


1Dermatology Department and 3Medical Oncology Department, Hospital Clinic of Barcelona, University of Barcelona, 2Institut d’Investigacions Biomediques August Pi I Sunyer (IDIBAPS), and 4Centro de Investigación Biomédica en Red de Enfermedades Raras CIBERER, Instituto de Salud Carlos III, Barcelona, Spain
#These authors contributed equally to this study.
Given recent developments in the treatment of metastatic melanoma, early detection of disease recurrence is crucial. The aim of this single-centre retrospective cohort study was to investigate the impact of the initial stage of primary melanoma on the pattern and timing of disease recurrence and post-recurrence survival. Patients diagnosed with cutaneous melanoma with initial stage IA–IIID, between January 1996 and December 2018 and who developed disease recurrence until May 2019 were included (n = 784). Earlier stage at diagnosis was associated with a higher proportion of locoregional and a lower proportion of distant metastasis (p = 0.01). The median time to first metastasis decreased with the more advanced stages at initial diagnosis: 3.32 years (interquartile range (IQR) 1.72–6.14 years) for stage I, 1.85 years (IQR 0.99–3.78 years) for stage II and 1.19 years (IQR 0.70–2.42 years) for stage III disease (p < 0.001). These findings add evidence that American Joint Committee on Cancer stages at initial diagnosis of melanoma play a key role in the pattern and timing of disease recurrence and may be helpful to improve surveillance strategies in the follow-up of patients with melanoma.
Key words: melanoma; follow-up studies; cutaneous malignant; disease progression; recurrence; metastasis; survival.
Accepted Apr 19, 2021; Epub ahead of print May 18, 2021
Acta Derm Venereol 2021; 101: adv00502.
doi: 10.2340/00015555-3832
Corr: Susana Puig, Melanoma Unit, Dermatology Department, Hospital Clinic Barcelona, Villarroel 170, ES-08036, Barcelona, Spain. Email: susipuig@gmail.com
This study investigated the role of initial American Joint Committee on Cancer stage on the pattern and timing of first disease recurrence in a large cohort of patients with cutaneous melanoma. Earlier stage at initial diagnosis was associated with a higher proportion of locoregional metastasis and a longer time to first disease recurrence compared with more advanced stages. As stage I patients develop distant metastasis especially late, they may require longer follow-up periods with adequate protocols.
Cutaneous melanoma is a highly aggressive malignancy, which accounts for the majority of skin cancer-related deaths (1). In the USA, cutaneous melanoma is the 5th leading cancer in both men and women, and its incidence continues to increase in most white populations worldwide, as the greatest burden from melanoma falls on Australasian, North American and European populations (2, 3).
At the time of diagnosis, approximately 85% of patients have localized disease, 10% have regional metastatic disease, and 5% have distant metastatic disease (4). Although only a small subset of patients with melanoma present with metastatic disease at initial diagnosis, almost one-third of patients will eventually develop metastasis through disease progression (5). The development of melanoma metastasis has been proposed to occur via 3 main pathways: (i) intralymphatic metastasis (including satellite and in-transit metastasis), (ii) regional lymph node metastasis, and (iii) distant metastasis (6). In general, approximately half of melanoma patients with tumour progression develop regional lymph node metastasis, approximately 25–30% develop distant metastasis and the remaining 20–25% develop satellite/in-transit metastasis as a first manifestation of recurrence (6, 7). Although many studies have identified risk factors for developing disease relapse, the factors that influence the pattern and timing of first recurrence remain unclear. However, this is of special importance, as an early diagnosis can increase the probability of curative treatment and improve survival in the era of targeted therapies and immunotherapies for melanoma.
This study evaluates the associations of initial melanoma stage with pattern and timing of disease recurrence and post-recurrence survival.
