


1Department of Dermatology and Allergy, Herlev and Gentofte Hospital, University of Copenhagen and 2Copenhagen Research Group for Inflammatory Skin (CORGIS), Hellerup, Denmark
Advances in technology have led to an increased number of studies investigating the microbiome in patients with psoriasis. This systematic review examined data regarding the oral and gut microbiota in patients with psoriasis and/or psoriatic arthritis and the effect of probiotics on the microbiota and severity of psoriasis. Of 1,643 studies, 23 were included (22 observational, 1 interventional). Studies examined the microbiota using culture or 16S rRNA gene sequencing analysis. All culture-based studies identified an increased presence of oral Candida in patients with psoriasis, whereas small variations in the oral microbiota were found in a 16S rRNA gene-based study. All 16S rRNA gene sequencing based studies agreed that the gut microbiota of patients with psoriatic disease differed from that of healthy controls, but the results were heterogeneous. Probiotics were associated with a significant improvement in the severity of psoriasis, but did not change microbiota. Overall, studies lacked relevant inclusion criteria and baseline information. In conclusion, the role of the microbiota in patients with psoriasis requires further investigation using more robust methods.
Key words: psoriasis; psoriatic arthritis; microbiota; immune system; probiotics.
Accepted Jul 14, 2021; Epub ahead of print Jul 15, 2021
Acta Derm Venereol 2021; 101: adv00512.
doi: 10.2340/00015555-3882
Corr: Tanja Todberg, Department of Dermatology and Allergy, Herlev and Gentofte Hospital, University of Copenhagen, Gentofte Hospitalsvej 15, DK-2900, Denmark. E-mail: tanja.todberg@regionh.dk
Studies investigating the association between psoriasis and the microbiome have increased rapidly. This systematic review examined the role of the oral and gut microbiota and the effect of probiotics in patients with psoriasis and/or psoriatic arthritis. Twenty-three out of an initial total of 1,643 studies were included in the analysis. Of these, 22 studies were observational and 1 was interventional. The results showed increased presence of Candida in the oral cavity, and all studies examining the gut microbiota identified an altered microbiota in patients with psoriatic disease, but, overall, the results were heterogeneous. Probiotics were associated with a significant decrease in psoriasis severity, but the microbiota was unchanged. Further research is required into the role of the microbiome in patients with psoriasis.
Psoriasis is a chronic inflammatory skin disease affecting 2–4% of the population (1). It is associated with several comorbidities, including psoriatic arthritis (PsA) and inflammatory bowel disease (IBD) (2). The pathogenesis of psoriasis is believed to involve an interplay between genetics, environmental markers, and the immune system, in which interleukin (IL)-23 and the Th17-derived cytokines IL-17 and IL-22 are considered to be the main drivers of inflammation (3).
The gastrointestinal system harbours trillions of microbial cells, with more than 9.9 million genes identified and, currently, the potential role of aberrant gut microbiota in inflammatory diseases is the focus of intense research, as the intestinal microbiota is known to have a critical function in the maturation and homeostasis of the immune system (4).
Studies, including murine models of imiquimod induced-psoriasis, have shown that changes in gut bacteria are associated with increased severity of skin inflammation, supporting the linkage between a gut–skin axis (5). Likewise, in adult mice, dysbiosis caused by administration of antibiotics has been associated with a reduced Th17 response and decreased psoriasiform inflammation (6). This potential modulation of the gut microbiome may represent a new target for the treatment of psoriasis; however, a greater understanding of the functional potential of the gut microbiome is needed.
In recent years there has been increased focus on inflammation and psoriasis, leading to an emerging number of studies investigating the microbiome in patients with psoriasis. Methodological characterization of the microbiome has evolved rapidly; thus, culture-dependent methods are being replaced by sequencing analyses, such as 16S rRNA gene amplicon technique and shotgun metagenomic sequencing (7). Consequently, differences in study designs and methods make it difficult to interpret the results.
