


1Department of Women’s and Children’s Health, 2Section of Clinical Bacteriology, Department of Medical Sciences, Uppsala University, and 3Department of Clinical Microbiology, Uppsala University Hospital, Uppsala, Sweden
Internet-based testing for Chlamydia trachomatis and Neisseria gonorrhoeae is a public health service in Sweden. However, knowledge about users of the service is limited. This study examined experiences of using the C. trachomatis/N. gonorrhoeae self- sampling service. Individuals ordering a free-of-charge C. trachomatis/N. gonorrhoeae self-sampling test from an eHealth website in 2018/2019 were invited to complete a questionnaire. Of the 1,785 participants 69.4% were women. The majority of participants (77.1%) were single and heterosexual (88.2%) and 5.3% of samples tested positive. The self-sampling service was appreciated, with > 90% considering it good/very good. The main reason subjects gave for testing was to check their health after unprotected sex (72.9%). Almost half (44.7%) had regretted having sex after alcohol intake. Differences in attitudes were seen between categories: born vs not born in Sweden, employed vs student, single vs married/having a partner. Participants were happy with the self-sampling test service, and sexual risk behaviours motivated use of the test.
Key words: Chlamydia trachomatis; attitudes; eHealth; public health; sexual behaviour; sexually transmitted infection.
Accepted Oct 21, 2020; Epub ahead of print Oct 26, 2020
Acta Derm Venereol 2020; 100: adv00315.
doi: 10.2340/00015555-3677
Corr: Björn Herrmann, Section of Clinical Bacteriology, Department of Medical Sciences, Uppsala University, SE-751 85, Uppsala, Sweden. E-mail: bjorn.herrmann@medsci.uu.se
Chlamydia trachomatis is a common sexually transmitted infection, which may cause severe reproductive complications. Widespread testing in combination with treatment and partner notification is vital to interrupt the spread of infection. Although internet-based testing is well- established, the data regarding the user experience is scarce. This study gives users’ perspective on internet-based self-sampling, which is valuable for healthcare providers. The main findings revealed that the 1,785 participants were happy with the self-sampling test service and that their sexual risk behaviours motivated them to use the test. This public health service provides a user-friendly and valuable tool to reduce chlamydia infections.
Chlamydia trachomatis (CT) is the most frequently detected bacterium in sexually transmitted infections (STIs) and may cause complications, such as pelvic inflammatory disease, ectopic pregnancy and infertility. To achieve disease control and reduce complications, testing for CT in combination with treatment and partner notification is important in breaking the epidemiological chain of infection (1). Guidelines recommend annual screening of sexually active persons aged < 25 years (Centers for Disease Control and Prevention only women) (2, 3). Several countries, such as England, Sweden, Denmark, Norway, Finland and Estonia, have a practice of generous testing, with the aim of reducing transmission and chlamydia-associated complications (4).
To facilitate CT testing, the use of internet-based self-sampling at home with analysis at a hospital laboratory has been evaluated in several studies (5–7). An initial study in Sweden indicated that internet-based self-sampling reached men to a greater extent and had the potential to decrease the workload in clinics (8). Currently, this service is an integrated part of the healthcare system all over Sweden and covers both CT and Neisseria gonorrhoeae (NG). The diagnostic outcome of self-sampling has been compared with clinic-based testing, and was recently evaluated on a national level (9). Self-sampling now comprises more than 20% of all CT tests, which is a higher proportion than reported from other countries (10, 11), and represents more than 20% of chlamydia cases detected. Furthermore, the positivity rate is higher than in clinic-based testing, and self-sampling reaches men slightly more than clinic-based testing. Although the concept of internet-based testing is well established, little data is available about users and their experiences of internet-based self-sampling, especially when this service is an integrated part of the healthcare system. This study aimed to characterize users and determine their opinions about internet-based self-sampling tests for CT and NG.
An invitation to participate in an evaluation of the internet-based self-sampling service for CT/NG was sent to 4,000 consecutive users via the public healthcare website www.1177.se in the Uppsala Region, Sweden. The region has 376,000 inhabitants living in one large university city, a few smaller towns and in rural areas. Website www.1177.se is a national service, widely used for different healthcare issues, such as: information about diseases, advice for illness with on-line contact with a nurse, booking appointments with healthcare providers, prescriptions of drugs, results of tests. Furthermore, citizens can access their own patient record. Thus, the self-sampling service is embedded in the standard healthcare system. The self-sampling service can be used by persons above 15 years of age who have a national registration number. Tests can be ordered repeatedly.