Study population
Between January 1996 and December 2018, 3,784 patients with cutaneous invasive melanoma were visited in the Melanoma Unit of Hospital Clinic of Barcelona. Only patients with invasive cutaneous melanoma presenting with stage IA–IIID at primary diagnosis and developing disease recurrence until May 2019 were included in the current analyses.
All primary tumours were re-staged according to the 8th edition of the American Joint Committee on Cancer (AJCC) staging manual (8). When pathological staging was not available (where sentinel lymph node biopsy (SLNB) was not performed due to advanced age, comorbidities, patient refusal, etc.), clinical staging was used. Patients with known distant metastasis at the time of the initial diagnosis (n = 33) and with missing relevant staging information (n = 45) were excluded. After application of exclusion criteria, out of the remaining 3,706 patients with invasive cutaneous melanoma, 784 developed disease recurrence and could be included in the analyses. For patients with multiple primary melanomas, the most invasive tumour according to Breslow thickness was included in the analyses, as it was presumed responsible for the development of metastasis (9).
Patient follow-up was performed according to the standardized intensive protocol (9, 10) and is shown in Table SI. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines for the conduct and reporting of this observational study were followed (11).
Study variables and data collection
From our database and electronic medical records, information was obtained on clinical characteristics and histopathological features, including sex, age, Fitzpatrick skin phototype, anatomical location of the tumour, tumour subtype, Breslow thickness, ulceration, mitotic index, lymphovascular invasion, neurotropism, predominant cell type and microsatellitosis. Breslow thickness and mitotic index were used as continuous variables.
The primary outcome measured was time to recurrence, calculated from the time of excision of the primary tumour to the time of local, regional lymphatic, or distant recurrence. The secondary outcome was post-recurrence melanoma-specific survival, which was calculated from the time of recurrence to the time of last follow-up or death from melanoma.
Patterns of disease recurrence
In the current study, disease progression was categorized into 3 different metastatic patterns at first recurrence: (i) locoregional metastasis, (ii) distant metastasis, and (iii) mixed metastasis, a combination of the two. All metastases were confirmed by relevant imaging studies and/or histological examination. Locoregional metastasis included local recurrences, satellite and in-transit metastases and regional lymph node metastases. The regional lymph node areas that were considered were: ipsilateral axillary group for upper limb melanoma, ipsilateral inguinal group for lower limb melanoma, bilateral cervical and supraclavicular groups for head and neck melanoma, and bilateral axillary and inguinal groups for trunk melanoma. All other types of lymph node metastasis were considered to be distant. Mixed metastases were defined as detection of both locoregional and distant metastases synchronously within a 3-month interval from the first recurrence.
Statistical analysis
Differences between AJCC stages, metastatic patterns and independent variables were calculated as follows. Pearson’s χ2 test and trend test for ordinal variables were used to compare categorical and ordinal variables, respectively. For continuous variables, the Wilcoxon test was used for comparison between 2 groups of samples and Kruskal–Wallis test for comparing multiple groups.
Survival curves based on Kaplan–Meier methods were used to investigate differences in post-recurrence melanoma-specific survival (MSS) for AJCC staging (classified as Stage I, Stage II and Stage III) and according to the pattern of relapse. Curves were calculated using the “survfit” function in the “survival” package and plotted with the “survminer” package in r. To test for a significant difference in outcome between the 3 AJCC stages, a log-rank test was performed using the “survminer” package in computing enviroment R version 4.0.0.
Multivariable survival analyses were performed using Cox’s proportional hazards model. Models were fitted using the “coxph” function in the “survival” package in r. Hazard ratio estimates were calculated for the effect of AJCC stages on MSS, adjusted for age at diagnosis, sex, and type of metastasis. No missing data were present for the latter variables; therefore, no imputation methods or deletions were necessary to implement this model. A regression table for univariable and multivariable hazard ratios was calculated with the “finalfit” package in r.
All statistical analyses were performed using the computing environment R version 4.0.0 and RStudio (12, 13).