The focus of this systematic review was to summarize results, taking into account methodological variations in studies, regarding the gut microbiota in patients with psoriatic diseases (i.e. psoriasis or PsA) compared with healthy controls. Since the oral cavity is part of the gastrointestinal tract and, due to the association between psoriasis and periodontal diseases, oral microbiota studies were also included (8).
This systematic review was established and performed in accordance with the Preferred Reporting Items for Systematic Review and Meta- Analyses (PRISMA) guidelines (9). A priori, a protocol was registered at PROSPERO (CRD42020168641).
Literature search
The databases PubMed, Embase, Cochrane Library and clinicaltrials.gov were searched for articles and trials until 11 March 2021, using the search term: “((psoriasis OR psoriatic OR psoriatic arthritis) AND ((microbiome OR microbiota OR microbial OR microflora OR prebiotics OR probiotics OR synbiotics) OR ((gut OR gastrointestinal OR gastro OR intestinal OR oral OR saliva OR dental) AND (diversity OR abundance OR composition OR balance)))”.
Study selection, outcome and quality assessment
Two authors (TT, HK) screened the titles and abstracts for eligible full-text studies. Eligibility criteria were observational studies that examined the association between patients with psoriasis and/or PsA and the oral and/or gut microbiome compared with healthy controls. Further interventional studies examining the effect of probiotics on the oral/and or gut microbiome in patients with psoriasis and/or PsA, were included. Animal studies and non-English studies, conference abstracts, case reports, and studies with no healthy control group or microbiome data were excluded. Newcastle Ottawa Scale (NOS) (score ≥ 7 indicated high-quality study) and Cochrane Collaboration’s tool were used for quality assessment (10).
Study characteristics
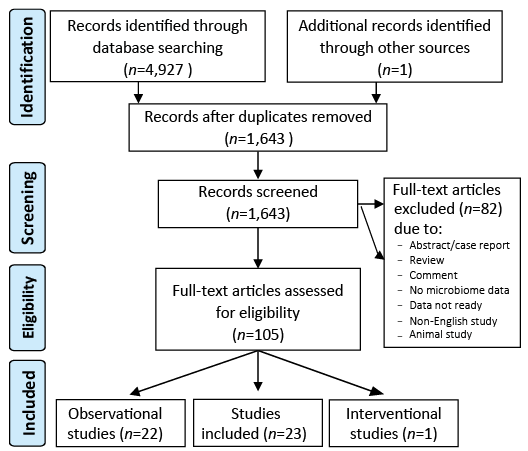
A total of 1,643 studies were identified in the screening process. Of these, 105 full-texts were eligible for further review and 23 full-text articles were included in the analysis (Fig. 1).
Fig. 1. Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow chart.
The studies included 4,379 participants, of whom 1,388 had psoriasis and 36 had PsA. All studies examined adults, except one study examining both children and adults (age range 10–82 years) (11) and, in most studies, the psoriatic population was age- and sex-matched with the control population (12–23). Nine studies included patients with plaque psoriasis only (11–13, 18, 20, 23–26), 6 studies included patients with mixed psoriasis types (15, 17, 21, 22, 27, 28) and 7 studies did not specify the type of psoriasis (14, 16, 19, 29–32). Fifteen studies examined patients with mild, moderate or severe psoriasis (11–13, 15–22, 24, 25, 27, 29), 2 studies examined patients with mild psoriasis (14, 32) and 4 studies reported no information on psoriasis severity (23, 28, 30, 31).
Quality assessment
Due to lack of information or unmatched controls, 16 studies were rated with a NOS score < 7 (11–13, 15, 17, 18, 22, 23, 25, 27–33), and 6 studies rated ≥ 7 (14, 16, 19–21, 24). The interventional study was rated with a low risk of bias (34).
