


1Department of Infectious Diseases and Dermatology, Saint-Pierre University Hospital, 2Inserm-CIC-1410, Saint-Pierre University Hospital, La Réunion, France, 3Photodermatology and Vitiligo Treatment Centre, Israelite Hospital, Rome, Italy, 4Department of Adult and Pediatric Dermatology, Bordeaux University Hospital, Bordeaux, 5Laboratoires Genevrier, Clinical Research Department, Antibes, 6Dermatological Institute, Paris, 7Department of Dermatology, Le Mans Hospital, Le Mans, France and 8Department of Dermatology, Ghent University Hospital, Ghent, Belgium
The aim of this study was to assess the efficacy of non-cultured autologous epidermal cell grafting resuspended in hyaluronic acid, performed using a ready-to-use kit, compared with hyaluronic acid alone (neutral comparator) for repigmenting vitiligo and piebaldism lesions at 6 months. Two identified paired lesions per patient were randomized to be treated by either device. Devices with a ready-to-use kit were prepared by separate health professionals, to maintain blinding. A skin biopsy was digested using trypsin, and cells resuspended in hyaluronic acid solution. Among 38 patients screened, 36 (94.7%) patients, corresponding to 72 lesions, were analysed. For difficult-to-treat lesions, defined as those located on the wrist, elbow, and hands (n = 30), no repigmentation ≥ 50% was observed. For all other locations (n = 42), the success rate was significantly higher (p = 0.021) in the ready-to-use kit group (47.6% vs 9.5%) at 6 months and was maintained until 12 months. In conclusion, a single application of non-cultured epidermal cellular grafting using a ready-to-use kit was efficient at 6 months and at 1-year follow-up.
Key words: non-cultured epidermal cells; autologous grafting; repigmentation; leukoderma; vitiligo; piebaldism.
Accepted Jul 6, 2021; Epub ahead of print Jul 7, 2021
Acta Derm Venereol 2021; 101: adv00506.
doi: 10.2340/00015555-3870
Corr: Antoine Bertolotti, Department of Infectious Diseases and Dermatology, Saint-Pierre University Hospital, 97 Avenue du Président Mitterrand, La Réunion, France. E-mail: antoine_bertolotti@yahoo.fr
A ready-to-use kit, Viticell® (CE 0344, Laboratoires Genevrier, France), has been developed to facilitate non-cultured epidermal autologous cellular grafting and was assessed in a multicentre, multinational, double-blinded, randomized, neutral comparator (hyaluronic acid 2%)-controlled study. Grafting performed with this ready-to-use kit was shown to be an effective treatment for repigmentation of stable vitiligo and piebaldism lesions, over a 12-month follow up.
Leukoderma, manifesting as achromic macules, is a loss or decrease in skin pigmentation mostly due to a substantial loss of melanocytes. Due to its aesthetic impact, leukoderma can severely affect the patient’s quality of life, leading to psychological damage and social repercussions (1, 2). This study concerns vitiligo, which affects 0.5–1% of the population worldwide (3, 4) and the rare dominantly inherited disease piebaldism (the exact prevalence of which is unknown, but the incidence is estimated at 1 in 20,000 births) (5). Currently, the usual treatment for vitiligo combines phototherapy and topical anti-inflammatory drugs. For patients who do not respond to treatment, autologous epidermal cell suspension is a good therapeutic approach for segmental vitiligo and, more rarely, for stable generalized (non-segmental) vitiligo. For piebaldism, there is no available medical therapy, and autologous cell grafting is considered an excellent option (6). Autologous cell grafting consists of isolating autologous epidermal cells from a superficial biopsy, followed by their application to a dermabraded lesion. The method was developed by Gauthier & Surleve-Bazeille (7) and improved by others, in particular van Geel et al. (8). The importance of the presence of hair follicles in the donor area was emphasized in the original report (7) using scalp skin. Other physicians use pubis skin, but the majority prefer, for the sake of simplicity of the procedure, to sample the gluteal region. A ready-to-use (RTU) kit using autologous cells resuspended in hyaluronic acid CE-marked (Viticell®, CE 0344, Laboratoires Genevrier, France) was developed in order to provide doctors (e.g. dermatologists, plastic surgeons, etc.) with a simplified all-in-one medical device to perform the grafting in less than 2 h. The RTU kit is a single-use, stand-alone device for preparing a cell suspension. It comprises an enzymatic solution (10 ml amber bottle containing 25 mg trypsin), digestion, rinsing and preparation sterile solutions (3 syringes pre-filled with phosphate-buffered saline (PBS)), application sterile solution (1.5 ml pre-filled syringe containing 30 mg hyaluronic acid in a saline solution (HA 2%)), a portable instant heat pack with sodium acetate saturated solution (heat through crystallization) and devices such as Petri dish and needle (9).