Clinicopathological characteristics of the cohort
In the melanoma database of our hospital, 3,786 patients with cutaneous invasive melanoma were registered with a median follow-up of 6.89 years (interquartile range (IQR) 2.91–12.16). Of these, 3,786 patients, 2,287 had initial stage I, 773 had initial stage II, 648 had initial stage III, and 33 had initial stage IV disease. Forty-five patients did not have relevant staging information. During the study period, only 157 (4.2%) patients were lost to follow-up.
After application of inclusion and exclusion criteria a total of 784 melanoma patients with disease recurrence were included in the study cohort. Clinicopathological characteristics of the population are summarized in Table I. The majority of the study cohort (99%) were Caucasian patients of European origin. The mean age of onset was 54.1 years, and the majority of patients were men (57.9% male vs 42.1% female). Of the 784 patients who developed disease recurrence, 171 (21.8%) patients presented with initial stage I, 260 (33.2%) with stage II and 353 (45%) with stage III disease. A further substage distribution of the metastatic patients is shown in Fig. S1. Low-risk melanoma patients from stage IA to IIA make up a large proportion of all metastatic patients (33.3%).
Table I. Baseline characteristics of the cohort stratified by initial stage at diagnosis
Of the patients who developed metastases, 393 (50.1%) developed locoregional metastases alone, 293 (37.4%) developed distant metastases alone, and 98 (12.5%) developed mixed metastases as the first site of tumour recurrence. Earlier stages at the initial diagnosis were associated with a higher proportion of locoregional metastasis and a lower proportion of distant metastasis at the first relapse (p = 0.01). Mixed type recurrence frequency was relatively similar among all stages (Fig. 1).
Fig. 1. Distribution of different patterns of first recurrence according to initial American Joint Committee on Cancer stage at diagnosis.
Timing of disease recurrence
Overall, the median disease-free interval after the diagnosis of primary melanoma to development of the first recurrence was 1.77 years (IQR 0.88–3.46 years). Locoregional metastasis manifested earlier than the distant and mixed type of metastasis, with a median period of 1.46 years (IQR 0.88–3.11) compared with 2.13 (IQR 0.91–3.87) and 2.07 (IQR 0.86–3.71) years, respectively (p = 0.048) (Table II).
Table II. Time in years to first recurrence after the diagnosis of primary melanoma
The median disease-free interval decreased with more advanced AJCC stage (p < 0.001). It was 3.32 years (IQR 1.72–6.14) for patients with initial stage I disease, 1.85 years (IQR 0.99–3.78) for patients with initial stage II disease and 1.19 years (IQR 0.70–2.42) for patients with initial stage III disease (Fig. 2).
Fig. 2. Time in years to develop first recurrence after primary diagnosis. (A) Box plot of initial stages stratified by metastatic patterns: earlier stage at initial diagnosis is related to a longer disease-free interval until development of each different kind of first recurrence. (B) Density plot of initial stages stratified by metastatic patterns: density curves of stage III patients show a peak early in the disease course as the majority of patients relapse within 2 years of diagnosis, while density curves of stage I patients shows a relatively uniform distribution over time. In (B) only the first 10 years after primary diagnosis was shown for a better graphical visualization, but all the metastatic patients were included in the analyses. **p < 0.05 (Wilcoxon test). ns: statistically non-significant.
The box plots in Fig. 2A and the density plot in Fig. 2B show the relationship between disease-free interval and initial stages of melanoma, stratified by different metastatic patterns. The median disease-free interval was longer in patients with stage I disease than in patients with stage II or stage III disease for each kind of metastatic pattern (p < 0.001). Stage I patients developed distant metastasis especially late, with a median period of 4.77 years (IQR 3.33–7.64), compared with 2.60 (IQR 1.40–3.94) for stage II and 1.23 (IQR 0.61–2.48) for stage III patients (p < 0.001) (Table II).