Observational studies
Oral microbiota and psoriasis. Five studies investigated the oral microbiota in patients with psoriasis (n = 347) compared with healthy controls (n = 669) (11, 13, 24, 29, 30). Of these, 4 used culture-dependent methods and 1 used 16S rRNA gene sequencing analysis. Studies included both untreated patients and patients who used anti-psoriatic treatment, in 4 studies antibiotics were prohibited from 0–3 months before inclusion (11, 24, 29, 30), 2 studies had excluded patients with diabetes (11, 24), and in one study it was clinically verified that neither patients with psoriasis nor controls had periodontitis (30) Different methods were used for collection of oral material (Tables I and SI).
Table I. Overview of observational studies characterizing the oral microbiota in patients with psoriasis and in healthy controls
Gut microbiota and psoriasis. Sixteen studies investigated the gut microbiota in patients with psoriasis (n = 812) compared with healthy controls (n = 242). Various criteria for use of concomitant treatment were allowed; in the majority of studies, antibiotics were prohibited from 2 weeks to 3 months before inclusion, but 4 studies gave no information on the use of antibiotics (13, 28, 32, 33). In most studies patients used various treatments for psoriasis, including topical corticosteroids, phototherapy and systemic anti-inflammatory treatment. However, in 4 studies, patients were systemic-naïve for 3 months prior to inclusion (12, 14, 16, 20). Regarding comorbidities, 4 studies included patients with diabetes (18–20, 31). Heterogeneous methods were used for collection of stool samples (Tables II and SI).
Table II. Overview of observational and interventional studies characterizing the gut microbiota in patients with psoriasis and/or psoriatic arthritis and in healthy controls
Various methods were used to assess α-diversity, and comparison between studies showed large variability (12, 14, 16, 1 7, 19–23, 25, 31). For patients with psoriasis; 2 studies reported a decreased diversity (16, 25), one found an increased diversity (12) and 6 studies found no significant differences between patients with psoriasis and healthy controls (17, 18, 21–23, 31). In addition, one of these studies, including 32 patients with psoriasis and 64 healthy controls, reported that sex, phototherapy, diet, alcohol, smoking, physical activity or the severity of psoriasis did not significantly affect the microbial profile (18). Notably, another study found no difference in α-diversity when investigating 55 patients with psoriasis compared with 27 healthy controls, but a lower richness in patients with more severe psoriasis was shown (20).
β-diversity
In all 10 studies that assessed β-diversity, a difference was observed between patients with psoriasis and healthy controls (12, 14, 16–20, 22, 23, 25, 31). Interestingly, one study (18) found that the difference was present only when comparing patients with psoriasis (n = 19) and healthy controls (n = 36) with body mass index (BMI) <25 kg/m2, but not among subjects with BMI ≥25 kg/m2.
Differences in relative abundance
Studies showed large variability when evaluating relative abundance and focused on various taxonomy levels. At phyla level, 5 studies described Bacteroidetes, Firmicutes, Proteobacteriae and Actinobacteriae as the most dominating bacteria in both patients with psoriasis and in healthy controls, with Bacteroidetes and Firmicutes as the most abundant (16–18, 20, 31).
In patients with psoriasis, 6 studies found Bacteroidetes to be decreased, and Firmicutes and Actinobacteriae to be increased (12, 14, 16, 18, 20, 31); however, one study found the opposite, with an increased level of Bacteroidetes and decreased levels of Firmicutes and Actinobacteriae in patients with psoriasis (n = 35) compared with healthy controls (n = 27) (17). At the family level, 2 studies described that patients with psoriasis had less Prevotellaceae than healthy controls (16, 18). At the genus level, Akkermansia was increased in patients with psoriasis in one study, whereas a low abundance of Akkermansia in patients with psoriasis was found in 2 studies (12, 14, 25).
