuals who were screened for health examination at our hospital (23). Although there were selected individuals diagnosed at the Department of Infectious Disease (52.22%) and Dermatology & Sexually Transmitted Diseases (7.85%) with greater HIV seroprevalence, a lower baseline HIV seroprevalence was observed in all the patients tested in the 2 departments (3.27% and 1.35%, respectively) (23). Patients with syphilis are at a higher risk of being infected with HIV than the general population (21). Sy-philis, as one of the genital ulcer diseases, can increase HIV transmission by a variety of biological mechanisms, which probably affect both the infectiousness of and susceptibility to HIV (1). One biological explanation for the increased susceptibility to HIV among individuals infected with syphilis is based on the theory that the breakdown in mucosal integrity due to ulceration provides a portal of entry for the HIV virus (12). In addition, this ulceration may result in a local influx of CD4+ lymphocytes, thereby increasing the number of HIV target cells (12–14).
In the current study, male patients with syphilis were much more likely to be co-infected with HIV. The discrepancy regarding sex may be linked with the reported baseline seroprevalence of HIV (0.37% and 0.09% for men and women, respectively) (23). The most likely explanation for the male precedency in HIV infection seems to be the high prevalence of HIV/syphilis co-infection in the MSM population (9, 24–26). Unfortunately, because behavioural information for the study subjects, includ-ing their sexual orientation, condom use, and number of sexual partners, is incomplete, these variables were not included. In addition to the factor MSM, males are more likely to initiate sexual intercourse, have more frequent sexual intercourse and significantly higher risk behaviour than females (27), which may also increase the HIV infection risk in males.
Younger age (< 55 years), especially among the 25–34-year-old age group, and coming from Southern China were also identified as risk factors for co-infection with HIV in patients with syphilis, which was consistent with the age and regional distribution of national HIV incidence (28). Young people are more susceptible to STDs, including syphilis and HIV, because they are more sexually active and may engage in unsafe sex. Rates of condom use have increased among young people; how-ever, inconsistent use of condoms and multiple different partners contribute to a higher risk of STDs and HIV. The 15–24-year-old age group has the highest rates of STDs in the majority of the USA (29). Patients with a younger age may have less access to information about STDs and prevention methods, safe-sex practice, and healthy behaviours (30, 31). Given the worrying status of awareness about STDs among young people reported by previous studies (30, 31), there is an urgent need to implement STD education for adolescents and young people. New strategies for accessing and counselling young people, such as addressing this population during secondary school, or even primary school, are needed to implement a more appropriate healthcare policy in China.
Patients with co-infection with early-stage syphilis and HIV have been shown to usually have a higher titre on non-treponemal serological tests (e.g. RPR and Venereal Disease Research Laboratory (VDRL)) than patients with syphilis without HIV infection (32–34), which may be caused by inappropriate B-cell activation in HIV-infected patients (33). This result may partially account for our finding that having a RPR titre of ≥1:32 is independently associated with HIV infection in patients with syphilis.
HBV infection remains a serious public health problem in China (4, 35). It was estimated that the prevalence of HBV (as measured by HBsAg detection) in 2016 was approximately 6.1% (5.5–6.9%) in China (23, 36). The current study detected co-infection with HBV (HBsAg) in only 5.75% of patients with syphilis, which is consistent with the rate in the general population (37). In addition, male sex and living in Southern China were identified as risk factors for HBV co-infection in patients with syphilis, which was consistent with the reported findings of a national epidemiological serosurvey of HBV (38). In the general Chinese population, the estimated prevalence of HCV is approximately 1.0–2.9% (39–41). Thus, co-infection with HCV was found in 1.02% of patients with syphilis, indicating that syphilis infection may not increase infection with HCV, similar to the situation for HBV.