Post-recurrence survival analysis
Post-recurrence melanoma-specific survival analysis of patients, stratified by initial stage of melanoma and the pattern of disease recurrence, demonstrated significant differences among the groups. Patients diagnosed with stage I melanoma showed better post-recurrence MSS (2.42 years) than patients diagnosed with stage II or III disease (post-recurrence MSS 2.27 and 1.70 years, respectively) (p = 0.025) (Fig. 3). While median post-recurrence MSS was similar between distant and mixed type of metastasis (0.98 and 0.91 years, respectively), patients with locoregional metastasis alone had a better post-recurrence MSS with 4.48 years (p < 0.001) (Fig. 3).
Fig. 3. Kaplan–Meier curves of post-recurrence melanoma specific survival according to the initial stage at diagnosis and metastatic pattern. Below the x-axis is displayed the number of patients at risk at each 2.5-year interval. AJCC: American Joint Committee on Cancer.
Factors associated with post-recurrence MSS were explored in univariable and multivariable analyses (Table III). Initial stage at diagnosis, sex and primary tumour location were not of prognostic significance on multivariable analyses. Distant or mixed type of metastasis had a negative prognostic significance for post-recurrence MSS compared with the locoregional metastasis. Later-age at onset was associated with a shorter post-recurrence MSS, even though this association was only statically significant for the oldest quartile of patients (> 72 years) compared with the youngest quartile (< 45 years) (hazard ratio (HR) 1.49. 95% CI 1.13–1.97, p = 0.005).
Table III. Univariable and multivariable Cox regression analysis of post-recurrence melanoma-specific survival
This cohort study suggests that the initial staging at melanoma diagnosis has a profound impact on the pattern of disease recurrence, timing of recurrence and post-recurrence survival. Although some studies have analysed different patterns of disease recurrence, timing of recurrence and post-recurrence survival in patients with metastatic melanoma, many of them include only a limited number of patients.
In this study, we observed that the pattern distribution of the first metastasis was different across the initial stages. A more advanced stage at initial diagnosis was associated with a higher proportion of distant metastasis and lower proportion of locoregional metastasis. These findings were in concordance with the study by Tas et al. (14), which showed that locoregional metastasis was predominant in stage I–II patients, whereas the majority of stage III patients developed distant or mixed type metastasis as the first site of relapse. In 2 different studies from the Memorial Sloan Kettering Cancer Center that analysed metastatic patterns of initial stage II and stage III patients by substage, it was further demonstrated that more advanced substages were more likely to relapse at distant sites than locoregional sites (15, 16). There is no specific explanation for this finding, but previous lymph node dissection in stage III patients could be one reason for lower percentages of locoregional metastasis in this group of patients. Another interesting explanation could be the specific anatomical and structural differences between lymphatic and blood vasculature of dermis. Similar to blood vessels, lymphatic vessels are situated immediately below the epidermis, but lymphatics generally possess a wider and more irregular lumen, and a thinner vessel wall than blood capillaries. Furthermore, they have a poorly developed basal lamina and no tight junctions, which can ease lymphatic invasion even for thinner melanomas (17, 18).
The current study showed that the timing of recurrence varies according to different metastatic patterns and different initial stages. Distant metastasis and mixed type metastasis had a similar median time to disease recurrence, and they occurred later than locoregional metastasis. Furthermore, patients with earlier stages at diagnosis developed metastasis later than those at more advanced stages. This difference was particularly evident for the distant metastasis, where median disease-free interval until relapse was 4.8 years in patients with stage I disease, compared with 1.4 years in patients with stage III disease. A similar finding was previously reported in another cohort study, in which median time to distant relapse was markedly longer in patients with stage I–II melanomas than stage III melanomas (14). In a recent study from Australia, the authors reported that, for melanomas < 1 mm of Breslow, most deaths occurred between 5 and 20 years after diagnosis, whereas for thicker melanomas most deaths occurred within the first 5 years (19). Although the reason why tumour recurrence of stage I melanomas develops later than advanced stages is still not known, one can assume that primary tumour biological and molecular characteristics play a key role. Tumour dormancy is a well-recognized clinical phenomenon for some types of cancers including melanoma, in which disseminated tumour cells remain occult and asymptomatic over a prolonged period of time before they contribute to disease recurrence at distant sites, and early-stage melanomas are exhibiting this phenomenon more often (20–22). However, one should interpret these results with care to avoid potential bias: It seems true that melanoma patients with late recurrence usually had an early-stage melanoma at initial diagnosis, because a high percentage of patients with more advanced stages are expected to be lost already due to their apparently lower 5-year survival rates. Novel adjuvant therapies for high-risk melanoma patients might postpone the timing of first recurrence for this group of patients, and this requires further study.