Gut microbiota and psoriatic arthritis. Three studies examined the gut microbiota in patients with PsA (n = 36) compared with healthy controls (n = 68) (14, 32, 33). In 2 studies, all patients also had psoriasis (14, 32). A culture-based study found E. coli isolated as the only species in a small group of patients with PsA (n = 5), compared with the control group (n = 36) where E. coli, Enterococcus, Klebsielle oxytoca and Klebsiella pneumonia were present (33). Two studies were based on 16s rRNA gene analysis (14, 32), with one study presenting a lower abundance of Akkermansia in patients with PsA (n = 16) compared with healthy controls (n = 17) (14).
Interventional studies
Only one study examined the effect of probiotics on the gut microbiome and the severity of psoriasis. In this 12-week randomized controlled trial, 90 patients with psoriasis were randomized to daily doses of either probiotic capsules or placebo (34). Topical treatment was allowed during the study. At the end of the trial the authors found no significant difference in the microbiota between the probiotic and the placebo groups, but the results showed a significantly clinical effect on severity of psoriasis; 66.7% of subjects in the probiotic group achieved at least PASI75 compared with 41.9% of subjects in the placebo group (p = 0.03) (Tables III and SII).
Table III. Overview of interventional study characterizing the gut microbiome in patients with psoriasis after treatment with probiotics vs placebo
Main findings
Overall, this review demonstrates that patients with psoriasis seem to have some variations in their microbiota compared with healthy controls, but, in general, the results were based on small sample sizes and, across studies, there were wide variations in inclusion criteria and methods used.
Across studies using the culture-based method the prevalence of Candida in the oral cavity and gut was found to be higher in patients with psoriatic diseases, whereas the single study examining the oral microbiota using 16S rRNA gene sequencing analysis found no difference in α- or β-diversity, although some taxa differed between groups.
Across studies that examined the gut microbiota using 16S rRNA gene sequencing analysis, no core microbiota of patients with psoriatic disease was identified, although all the studies agreed that patients with psoriatic disease had a distinct microbiota compared with healthy controls. Except for β-diversity, where clustering was identified between patients with psoriatic disease and healthy controls, no consensus was found for α-diversity and lower taxonomic profiles varied between studies.
Interestingly, the interventional study found no significant change in microbial composition after administration of probiotics, but a considerable clinical improvement in psoriasis was seen.
Interpretation
Several factors might contribute to the increased presence of Candida in the oral microbiota in patients with psoriasis. Patients with psoriasis use various immunosuppressive drugs, are more often smokers, and diabetes is more common among this patient group (35). In fact, in former studies, smoking and obesity have been associated with periodontitis (36, 37), which is characterized by an altered oral microbiota (38); hence conditions other than psoriasis may impact the oral microbiology. Of note, only one study verified that patients with psoriasis did not have periodontitis prior to inclusion (30).
In addition, food substances, such as simple carbohydrates, are known to affect the microbial environment, and may increase the risk of Candida colonization; however, studies gave no information about variations in diet between patients with psoriasis and healthy controls (39). Notably, 1 included study observed a distinct oral bacterial environment in patients with psoriasis compared with healthy controls and, as it is well known that approximately 1,500 bacterial species inhabit the oral cavity, with each person harbouring approximately 200 species, it cannot be excluded that patients with psoriasis have a distinct bacterial environment that is more susceptible to Candida species (30), although the results may be confounded by various factors.
All sequencing-based studies assessing the gut microbiota found heterogeneous results, although, at phyla level, 5 studies agreed that Bacteroidetes, Firmicutes, Proteobacteriae and Actinobacteriae were the most abundant, both in patients with psoriasis and in healthy controls (16–18, 20, 31). In support of this, previous studies have detected these phyla as the most dominating independent of health status (40, 41). It is widely discussed whether the dominance of bacterial groups may impact on health, with some reporting wide variation in dominance of, for example, the genus Bacteroides, in a large study of healthy individuals (42), indicating that a low or high ratio of specific families, genera or species may not indicate that a person is unhealthy or “dysbiotic”. In contrast, others have suggested that the dominance of specific phyla may be important, as previous studies have linked a high Firmicutes/Bacteroidetes ratio with obesity, while a decrease in the Firmicutes/Bacteroidetes ratio has been observed in patients undergoing weight loss (43). Notably, 6 studies agreed that Firmicutes were more abundant compared with Bacteroidetes in patients with psoriasis, one study found a lower Firmicutes/Bacteroidetes ratio, and one study found no significant difference in Firmicutes/Bacteroidetes ratio between patients with psoriasis and healthy controls (21).