The objective of this study was to compare the efficacy of non-cultured epidermal cellular grafting using the RTU kit with a non-cellular comparator in vitiligo and piebaldism.
Trial design
The study was an interventional, multicentric, international, prospective, randomized (1/1 ratio), double-blind, controlled, phase III clinical trial evaluating the efficacy and safety of autologous epidermal cell suspension grafting using RTU kit on patients for stable vitiligo or piebaldism, compared with a neutral comparator: HA 2% alone. The patients in this study are their own controls, since they received both treatments on 2 identified separate lesions.
Outcomes
The primary efficacy endpoint was the success of repigmentation at month 6, defined as at least 50% repigmentation of the treated area. Repigmentation was clinically assessed by physical examination of the patient by the investigator. Repigmentation is defined as a colouration (restoration of the original skin colour) of white patches. Wood lamp (ultraviolet (UV) radiation) could allow a more precise delimitation between white and coloured area.
Secondary endpoints were: (i) success of repigmentation at month 12, (ii) variation in repigmentation (percentage) between inclusion and each follow-up visit: 3, 6, 9 and 12 months after grafting (M3, M6, M9 and M12), (iii) patients’ and doctors’ satisfaction using a 5-point Likert scale ranging from 1 to 5 (1: Not at all satisfied/2: Slightly satisfied/3: Moderately satisfied/4: Very satisfied/5: Extremely satisfied) (10), and (iv) colour-matching using natural light (hypopigmented, hyperpigmented, normally pigmented skin) compared with surrounding skin. The baseline value was the lesion size at the time of the inclusion visit. Lesions were measured by investigators at each visit using tracing paper or transparent sheets.
Safety parameters were assessed as adverse events (AEs) and clinical examination (vital signs).
Participants
The study was conducted at 5 sites in Europe (1 site in Belgium, 1 site in Italy and 3 sites in France). To be eligible, all patients had to comply with the following inclusion criteria: (i) patients aged over 18 years with a diagnosis of non-scarring leukoderma, stable over the last year (non-segmental vitiligo, segmental vitiligo or piebaldism), (ii) lesion size of at least 1 cm2, (iii) minimum distance of 2 cm between 2 lesion areas and to normal pigmented skin of at least 0.5 cm, (iv) for vitiligo, documented medical treatment failure in the last 6 months, (v) absence of infected lesions, (vi) negative serology (HIV, HBV, HCV, syphilis), (vii) washout of 1 month for topical treatments and 3 months for phototherapy.
Exclusion criteria were: hypersensitivity to local anaesthetics or 1 of the components of the resuspension medium (trypsin, HA); contraindication of biopsy; patient with a history of melanoma; herpes if present on the day of treatment in the region to be treated; history of keloidal scars and clinically assessed presence of Koebner’s phenomenon; treatment locations of lesions located on the face, fingers and toes in the case of non-segmental vitiligo; pregnant or lactating women.