In the self-sampling service for CT/NG, men accounted for 34.0% and the 15–29 years age group for 72.5% of the self-sampled tests (9). No economic incentive was used.
Those agreeing to participate in the study were sent an internet-based questionnaire that comprised 27 questions (see Appendix S1; Questionnaire 1) and was based on previous research and clinical experience (12). The questionnaire was tested on 3 representatives of the public before final design, and was answered anonymously during the period December 2018 to July 2019. For additional information about the testing procedure, see Appendix S2.
The first part captured background demographic data, while the main part comprised questions about sexual behaviour, previous STI testing and STIs, reasons for testing and attitudes to the self-sampling service. The questions had multiple-choice alternatives and included questions about the main reason for taking the test and suggestions for improvements. Open-ended questions were analysed by systematically organizing and categorzsing the answers.
In addition, a questionnaire with 6 questions was sent to 1,209 persons who had requested a test kit without returning it to the laboratory, in order to explore their reasons for not returning the test, see Appendix S1; Questionaire 2).
Data were entered and analysed using Statistical Package for the Social Sciences (SPSS), version 26. Differences between groups were tested with Student’s t-test, a χ2 test and Fisher’s exact test. A p-level < 0.05 was considered significant. The study was approved by the Swedish Ethical Review Authority (Dnr. 2018/250).
Characteristics of participants
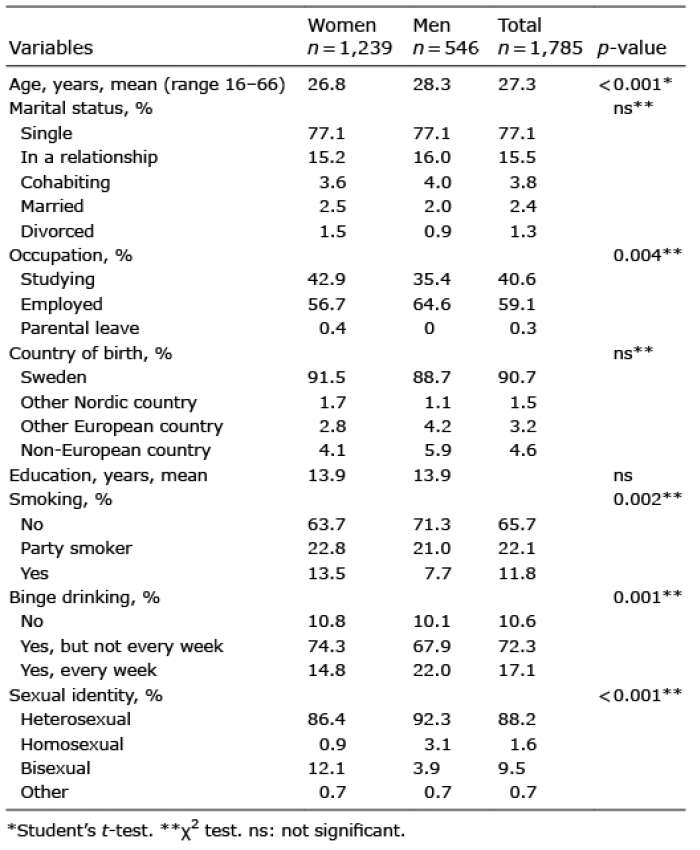
The questionnaire was returned by 1,785 people (37%) with a mean age of 27.3 years, 30.6% of them men. Table I presents the characteristics of the participants and Fig. S1 their age distribution. The majority of participants (1,653 (92.6%)) were single or in a relationship, but unmarried and not cohabiting. More than half were employed (1,055 (59.1%) and 725 (40.6%) were students. Almost 10% of the respondents were born outside Sweden and the vast majority (1,574 (88.2%)) were heterosexual.
Fifteen percent (n = 269) of the 1,785 respondents had not sent in a sample to be tested. Eighty of those who had sent in their samples tested positive for chlamydia and one tested positive for gonorrhoea; 5.3% in total.