It is well described that obesity is associated with an aberrant microbial profile; therefore BMI is an important factor to consider in the analyses of microbiota data (44). In support of this, one study identified a difference between normal-weight patients with psoriasis and normal-weight healthy controls, but not between overweight groups; thus data from normal-weight subjects may represent a more “true” microbiota profile, when not confounded by obesity (18). Overall, patients in the studies had a mean BMI ≥25 kg/m2 (15, 18, 20, 27, 31, 32). This is in line with the literature, as it is well known that patients with psoriasis are more often obese compared with the background population (45).
In one study the genus Akkermansia was found to be increased in patient with psoriasis (12), whereas 2 studies found that Akkermansia was decreased in patients with psoriasis, and decreased even more in patients with both psoriasis and PsA (14, 25). Akkermansia is a commensal in the large intestines, representing 1–4% of the microbiota in healthy adults, and has been associated with dual functions. In murine studies Akkermansia has been linked with mucus degradation (46, 47), which may, in turn, facilitate increased permeability of the intestinal wall. In theory, this could potentially contribute to the systemic inflammation of psoriasis, as bacterial DNA with origin from the intestines has been observed in peripheral blood in patients with moderate-to-severe plaque psoriasis, but not in healthy controls (48). In contrast, adequate levels of Akkermansia species have been associated with beneficial regulation of mucus thickness, interaction with the immune system via Toll-like receptors and with the production of short-chained-fatty-acids (SCFA), which are produced by gut microbiota as metabolites of a fibre-rich diet (49–51). SFCA acetate, propionate and butyrate are known to have immune regulatory effect on regulatory T-cells (Treg) in immune-mediated diseases (52). Of note, most of the main producers of butyrate belong the families of Ruminococcaceae Lachnospiraceae (53). A recent study has shown that, in murine models of imiquimod-induced psoriasis and in isolated peripheral human blood from patients with psoriasis, butyrate stimulated the activity of Treg, leading to reduced expression of IL-17 and IL-6 and increased IL-10 expression (54). Thus, a fibre-rich diet is likely to decrease proinflammatory metabolites in the gut, leading to reduced IL-17 expression, and thereby decreased severity of psoriasis. Only one study assessed diet, and found that this did not affect the microbial profile (18). However, diet has been shown to affect the microbiota in several studies (4, 49, 55). Indeed, the genus Prevotella has been linked to a diet rich in plant-fibre and is more common in non-Westernized populations and, in 4 studies, the abundance of Prevotella was decreased in patients with psoriasis compared with the control populations (16, 18, 20, 31).
The role of probiotics in psoriasis
In the interventional study, no significant change in the microbiota was observed in the probiotic-treated group compared with the placebo group, but when evaluating the clinical effect, a substantial reduction in the severity of psoriasis was seen in the treated group, with 66.7% of patients achieving PASI75 compared with 41.9% of patients in the placebo group.
The gut microbiota comprises approximately 1012 microbial cells, compared with probiotics comprising 109 colony-forming units; thus the microbiota outnumbers the probiotics extensively (56). Probiotic capsules are often consumed orally, and therefore need to survive the low pH in the stomach and to be established in a very diverse ecosystem with competition from the commensal microbiota. Although authors found a significant difference in the clinical presentation of psoriasis, a limitation was that topical corticosteroid use was not prohibited. Notably, numerous studies in patients with other indications have shown that there is little evidence to show that probiotics can change the gut microbiota (57, 58).