This study was conducted in accordance with the Declaration of Helsinki and reviewed favourably by the local ethics committees of France (CPP Sud-Ouest III), Italy (Comitato Etico Centrale IRCCS Lazio) and Belgium (Commissie Voor Medische Ethiek). Written informed consent was collected for all patients during the screening visit before any intervention and data collection.
Interventions
For each patient, 2 lesions or 1 lesion divided into 2 areas were identified measured and randomized, 1 for receiving RTU kit and 1 for receiving the neutral comparator (D0). The cells collection and preparation were standardized. A thin-skin biopsy, 0.2–0.3 mm thick and 4–10 cm² in area, was collected from normally pigmented skin (the location was chosen at the investigator’s discretion), using a dermatome after cleaning the donor site with an antiseptic solution, and rinsed with a sterile saline solution. The biopsy donor site was determined according to the surface area to be treated (the recommended ratio is 5 times the size of the biopsy), and local anaesthetic could be used. Skin biopsy was then digested using enzymatic digestion (37°C for 30 min) and cells collected and resuspended in a HA solution (2% in 1.5 ml). HA 2% alone was used as the comparator. Both selected lesions to be treated were dermabraded using a carbon dioxide laser (parameters at the investigator’s discretion, e.g. 2 W in continuous mode). The suspension and HA alone were then applied on the dermabraded areas as an outpatient procedure and a dressing (using Mepitel Film® or Mepitel® and, subsequently, Tegaderm®) was applied to each lesion and left for 6 days.
A visit was made 6/7 days after the procedure to remove the dressing and for evaluation of safety. Lesions were assessed at 3, 6, 9 and 12 months after grafting (M3, M6, M9 and M12) and a written satisfaction questionnaire was answered by patients and doctors at M12.
Randomization
A randomization list was generated by the statistician in blocks of 4 in a ratio of 1:1 for each type of vitiligo, using SAS V9.4 software (Copyright © SAS Institute Inc., SAS Campus Drive, Cary, NC, USA. All rights reserved). before the start of the study and stored in electronic format (Excel file). RTU kit and comparator were randomly allocated at the first visit (D0) through an Interactive Response Server (IRS): a site staff health professional other than the investigator evaluator sent a request by fax and received an e-mail allocating the treatment to the lesion according to the randomization list.
To ensure the double-blinding procedure, the unblinded health professional prepared suspensions with non-cultured autologous dermal cell using RTU kit and comparator after randomization. Patients and investigator evaluator were blinded.
Sample size
The sample size was calculated for a superiority trial, according to the hypothesis of a bilateral alpha risk = 5% and beta risk = 20%, for a power equal to 80%, a 30% of potential drop-outs and an expected difference in success rate of at least 30% between epidermal cell suspension and neutral comparator. This resulted in the need to include 60 patients in the intent-to-treat (ITT) population. Patients who discontinued the study were not replaced.
Statistical analysis
Statistical analysis was performed with SAS V9.4, and the results are expressed for: (i) quantitative parameters in terms of mean, standard deviation (SD) and were analysed using Student’s paired t-test or Wilcoxon’s signed rank test according to the normality of the distribution, (ii) qualitative parameters in terms of number and percentage of each modality providing 95% confidence interval (95% CI) were analysed using McNemar test (paired data).
Efficacy parameters were analysed globally and according to location (subgroup 1: hand, elbow, wrist; and subgroup 2: all other locations). All statistical analyses were performed at the 0.05 global significance level, using 2sided tests. Missing data regarding the size of the lesion were replaced using the last observation carried forward (LOCF).
The safety population was defined as all patients treated. The ITT population was defined as all the randomized patients with at least 1 evaluation. The per protocol (PP) population included all patients from the ITT population and with no major deviation from the protocol.