Table I. Characteristics of the participants
Reasons for not returning the test
A total of 279 (23.1%) of the 1,209 individuals who had requested a test kit without returning it to the laboratory completed the additional short questionnaire. The majority, 246 (87.9%), were born in Sweden with a mean age of 27.1 years (range 18–60 years), and 73 (26.1%) were men, 201 (71.8%) women, and 3 (1.1%) of other gender identity. Half of the participants, 140 (50.2%), were employed and 118 (42.1%) were students. There were several reasons for not returning the test: 92 (32.9%) had taken the test at a health clinic instead of the home self-sampling test, while 63 (22.5%) reported lack of time, and 34 (12.1%) had not returned the test as they were no longer worried about being infected. In addition, 18 (6.4%) considered it good to have the test in case they had new sexual partners in the future. Finally, 72 participants (25.7%) reported other reasons, as presented below, with illustrative quotations for clarification.
Other reasons expressed by respondents. According to 32/90 comments (35.5%), respondents “never received the test”, i.e. the ordered test never arrived by post, or the test was taken and returned to the laboratory, but got lost on the way. “I put the envelope in the postbox but the postal service must have sent it somewhere else.” The time limit on self-sampling was mentioned as a barrier (n = 20, 27.7%), and “I totally forgot” to return the test (n = 12, 16.6%) was another reason highlighted. In addition, 6 participants (8.3%) reported “mistakes they had made”, such as dropping the test or the swab, while 8 (11.1%) reported “personal circumstances”, sickness or family matters as reasons for not returning the test. “I’ve had a hysterectomy and cannot take a vaginal swab at the moment.”
Sexual experiences and infections
Table II presents a number of variables related to sexual activities during the last 12 months, as well as previous experience of STIs, whether or not respondents had previously taken an STI test and, if so, in what way. Women had been tested to a larger extent than men and a larger proportion of women had previous experience of an STI. Almost half of the participants had regretted having sex after alcohol intake.
Table II. Sexual experiences, sexually transmitted infections (STIs) and STI testing
Opinions about the self-sampling service
Table III shows participants’ reasons for taking the test and also their opinions about the self-sampling service. The main reason for taking the STI test was to check one’s health after unprotected sex. The self-sampling option was highly appreciated, with more than 90% of the participants rating it as good/very good. More than half responded that a waiting time of up to 5–6 days for the result was acceptable. Six out of 10 could consider paying a fee for the service, but 4 out of 10 stated that they would not use the service if they had to pay for it. Most participants would take a test elsewhere if the home-based self-sampling service did not exist, but 15% of the men would not take any test if this option was not available.
Table III. Opinions about home-based home sampling for chlamydia/gonorrhoea
Those who had tested positive did not differ from participants with a negative test result with respect to any of the demographic variables. Some differences were, however, found in opinions about the service. Swedish-born participants were more in favour of the self-sampling service than were foreign-born. Single respondents were more positive about use of self-sampling than those who were married/cohabiting, and those who were employed were more positive than students. Furthermore, participants who had regretted having sex after alcohol intake and those with a negative test result had more favourable opinions about the home-based self-sampling service (Appendix S2, Table SI).
Female participants, those who were single, those who had regretted having sex after alcohol intake, those who had previously been tested and those with a positive test result were more inclined to take a test elsewhere if the home-based self-sampling service did not exist (Appendix S2, Table SI). Respondents who were not prepared to pay were more likely to have had a chlamydia infection than those who were prepared to pay (41.5% vs 36.4%, p = 0.045). However, no differences were found if all previous STIs were included. No differences were found in readiness to pay related to having regretted having sex after alcohol consumption, but some differences in the mean number of unknown sexual partners during the previous year: a mean of 1.94 for those not prepared to pay compared with 1.58 among those prepared to pay (p = 0.036). Furthermore, those born outside Sweden were more prepared to pay than Swedish-born participants; 72% compared with 62.2% (p = 0.013).
Suggestions for improvement of the internet-based self-sampling service
In all, 330 comments with suggestions for improvement were analysed with quantitative content analysis, grouped into 5 categories: “Works well as it is”, “Include tests for other STIs”, “Clearer information”, “Time perspective – should be handled faster” and “Should be better promoted and marketed” (Appendix S2). In the majority of participants’ comments, 171/330 (51.8%), no suggestions for improvement were found. The service was considered to work well as it was and participants appreciated it and found it convenient and easy to use. They expressed their gratitude and hoped that the service would continue to be easily available and free of charge. “No, it works perfectly well as it is today. Very good service!”.