Heterogeneity of study design
The overall results were heterogeneous, although in most studies patients were age- and sex-matched. In general, studies lacked description of possible factors that may interfere with the results. Antibiotics that are known to affect the microbiota were prohibited for at least 3 months in only 5 studies (14, 16, 20, 30, 31). A recent paper has shown the microbiome to be affected by antibiotics for up to 6 months (59).
In addition, possible confounders that may affect the results include; non-BMI-matched populations, inclusion of participants with other immune-mediated disease and concomitant treatments, such as metformin and proton pump inhibitors, which are well-known modulators of the microbiota (60, 61). When including patients with psoriasis in systemic treatment for psoriasis, authors should be aware that it may not be the association between the gut microbiota and psoriasis that is investigated, but rather the effect of a drug on the microbiota and psoriasis (60). Likewise, the collection of samples, season, ethnicity and matching groups from the same district can play a role (59).
Heterogeneity of methodology
In addition, the heterogeneity of the results may be explained by the type of analyses carried out. Culturing-based analysis is able to identify both bacteria and fungi, depending on the choice of media; however, as anaerobic bacteria comprise a large proportion of the commensals in the distal colon, this type of analysis is associated with several limitations, with only 0.1–10% of gut commensals being able to be grown in culture (62), thus a large discrepancy between culture- and sequenced-based studies exists, making them difficult to compare.
The 16s rRNA gene analysis targets both aerobic and anaerobic bacteria; however, the analysis is limited by typically not being able to sequence deeper than genus level, and by fungi not being identified. In addition, it is often based on operational taxonomic units (OTUs), in which a 97% similarity profile of base pairs is grouping OTUs together, which may be associated with errors (59).
In the 16S rRNA gene sequencing-based studies, choice of primers varied. Choosing the right primers is crucial when conducting a microbiome study, i.e. a study showed that the V1–V2 primer was unable to identify the most abundant bacteria in the vaginal tract (63). To study the microbiota V4–V5 is recommended prior to V3–V4, as, in most cases, it produces the most comparable results (64, 65).
None of the studies used shotgun metagenomic sequencing, which may be because this is a relatively new method and the expensive price. Shotgun metagenomic sequencing detects bacteria at the species level and, sometimes, even at strain level, depending on the sequencing depth, and information is given about the functional potential of the microbiota (59). The key to improving understanding of the microbiome may not be to identify which bacteria are present, which, to some extent, is provided by the 16S rRNA gene sequencing analysis, but rather to recognize the function of the bacteria.
Studies investigating other inflammatory diseases, such as atopic dermatitis, found that, although the same species are identified in both patients and in healthy controls, at strain level the bacteria can be different, highlighting the limitations of using 16S rRNA gene sequencing analysis (66). Another strength of using shotgun metagenomic sequencing is that fungi, virus and phages can sometimes be detected, which are all commensals with affinity to interfere with bacteria (67).
Study limitations
This systematic review has several limitations, including risk of publication bias, and the identified differences between patients with psoriasis and healthy controls may be explained by various confounders. The studies are based on culture or 16S rRNA gene sequencing analysis, and therefore the function of the microbiota is not described. The gut microbiota was assessed using stool samples; however, this analysis is limited as it represents only the end-products of the microbial composition. Furthermore, the data are based on observational single-point time profiles, and how to utilize these findings in development of treatment strategies and clinical practice remains unclear.
Conclusion
This review found a difference in the oral and gut microbiota between patients with psoriatic diseases and healthy controls. However, overall, studies lacked important information, as restrictions due to treatments and included patients with comorbidities known to affect the microbiota. Methodological heterogeneity was found between studies, including variations in sampling and processing of the identification of microbiota profiles; thus, any conclusions must be considered with caution. To date, there is no consensus for conducting a microbiome study; however, some guidelines have been published (59). In general, a challenge in microbiome studies is that it is a new research field. To improve insights of the microbiota in patients with psoriatic diseases, the design of future studies would benefit from strict matching, more restrictions, and assessment of the microbial profile with combined data and more advanced methods.