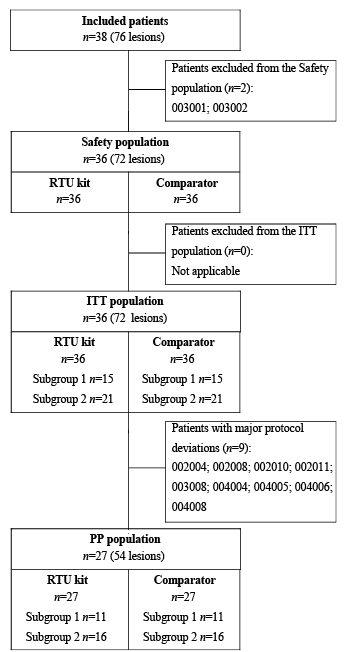
Participant flow
The flow chart of patients included in the study is shown in Fig. 1. A total of 38 patients were recruited to the study from April 2014 to April 2017 and followed until April 2018. Two patients were not randomized; 1 due to patient decision and 1 due to failure of screening. Therefore, the ITT population comprised 36 (94.7%) patients (72 lesions): 36 lesions in the RTU kit group and 36 lesions in the control group. Subgroup 1 (hand, elbow, wrist) comprised 15 (41.7%) patients: 15 lesions in the RTU kit group and 15 lesions in the control group patients; and subgroup 2 (all other locations) comprised 21 (58.3%) patients: 21 lesions in the RTU kit group and 21 lesions in the control group. Thirty-one (86.1%) patients (62 lesions) completed the study: 5 patients withdrew prematurely, 1 patient at visit 2 (D6–7), 1 patient at visit 3 (M3), 2 patients at visit 4 (M6), and 1 patient at visit 5 (M9). Twenty-seven (75%) patients (54 lesions) had at least 1 efficacy assessment available, but with major protocol deviations, and were included in the PP population. No statistically significant difference was observed between RTU kit and the control groups regarding lesion size (Table I). All other parameters were comparable for both groups. On the day of inclusion, patients had a median age of 41 (17–67) years and a median duration of the disease of 19.1 (1.5–49.3) years. Overall, 9 (25.7%) patients had a Fitzpatrick phototype II, 22 (62.9%) patients had a phototype III and 4 (11.4%) patients had a phototype IV (1 missing data). Twenty-three (63.9%) patients had non-segmental vitiligo, 11 (30.6%) had segmental vitiligo and 2 (5.6%) had piebaldism. All patients were in therapeutic failure with their previous therapy (Table I).
Fig. 1. Flow chart of the study participants. RTU: ready-to-use; ITT: intention-to-treat; PP: per protocol.
Table I. Sociodemographic and medical characteristics of the patients at inclusion, intention-to-treat (ITT) population (n = 36)
Outcomes
Primary efficacy outcome. Overall, the success rate of repigmentation at M6 was 27.8% (95% CI 13.1; 42.4) in the RTU kit group, and was significantly higher (p = 0.021) than in the comparator group (5.6%) in the ITT population (Fig. 2). Consistent results were obtained when analysis was performed in the PP population (Table II). There was no repigmentation ≥ 50% at M6 for lesions located in hands, elbow, or wrists in either group. For lesions in other locations (subgroup 2), the success rate of repigmentation at M6 was 47.6% (95% CI 26.3; 69.0) in the RTU kit group and was significantly higher (p = 0.021) than in the comparator group (9.5%). Consistent results were obtained in the PP population (Table II).
Fig. 2. Repigmentation rate at M6 and M12, intention-to-treat. *n = 36 patients, 72 lesions; p = 0.021. **Hands, elbows, wrists: n = 15 patients, 30 lesions; p = not significant. ***All other locations; n = 21 patients, 42 lesions; n = 0.02. M6: 6 months after treatment. M12: 12 months after treatment.