The type of first recurrence has been shown to be an important prognostic factor for post-recurrence survival. As was to be expected and has been described in previous studies, patients with locoregional metastasis had a longer post-recurrence survival than patients with distant or mixed metastasis (23–25). Although the median post-recurrence MSS was somewhat shorter for patients with mixed metastasis than with distant metastasis (possibly as a result of a higher tumour burden), the Kaplan–Meier curves overlapped. In the current study, the initial stage at diagnosis was also found to impact survival after disease recurrence. Initial diagnosis of stage II and stage III melanoma was associated with significantly worse post-recurrence MSS compared with an initial diagnosis of stage I disease. However, in the multivariable analysis after adjusting for type of first recurrence, age, sex and primary tumour location, its prognostic significance was lost. These findings suggest that the survival benefit of initial stage I melanomas is driven by the fact of their developing locoregional metastasis more frequently compared with more advanced stage melanomas. The current study was not able to revalidate the findings from a recent study, which included only patients with distant metastasis and concluded that, even after controlling for metastatic organ and serum LDH level, initial diagnosis of stage II and stage III melanoma was associated with significantly worse post-recurrence overall survival compared with stage I (26).
There is a widespread perception that the majority of melanoma metastases result from advanced melanomas at initial staging. However, melanomas diagnosed at an early stage, account for a substantial number of patients who relapse and die from melanoma. In our cohort, 33.3 % of all metastatic patients had an initial stage IA–IIA melanoma, increasing to 53.8% if we also include patients with stage IIB and IIC, defined as a low-risk group and do not require intensive surveillance with imaging studies or adjuvant treatment according to many guidelines (27–29). This fact supports the view that there are early melanomas with a biologic propensity to metastasize that are currently not being identified by classical risk factors (30, 31). The recent development of commercial gene expression profile (GEP) tests, based on the molecular characteristics of the tumour, may help clinicians predict the metastatic risk of each primary tumour more accurately, especially at early stages (32–35). Once the risk is further stratified by these tests, adequate follow-up strategies can be determined. As the current study shows that early-stage melanomas develop metastasis relatively late, an intensive follow-up with radiological examinations beyond 5 years may be neither rational nor cost-effective. In the future, non-invasive blood genomic marker assays (liquid biopsies) may be of benefit if implemented in follow-up protocols of early-stage melanoma patients with a high risk of metastasis. Those tests might allow dynamic disease evaluation over a sequential time-frame and provide the potential benefit of detecting disease recurrence before it becomes clinically evident (36, 37).
This study has some limitations. First, pathological staging of some patients could not be obtained because they did not undergo SLNB due to advanced age, comorbidities or patient refusal. In those cases, clinical staging information was used. A lack of initial nodal staging may result in underestimation of the true pathological stage, but those patients represented a relatively small subset of the total number. Secondly, owing to long study period, treatment modalities and adjuvant treatment indications have changed over time, which may have affected metastatic patterns, but we were unable to separately investigate the role of immunotherapy or targeted therapy on those patterns. On the other hand, the study is strengthened by the prospective collection of data, standardized long follow-up examinations, and by the large sample size of metastatic patients.