The study shows that internet-based self-sampling for CT/NG is highly appreciated by users, who would undergo considerably less testing if only clinic-based testing facilities were available. The behavioural risk profile of the users and their previous STI test results indicate that the service reaches a relevant target group. The main reason for testing was to check one’s health status after unprotected sex.
One strength of the study is that questionnaire respondents appeared to be representative of users of the test service, since the CT positivity rate (5.3% vs 5.5%) and the proportion of men (69% vs 66%) were similar to results from our national evaluation of the diagnostic outcome of the service (9). Another strength is that the study is based on users of an established public healthcare service and the respondents therefore represent a real-world situation. At the same time, a response rate of 37% indicates that the results may not provide a complete picture of users’ experiences of the test.
If a public health service is free of charge it is important that it reaches the intended target group, i.e. persons with an increased risk of being infected by CT/NG. The respondents in our study had several sexual partners, often without protection and also in combination with alcohol use. Furthermore, the predominant reason for using the test was to check health status after unprotected sex, while checking one’s health after treatment was rarely given as a motive. Users are thus aware of their risky behaviour and are a relevant target group for CT/NG testing.
A key finding was the considerable appreciation of the test service, with 93% rating it as good/very good. Our results from an established public healthcare service are in line with a recent evaluation in the UK, where 91% were happy using the online system and receiving results within one week (13). Self-sampling as a collection technique was considered to be well-received and acceptable by, on average, 85% of respondents in a plethora of previous studies in different settings and countries (14). The online service is also consistent with young people’s positive attitudes towards digital STI services (15).
More than half of the respondents in our study accepted a turnaround time from sending the sample to receiving the result in ≥ 5 days, which is in agreement with another study (16), where respondents rated test accuracy higher than time to result. Furthermore, in that study as well as in a Dutch study (17), young people preferred not to have direct contact with professionals for STI healthcare. This indicates that there may be decreasing acceptance of partner notification with face-to-face interviews in the future, impeding case detection.
The appreciation of the test service may explain why two-thirds of users are ready to pay, and a small charge for the test would probably reduce the 25% of delivered test kits that are never returned (9). At the same time, a substantial proportion would not use this service if there was a fee, and some would not even use clinic-based testing.
The impact of the chlamydia test per se on the individual has been investigated previously. In a Dutch study, CT positives were more likely to change their behaviour in a more positive and protective direction after their test result than CT negatives, who were more likely to shift towards riskier behaviour (18). Respondents in a British study reported that being tested for chlamydia “had a positive impact on their subsequent sexual behaviour or service use” (19). However, that was a cross-sectional study, so it was not possible to compare participants’ sexual and healthcare-seeking behaviour before and after testing. But even if testing may have a positive effect on behaviour and users greatly appreciate internet-based self-sampling at home, this service must be used with some caution. It has been suggested that, by delivering sample kits to target populations, it could be a tool for increasing CT screening (7, 20). However, indiscriminate use of screening may not serve the intended purpose, and, in addition, randomized controlled trials indicate that screening has a limited effect on prevalence of CT (21, 22).
The respondents were asked to suggest ways of improving the self-sampling service. Extended use, including rectal and throat self-sampling for CT/NG, was suggested and has been found to work (23). Approximately a 5th of the comments called for a service that included more STI agents, such as mycoplasma, herpes and human papillomavirus. Users choosing tests, including CT/NG, syphilis and HIV, has been applied in an evaluation of online sexual health services (24), but indiscriminate user-directed testing is problematic, given increasing problems of antibiotic resistance in Mycoplasma genitalium and interpretation of test results for human papillomavirus.