Table II. Repigmentation rate at M6 and M12, intention-to-treat (ITT) population (n = 36 patients, 72 lesions) and per protocol (PP) population (n = 27 patients, 54 lesions)
Secondary efficacy outcomes. Overall, the success rate of repigmentation at M12 was 25.0% (95% CI 10.9; 39.1) in the RTU kit group and was significantly higher (p = 0.020) than in the comparator group (5.6%) in the ITT population and consistent results were obtained in the PP population. For lesions located on hands, wrists and elbows, no repigmentation was observed in either group. For lesions in other locations, the success rate of repigmentation at M12 was 42.9% (95% CI 21.7; 64.0) in the RTU kit group and was significantly higher (p = 0.020) than in the comparator group (9.5%) in the ITT population, with consistent results observed in the PP population (Table II).
For all locations, the reduction in percentage of lesion size appeared rapidly after M3 and was significantly higher in the RTU kit group than in the comparator group for the entire follow-up, except at M9, with a mean percentage reduction (SD) of –15.8 (38.3) vs –1.2 (26.9) at M3 (p = 0.008), –18.5 (42.5) vs –1.3(32.5) at M6 (p = 0.030), –21.2 (42.5) vs –4.6 (32.2) at M9 (p = 0.055), and –20.5 (44.6%) M12 (p = 0.025). For lesions located on hands, wrists and elbows, no significant difference was observed. For lesions in other locations, the size reduction in percentage was rapid to obtain and was significantly higher in the RTU kit group than in the comparator group over the 12-month follow-up, with a mean percentage reduction (SD) of –31.9 (38.1) vs –8.0 (20.6) at M3 (p = 0.013), –38.8 (39.6) vs –9.6 (30.4) at M6 (p = 0.035), –41.3 (40.5) vs –15.0 (32.2) at M9 (p = 0.035), and –41.4 (40.9) vs –13.3 (27.9) M12 (p = 0.015) (Fig. 3).
Fig. 3. (a) Lesion size (cm2), intention-to-treat (ITT). *n = 36 patients, 72 lesions; p= not significant (NS). **Hands, elbows, wrists: n = 15 patients, 30 lesions; p = NS. ***All other locations; n = 21 patients, 42 lesions; p = NS. (b) Size reduction (%), ITT. *n = 36 patients, 72 lesions; p < 0.05 except M9. **Hands, elbows, wrists: n = 15 patients, 30 lesions; p = NS. ***All other locations; n = 21 patients, 42 lesions; p < 0.05.
Overall, 45.2% of patients were slightly satisfied and 29.0% very satisfied or extremely satisfied in the RTU kit group vs 29.0% and 3.2%, respectively, in the comparator group (p=0.01) and 48.4% of investigators were at least slightly satisfied and 25.8% very satisfied or extremely satisfied in the RTU kit group vs 35.5% and 3.2%, respectively, in the comparator group.
At M12, 12 (38.7%) patients in the RTU kit group had good colour matching vs 4 patients (12.9%) in the comparator group (p = 0.005). For lesions located on hands, wrists and elbows no colour matching was reported, whereas for patients treated in other locations, 12 (66.7%) patients in the RTU kit group had good colour matching vs 4 patients (22.2%) in the comparator group (p = 0.005). Pictures of target lesions, treated with RTU kit and comparator, taken at inclusion before treatment, and 6 months after treatment in a patient with non-segmental vitiligo are shown in Fig. 4.
Fig. 4. (a) Photograph of patient with a non-segmental vitiligo, located in the back, treated with (B) ready-to-use (RTU) kit in the left side and (A) comparator in the right side at inclusion visit before treatment (baseline). (b) Picture of patient with a non-segmental vitiligo, located in the back, treated with RTU kit in the left side (B) and comparator in the right side (A) at inclusion visit 6 months after treatment (M6).
Safety
Overall, 46 AEs were experienced by 20 patients in the safety population, all were considered mild or moderate, and 11 (30.6%) were related to the study device. The most frequent AEs were pain, graft complication, post-procedural discharge, wound, and skin disorders (pruritus, folliculitis). All related AEs were considered by investigators to be expected due to the grafting procedure.