We thank our patients and their families who are the main reason for our studies; nurses from the Melanoma Unit of Hospital Clínic of Barcelona: Daniel Gabriel, Mireia Domínguez, Pablo Iglesias and Maria E Moliner for helping to collect patient data; and Paul Hetherington English-language editing.
The study in the Melanoma Unit, Hospital Clínic, Barcelona was supported, in part, by grants from Fondo de Investigaciones Sanitarias P.I. 12/00840, PI15/00956 and 15/00716 Spain; by the CIBER de Enfermedades Raras of the Instituto de Salud Carlos III, Spain, co-funded by “Fondo Europeo de Desarrollo Regional (FEDER). Unión Europea. Una manera de hacer Europa”; by the AGAUR 2009 SGR 1337 and AGAUR 2014_SGR_603 of the Catalan Government, Spain; by a grant from “Fundació La Marató de TV3, 201331-30”, Catalonia, Spain; by the European Commission under the 6th Framework Programme, Contract nº: LSHC-CT-2006-018702 (GenoMEL); by CERCA Programme/Generalitat de Catalunya and by a Research Grant from Asociación Española Contra el Cáncer. CERCA Programme/Generalitat de Catalunya.
Sumeyre Seda Ertekin received a research grant from Turkish Society of Dermatology
The sponsors had no role in the design and conduct of the study; in the collection, analysis, and interpretation of data; or in the preparation, review, or approval of the manuscript.
Research protocol received approval from the Research Ethics Committee of the Hospital Clinic of Barcelona (IRB number: HCB/2015/0298).
The authors have no conflicts of interest to declare


 Click to show fullsize
Click to show fullsize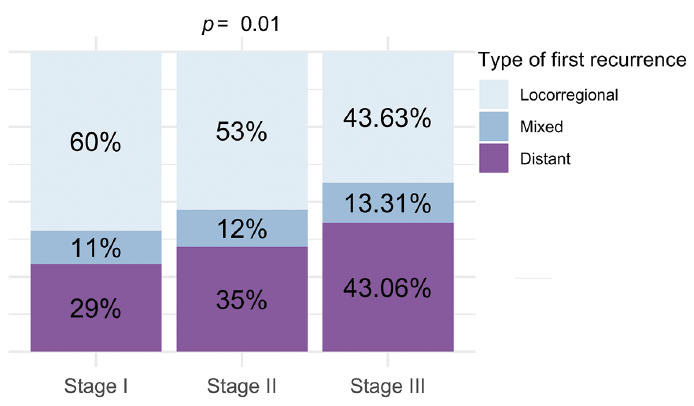 Click to show fullsize
Click to show fullsize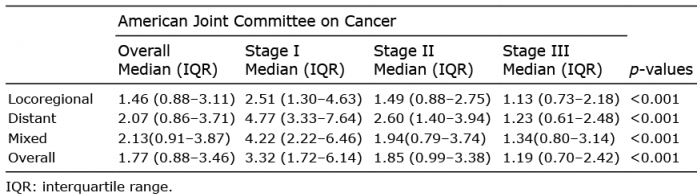 Click to show fullsize
Click to show fullsize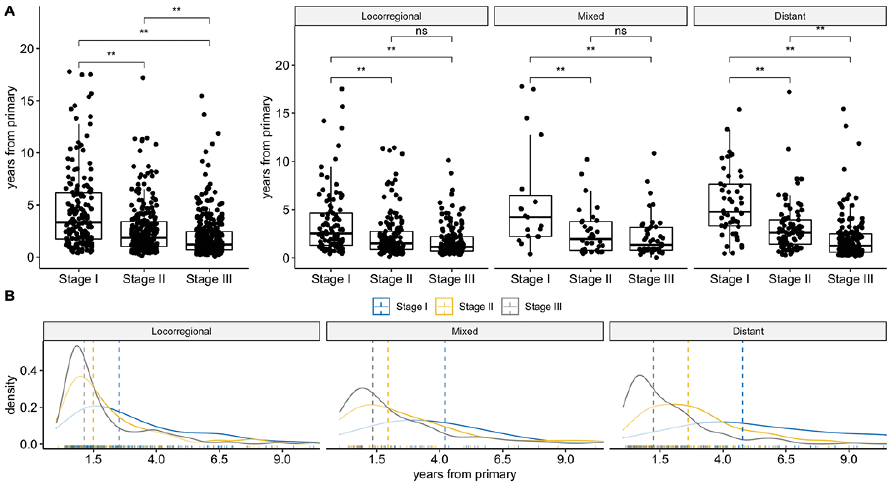 Click to show fullsize
Click to show fullsize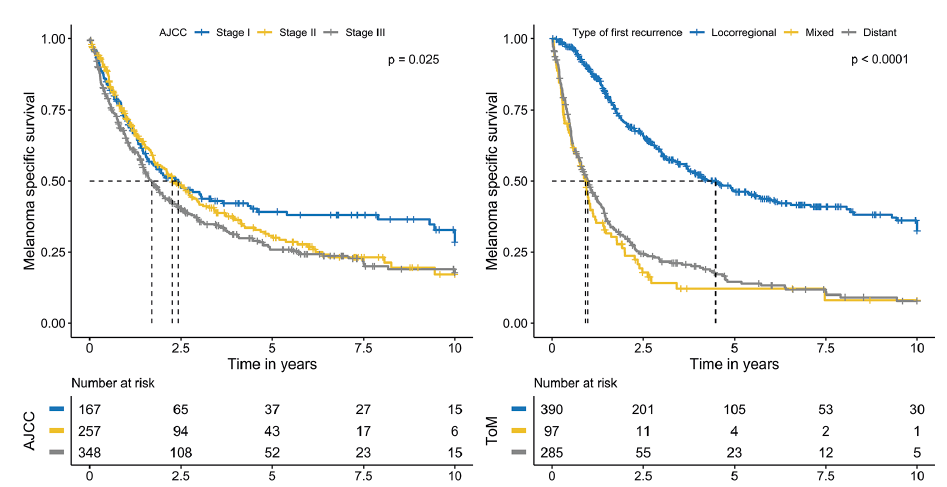 Click to show fullsize
Click to show fullsize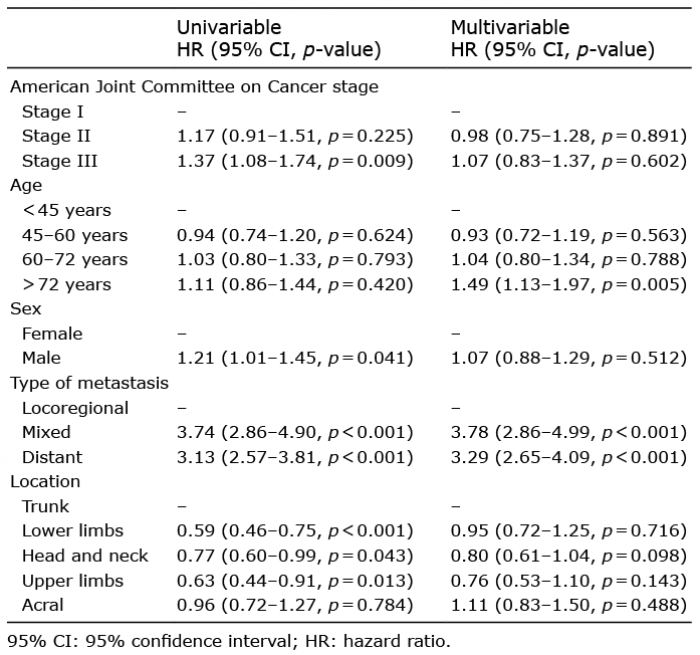 Click to show fullsize
Click to show fullsize