ACKNOWLEDGEMENTS
This study was supported by Aage Bangs Foundation.
Disclosures and conflicts of interests: TT has been an investigator for Novartis, Abbvie, Dr Wolff and Almirall. AE has received research funding from Pfizer, Eli Lilly, Novartis, Bristol-Myers Squibb, AbbVie, Janssen Pharmaceuticals, the Danish National Psoriasis Foundation, the Simon Spies Foundation, and the Kgl Hofbundtmager Aage Bang Foundation, and honoraria as consultant and/or speaker from AbbVie, Almirall, Leo Pharma, Galápagos NV, Sun Pharmaceuticals, Samsung Bioepis Co., Ltd., Pfizer, Eli Lilly and Co., Novartis, Galderma, Dermavant, UCB, Mylan, Bristol-Myers Squibb, and Janssen Pharmaceuticals. CZ has been an advisor, investigator and speaker for Abbvie, Eli Lilly, Novartis, Sanofi, Leo Pharma, UCB, CSL and Almirall. ASHO has received honoraria as speaker for Leo Pharma and consultant for Coloplast A/S. LS has been an advisor, investigator and speaker for Abbvie, Eli Lilly, Novartis, Sanofi, Celegene, Leo Pharma, BMS, UCB and Almirall, outside the submitted work. LS reports non-financial support from Abbvie, Sanofi, Janssen and grants from Novartis, Janssen, BMS and Sanofi.


 Click to show fullsize
Click to show fullsize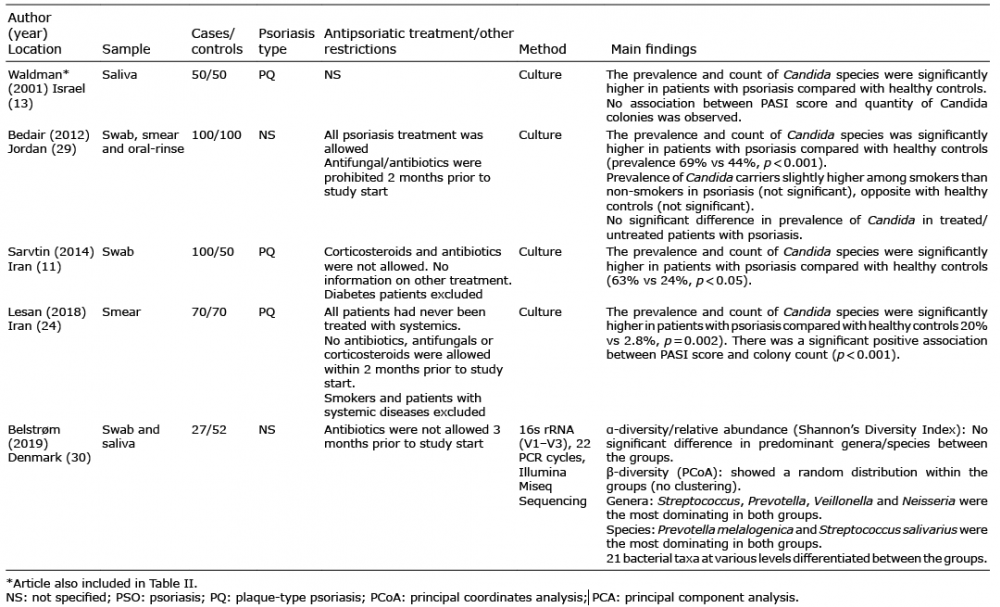 Click to show fullsize
Click to show fullsize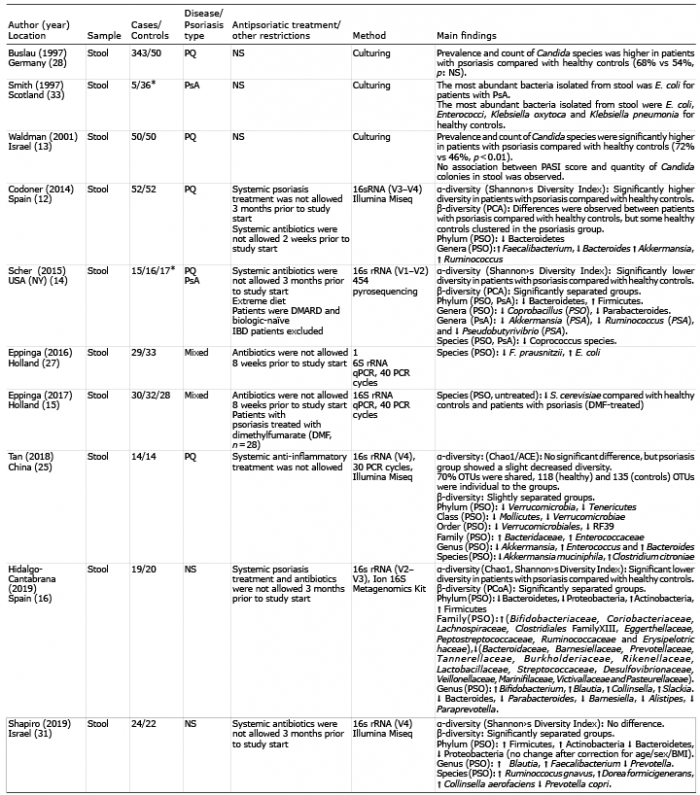 Click to show fullsize
Click to show fullsize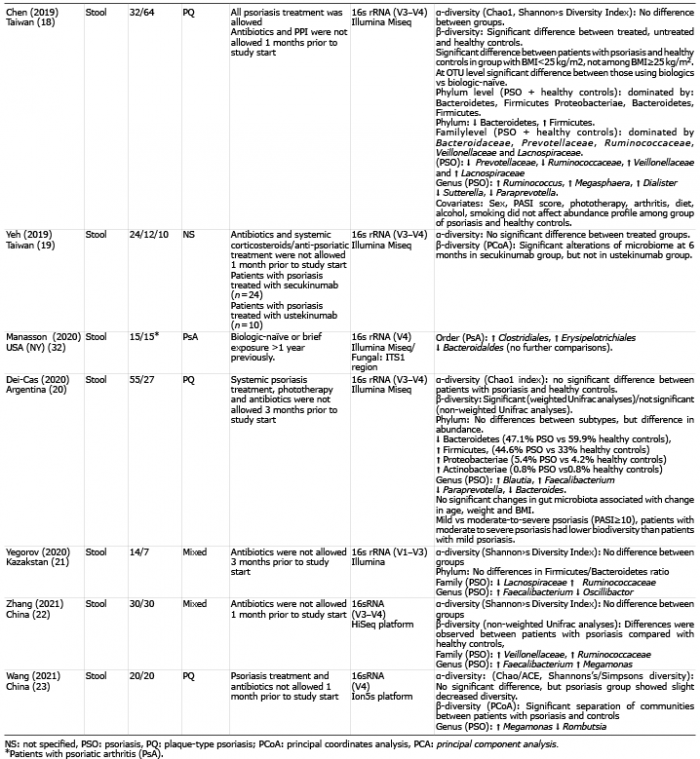 Click to show fullsize
Click to show fullsize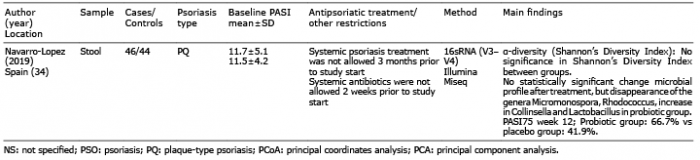 Click to show fullsize
Click to show fullsize