In order to facilitate the practice of autografts, the new RTU kit in this study allows a simplified outpatient procedure for grafting epidermal cells without the need for a cell culture facility. This study evaluate the efficacy of an autologous epidermal cell suspension made using the RTU kit compared with a 2% HA solution, in patients with stable segmental or non-segmental vitiligo or piebaldism and related conditions. The study demonstrated a statistically significant higher success rate at 6 months (27.8% vs 5.6%, p = 0.021) and a long-term beneficial effect: persistence at 1 year (25.0% vs 5.6%, p = 0.020) after a single autologous epidermal cell transplant using RTU kit compared with a 2% HA solution. This study also confirms a repigmentation success rate > 47% for the subgroup of patients with lesions all over the body except for the hands, wrists and elbows, which is significant compared with a 2% HA solution (9.5%). Moreover, the repigmentation persisted at 1 year (42.9% vs 9.5%, p = 0.021). Lesion size was reduced rapidly in the RTU kit group compared with the HA group at 3 months (p = 0.013), with an increasing effect at 6 months (p = 0.035) and 9 months (p = 0.035) maintained over 1 year (p = 0.015). This suggests a persistent effect of the graft performed using the RTU kit, with a mean repigmentation rate of more than 75% at 6 months and nearly 80% at 12 months for patients with grafting success. In terms of global satisfaction, the current study showed greater satisfaction of both patients and investigators for lesions treated by a suspension graft of epidermal cells using the RTU kit compared with a 2% HA solution. Overall, autologous epidermal cell transplants performed using the RTU kit were well tolerated with mild procedural complications (e.g. pain) or graft-related skin disorders (e.g. wound, bleeding), which recovered quickly and were considered by doctors to be expected for such a procedure. The results of the current study demonstrate that cell grafting using the RTU kit is effective in the repigmentation of stable vitiligo and piebaldism lesion with rapid and persistent effects.
Such results are consistent with the data of van Geel et al., showing that a transplanted epidermal cell suspension induced repigmentation of at least 70% in 55% of patients at 6 months. A long-term study of 142 patients (11) showed that, after 6 years, 56% have excellent and 11% good results. In accordance with the current results, another study showed that lesions located on the hands, elbows and wrists are difficult to treat (12). The study by Mulekar et al. (12) suggests that repeated transplants of autologous epidermal cells may be beneficial for such lesions. A recent randomized controlled study showed that mixing equal amounts of follicular cell suspension with epidermal cell suspension enhanced the efficacy of the autologous cell grafting as a novel approach for difficult-to-treat vitiligo lesions (13). This new finding, combined with the RTU kit, could be used to treat these lesions more effectively.
This study has some limitations. First, it was impossible to ensure procedural standardization (e.g. trypsinization, exact time and temperature) and the choice of patient to be included varied according to centres (e.g. one site included only patients with lesions on the hands and wrists). Data concerning the skin biopsy collection site was not captured for each patient; however, investigators have performed biopsies on the scalp, pubis or buttock, depending on the vitiligo location. Another limitation is that, when investigating medical devices, heterogeneous results were observed between sites, which are well-described as cluster effects (14). This could affect the response to treatment and may increase the variability of the results. Effectively, professional skills and the extent of activity differ according to centre and according to doctors; for instance, 1 site, which performed a very high quantity of grafts before the study, achieved a 67% success rate during the study. The response rate is directly related to experience; we can distinguish technical performance, which is centre/doctor-dependent, and clinical performance. This strongly suggests a beneficial role of previous training in autograft of epidermal cell suspensions. In addition, the number of subjects required for completion was not reached (36 patients treated instead of 42) because recruitment took longer than expected. This lower than expected number of patients slightly decreased the validity of the study without impacting the results, since the differences remained statistically significant. A large number of patients with lesions located on the hands, elbows and wrists were included and treated; these lesions are known to be difficult to treat and, as expected, no repigmentation was observed for all these lesions.