Study limitations
This study has some limitations. First, the data are from a retrospective study design. Secondly, not all of the patients with syphilis received HIV, HBV and HCV tests. Thirdly, all the patients were enrolled from PUMCH, which may cause some potential bias. Finally, data regarding some important co-factors, such as sexual orientation, number of sexual partners, etc., are missing due to incomplete information, which could lead to confounding bias. Despite these limitations, the results of the current study have several important public policy implications. Firstly, this study supports screening for syphilis in high-risk populations, such as STD clinic attendees, as a decisive measure through which to better control syphilis. Testing methods for syphilis are relatively simple and cost-effective, and expanding screening services to high-risk populations could prove beneficial not only in preventing future syphilis, but also future HIV infection and congenital syphilis in China. Secondly, HIV testing should be pursued aggressively in patients with syphilis, particularly for males, those in younger age groups, or with RPR titre ≥1:32, of whom a significant portion is co-infected with HIV. Thus, STD clinic surveillance plays an invaluable role in monitoring HIV seroprevalence, and, more importantly, new HIV infection. Lastly, because the HBV/HCV infection rate among patients with syphilis and the general population is almost the same, HBV/HCV testing should be recommended for patients with syphilis, using the same criteria applied to members of the general population.
Conclusion
Male sex, age less than 55 years, especially the age group 25–34-years-old, and with a RPR titre ≥ 1:32 were found to be risk factors for HIV co-infection in patients with syphilis. However, the HBV/HCV infection rate among patients with syphilis and the general population is similar.
We thank the patients, physicians (staff and investigators) and study coordinators for their hard work. We thank Shao Xia Xu, Qiao Feng Wang and Wei Hong Zhang for their assistance in laboratory testing; Jun Wang and Lian Ma for their support in data collection and project implementation in the field. We are grateful to Professor Qun Xu from the Department of Epidemiology and Health Statistics, Peking Union Medical College, China, for contributing to statistical analysis. Special thanks are extended to the hospital Infection Office and Department of Clinical Laboratory for their support in this study.
This study was supported by Beijing Municipal Science and Technology Commission (Z191100006619011) and Capital’s Funds for Health Improvement and Research (2020-2-4016).
This study was approved by the institutional review boards of the Peking Union Medical College Hospital (reference number S-K653). All patients consented to participate in this study.
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize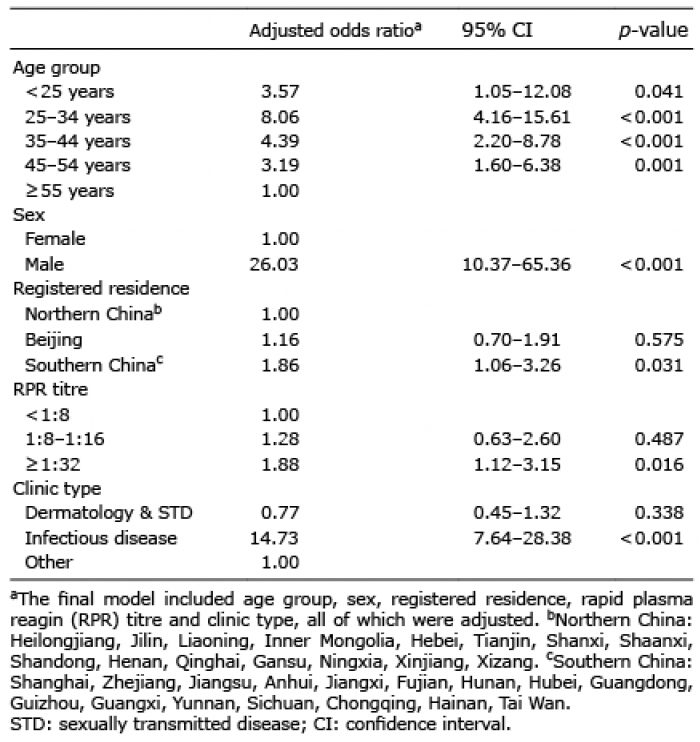 Click to show fullsize
Click to show fullsize