


1Department of Dermatology, Venereology and Allergology and 2Department of Hematology, Cell Therapy and Hemostaseology, University Medical Center Leipzig, Philipp Rosenthal Straße 23, DE-04107 Leipzig, Germany. E-mail: Benjamin.klein@medizin.uni-leipzig.de
A 56-year-old man presented to our dermatology department with petechial purpura on the lower legs (Fig. 1). One week previously he had had fever for 3 days (39°C), which resolved without therapy. Skin examination revealed non-palpable petechiae. Neither mucosal nor conjunctival haemorrhages were observed. Systemic examination revealed pressure pain in the left upper quadrant. The spleen was not enlarged. Laboratory analysis including complete blood count with differential revealed severe thrombocytopenia with a total platelet count of 1 Gpt/l (150–350 Gpt/l), which was confirmed in a citrate-buffered blood sample. The patient showed a leukocytosis (total 12.3 Gpt/l with neutrophilia, no microscopic changes in favour of leukaemia). Additional laboratory results, including liver enzymes, kidney parameters, lactate dehydrogenase and anti-neutrophil cytoplasmic antibodies were within normal ranges, and a SARS-CoV-2 smear (PCR test) was negative.
Serological results revealed primary HIV-infection (p24-antigen-positive) with a total CD4-cell count of 532, reduced CD4/CD8 ratio (0.3) and a viral load of 2.5 million copies/ml, hence stadium B1 of center of disease control - classification. Furthermore, the patient showed reinfection with syphilis, with TPPA 1:40960 and RPR 1:32, after being treated for syphilis 10 years previously. In addition, a seroconverted hepatitis B infection was detected. Serological results for hepatitis C virus, human herpes virus 6, cytomegaly virus and Epstein-Barr virus as well as screening for Chlamydia trachomatis, Neisseria gonorrhoeae and anogenital warts, were unsuspicious or negative.
What is your diagnosis? See next page for answer.
Fig. 1. Petechial purpura on the lower legs in a 56-year-old man. The patient has given written informed consent to publication of the case details.
Acta Derm Venereol 2021; 101: adv00530.
Diagnosis: Secondary immune thrombocytopenia due to primary HIV infection
The patient showed severe thrombocytopenia without any signs of internal bleeding. Under suspicion of secondary immune thrombocytopenia (ITP), he was first treated with systemic steroids (prednisolone 0.5 mg/kg body weight), which lead to increase in thrombocytes to 60 Gpt/l (Fig. 2). Together with our department of haematology, we diagnosed secondary ITP due to primary HIV infection (1). The patient received combined antiretroviral therapy (cART), consisting of bictegravir, emtricitabine and tenofovir-alafenamide, which led to normalization of total thrombocyte count (Fig. 2) and disappearance of purpuric lesions. Co-infection of syphilis was treated with i.m. benzathine-benzylpenicillin.
Secondary ITP represents a common clinical feature in HIV infection, which was previously described in the 1980s with an incidence of 10–30% (2). Clinical prevalence is increasing with viral load and decreasing after administration of antiviral therapy (3), as seen in our patient. Severe ITP, with a total platelet count < 10 Gpt/l was found in 0.6% of HIV-positive patients (4). In primary HIV infection, ITP is suspected to be caused by molecular mimicry of antiviral antibodies against platelet factors glycoprotein IIa and IIIb, inducing a complement-independent destruction of platelets (5, 6). Mechanisms in progressed stages include infection of megakaryocyte bone marrow-dependent progenitor cells (7, 8). Coinfection of syphilis is more frequently observed in patients with primary HIV infection. Under immunosuppression, primary syphilis manifestations can be atypical with multiple chancres or longer persistence of the lesion (9). In the current case, the patient showed serological reactivation of syphilis. Given the high prevalence of other sexually transmitted diseases (STDs) in primary HIV infection, standardized STD screening (including examination of human papillomavirus-associated skin and mucosal lesions) should be performed (10).
Other causes of secondary ITP include different viral infections (e.g. HCV, EBV, CMV), lymphoproliferative disorders (e.g. chronic lymphoid leukaemia), immunodeficiency syndromes and autoimmune diseases (e.g. systemic lupus erythematodes, rheumatoid arthritis) (8).
Petechial purpura represents a common dermatological feature, which can be classified into palpable and non-palpable lesions. The case reported here showed isolated non-palpable petechial purpura of the lower legs. Treatment of secondary ITP in HIV is realized by application of systemic steroids and antiviral therapy (4, 8), as seen in this patient. Platelet concentrates are not the first-line recommendation (4). The current case illustrates the clinical sign of non-palpable petechial purpura due to secondary ITP in primary HIV infection, which should be considered in differential diagnosis of purpura.
Fig. 2. Dynamics of thrombocytes during treatment. Severe thrombocytopenia was present at the time of consultation in our department, which increased to 60 Gpt/l after application of prednisolone, and normalized on commencement of combined antiretroviral therapy (cART).


 Click to show fullsize
Click to show fullsize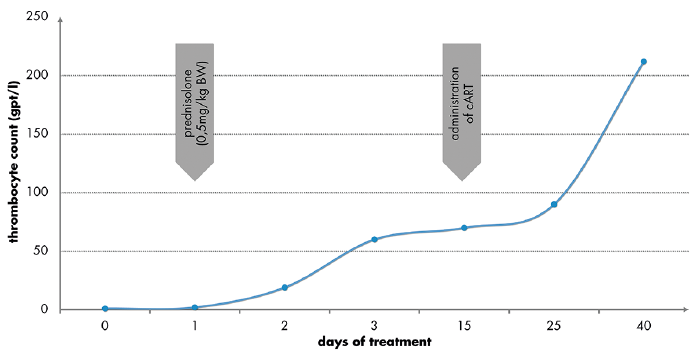 Click to show fullsize
Click to show fullsize