All participants provided a postcode, indicating geographical and socioeconomic area. The participants represented different areas, from the southern parts to the northern parts of Uppsala Region, including both rural and city areas. The number of immigrants was lower compared with the population at large. Individuals born outside Sweden, especially those from war-torn countries, have poorer health compared with Swedish-born individuals and face challenges in seeking healthcare due to language barriers and for cultural reasons (25, 26). Interestingly, those born outside Sweden were more willing to pay for the test than Swedish-born individuals, indicating that eHealth and self-sampling testing could target immigrants with higher socio-economic status, but, as a result, may not reach the population at large. Missing values were few, not exceeding 5% for any of the items. Although the response rate was only 37%, implying limitations in interpreting the results, we believe that the study could be representative of similar contexts.
This study gives the users’ perspective on internet-based self-sampling, which is of value to healthcare providers. However, further development and evaluation of the concept within established healthcare services, and not only in a study format, is warranted. Unanswered questions are: Can extragenital sampling be included? Can additional test agents be included without doing more harm than good? Will a risk score quiz before ordering a test lead to greater precision in reaching the infected target group?
In summary, the public health service of internet-based self-sampling testing for CT/NG is highly appreciated by users. Their behavioural risk profiles and their previous STI test results indicate that the service reaches a relevant target group. The main reason for testing was to check health status after unprotected sex.
This study received funding from the Public Health Agency of Sweden. The funders had no role in conducting the study or interpreting the results.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize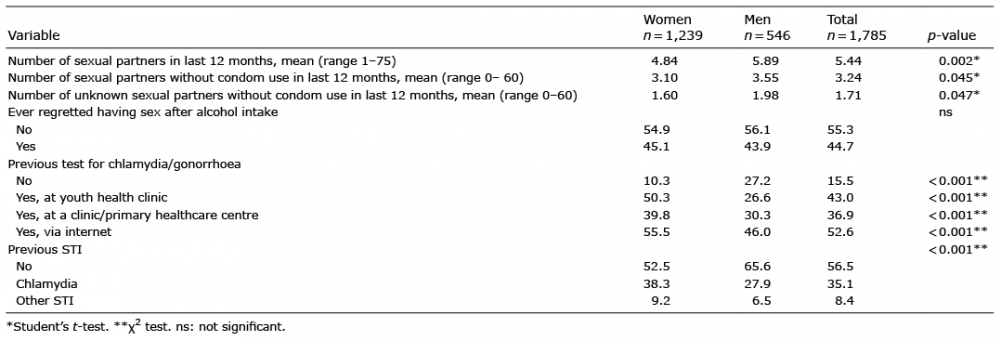 Click to show fullsize
Click to show fullsize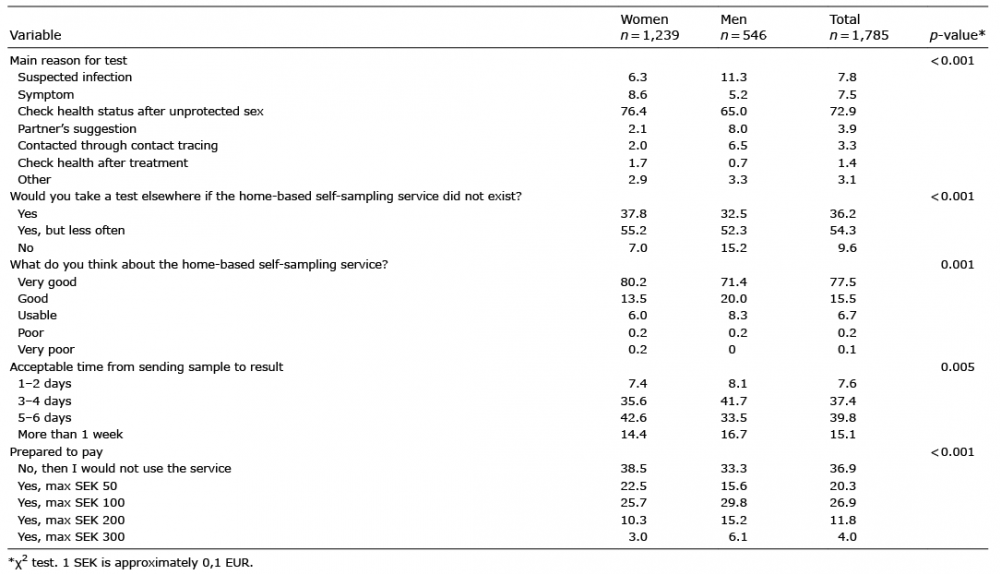 Click to show fullsize
Click to show fullsize