First-line treatment with topical immunosuppressors (15) combined or not with phototherapy (16, 17) are partially effective (6), but some patients are non-responders and for responder patients, results are not always persistent (18) and can be associated with adverse events especially when used in combination (19). Grafting using RTU kit can be considered as a second line of treatment of refractory small-medium-size stabilized vitiligo lesions and as a first line in the case of piebaldism (20). It should be noted that this device does not require specialized facilities (cell culture) or hospitalization (the procedure can be performed in an outpatient setting). The kit is complete and ready to use, and a further benefit is that it allows grafting on a medium-sized depigmented lesion area from a small skin biopsy.
The authors thank all the patients and centres that participated in this study and everyone who contributed to the development of the project. The patients in this study provided written informed consent to publication of their case details. All authors gave their final approval of the version to be published.
This study was sponsored by Laboratoires Genevrier. Data acquisition, data management, statistical analysis was supported by Novasco.
Conflicts of interest: N. van Geel, G. Leone and A. Taïeb have served on the scientific advisory board for Laboratoires Genevrier. E. Soriano is an employee of Laboratoires Genevrier.


 Click to show fullsize
Click to show fullsize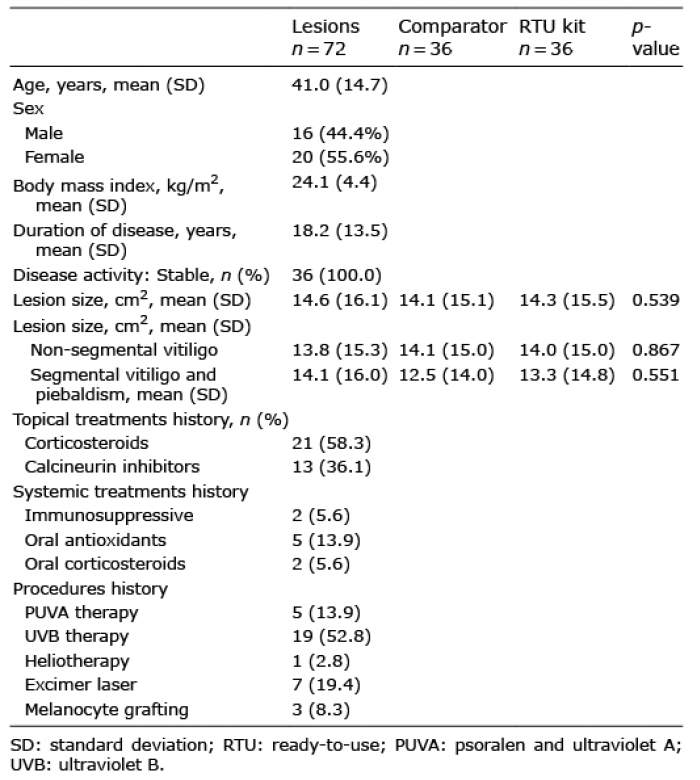 Click to show fullsize
Click to show fullsize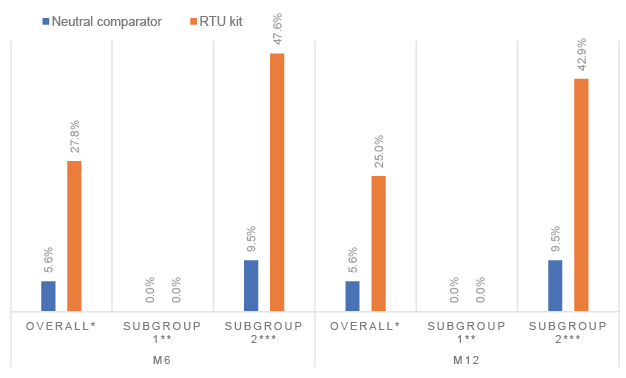 Click to show fullsize
Click to show fullsize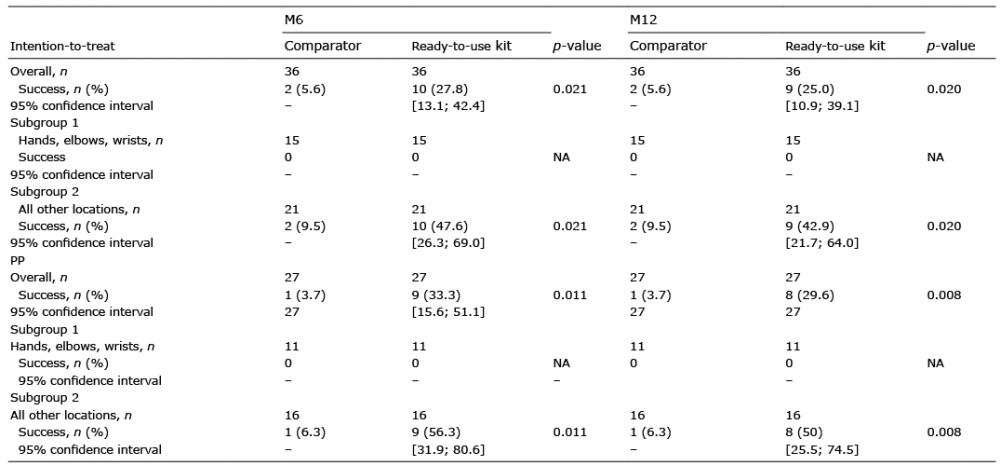 Click to show fullsize
Click to show fullsize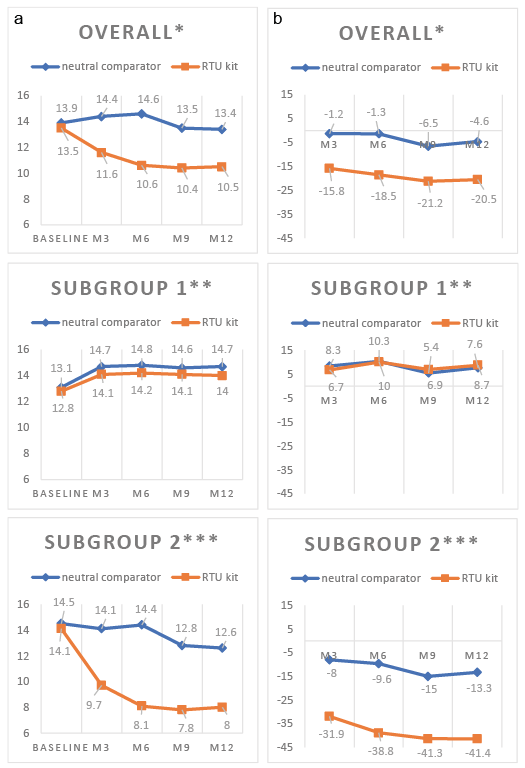 Click to show fullsize
Click to show fullsize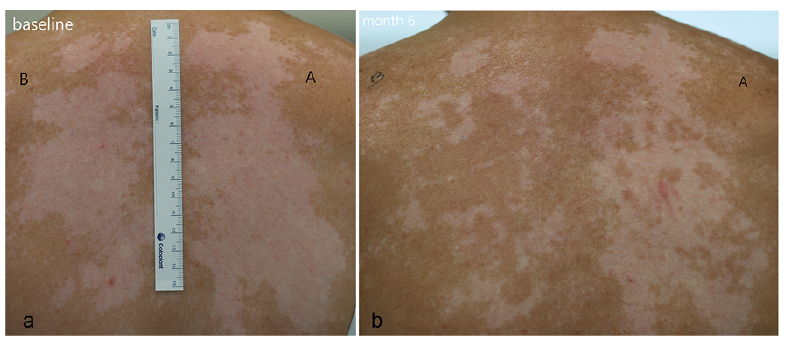 Click to show fullsize
Click to show fullsize