


1Department of Dermatology and Allergy, Technical University of Munich, School of Medicine, Munich, 2Department of Dermatology and Allergy, Hannover Medical School, and 3Immunodermatology and Allergy Research Hannover, Hannover, Germany
#Contributed equally as shared first authors; *contributed equally as shared last authors.
The globally increasing prevalence of chronic inflammatory skin diseases has substantial costs. Biologicals have become available as therapeutic options, but are encumbered with barriers to prescription. The aim of this study was to evaluate the barriers to prescription of biologicals in the treatment of chronic dermatological diseases. Dermatologists working in private practices in the German federal states of Bavaria and Lower Saxony participated in a cross-sectional study. Economic and legal aspects, including “high therapy costs”, “low reimbursements”, and “fear of regress claims”, were identified as the most prevalent barriers. Significant differences between dermatologists from Bavaria and Lower Saxony were found only regarding the treatment of atopic dermatitis. This study demonstrates the prevalence of barriers to the prescription of biologicals in the treatment of chronic dermatological diseases. Overcoming these barriers could improve the usage of modern therapies and thereby expand patient-centred care for chronic skin diseases.
Key words: biological therapy; dermatology; healthcare costs; prescriptions; patient-centred care; skin diseases.
Accepted Aug 18, 2021; Epub ahead of print Aug 24, 2021
Acta Derm Venereol 2021; 101: adv00560.
doi: 10.2340/00015555-3901
Corr: Maximilan C. Schielein, Technical University of Munich, School of Medicine, Department for Dermatology and Allergy, Biedersteiner Straße 29, DE-80802 Munich. E-mail: maximilian.schielein@tum.de
Biologicals are highly effective medicaments in the treatment of chronic skin diseases. Nevertheless, their prescription is encumbered by barriers. This study addresses the prevalence of barriers to the prescription of biologicals in the treatment of atopic dermatitis, chronic spontaneous urticaria and psoriasis by dermatologists working in private practice in 2 German federal states. “High therapy costs”, “low reimbursements”, and “fear of regress claims” were identified as the strongest barriers. Overcoming these barriers, by improving the education of dermatologists in legal, economic, and medical matters associated with the the prescription of biologicals, may contribute to improved patient-centred care.
Psoriasis, atopic dermatitis (AD), and chronic spontaneous urticaria (CSU) are chronic skin diseases with increasing global prevalence in recent years (1–3). They are associated with various symptoms, comorbidities, and impairment in quality of life (3–10), and their socio-economic impact has led to substantial costs, not only for individual patients as out-of-pocket costs, but also for health systems in general and for society as a whole (11–15).
Recently, new options for treating these diseases have evolved, to include the administration of biologicals that specifically block the activity of pro-inflammatory physiological components (16–19). The usage of biologicals is recommended by current guidelines for the treatment of moderate to severe psoriasis, AD and CSU (17, 20, 21). It is assumed that 25.0% of all patients with psoriasis have moderate to severe psoriasis (22) and that approximately 74.5% of patients with AD have a moderate to severe form of AD (23). Despite the high cost of this medication, a cost-effectiveness advantage of treatment with biologicals has been shown in several studies (24, 25). Nevertheless, prescription rates of biologicals were found to be low compared with the number of eligible patients in several European countries (26, 27). In a study from 2017, barriers to the prescription of biologicals included regulatory issues, high therapy costs, and low reimbursement for patient care for office-based dermatologists in Bavaria (28).
The aim of this study was to evaluate current barriers to the prescription of biologicals for dermatological practices, while considering the aforementioned barriers from 2017 to examine possible changes. The study was conducted for 3 different chronic dermatological diseases (moderate to severe psoriasis, atopic dermatitis, and chronic spontaneous urticaria) in the German federal states of Bavaria and Lower Saxony.
Study design
This cross-sectional, non-interventional, questionnaire-based study was conducted with dermatologists working in private practice in the German federal states of Bavaria and Lower Saxony from July to August 2020. Dermatologists registered on the official webpages (accessed 1 July 2020) of the databases of the Bavarian Association of Panel Doctors (Kassenärztliche Vereinigung Bayerns; KVB) (n = 608) and of the Lower Saxonian Association of Panel Doctors (Kassenärztliche Vereinigung Niedersachsen; KVN) (n = 350) were contacted individually. They were invited by post to participate in the study by completing an anonymized paper-based questionnaire after giving written consent for their participation. The dermatologists were also provided with the study information and a prepaid return envelope. All dermatologists received a reminder letter after one week.
The study was conducted in accordance with the principles of the Declaration of Helsinki and Good Clinical Practice guidelines and was approved by the ethics committees of Hannover Medical School (number 9123_BO_K2020) and the School of Medicine at the Technical University of Munich (number 361/20 S).
Questionnaire
A questionnaire for evaluating barriers to the prescription of biologicals for the treatment of moderate to severe psoriasis, CSU, and moderate to severe AD was developed based on pre-existing literature (28, 29). After feedback from 10 dermatologists from the departments of dermatology and allergy of the Technical University of Munich and the Hannover Medical School, questions were added and modified if consensus was reached in a study group that included 2 senior physicians, 1 assistant physician, 1 epidemiologist, and 2 medical students.
The questionnaire was divided into 3 sections. The first section included general questions on the personal and professional status of the participants (sex, age, workplace, and professional experience). In the second section, the participants were asked whether they co-operate with hospitals in the treatment of patients with biologicals, how many patients they treat per year, and how many patients are treated with biologicals. In the third section, participants were asked for an individual assessment of 18 barriers to the prescription of biologicals that were subdivided into 4 categories (28, 29): “physicians’ concerns”, “patients’ concerns”, “concerns regarding biologicals themselves”, and “external factors”. Possible answers were “not applicable”, “no barrier”, “moderate barrier”, and “strong barrier”. The questions were directed specifically to the situation prior to the COVID-19 coronavirus pandemic.
Statistical analysis
General characteristics were analysed using descriptive statistics and compared using unpaired t-tests and χ2 tests, where applicable.
Dermatologists were categorized into 2 categories: “low prescription” and “high prescription”, based on median splits for the parameter “proportion of patients treated with biologicals” for the respective diseases. For moderate to severe psoriasis, the median split was 20.0%, for CSU 8.0%, and for moderate to severe AD 4.0%. Univariate regression analysis was performed for the identification of associated variables. Thereby, “sex”, “work experience”, “state”, “number of patients treated for the respective disease”, and all 18 barriers were considered as independent variables. Multivariate analyses, including backward selections, were conducted. The parameters “sex”, “state,” and “work experience” were kept as fixed variables. The barriers were all entered and then removed stepwise.
Answers from the returned questionnaires were digitized using REDcap (Research Electronic Data Capture, Vanderbilt University, Nashville, TN, USA). Each answer was entered twice, and subsequent discrepancies in entries were identified and corrected. IBM SPSS Statistics (Version 26, IBM Corporation, Armonk, NY, USA) was used for all analyses and alpha error was set at 0.05.
Participating physicians
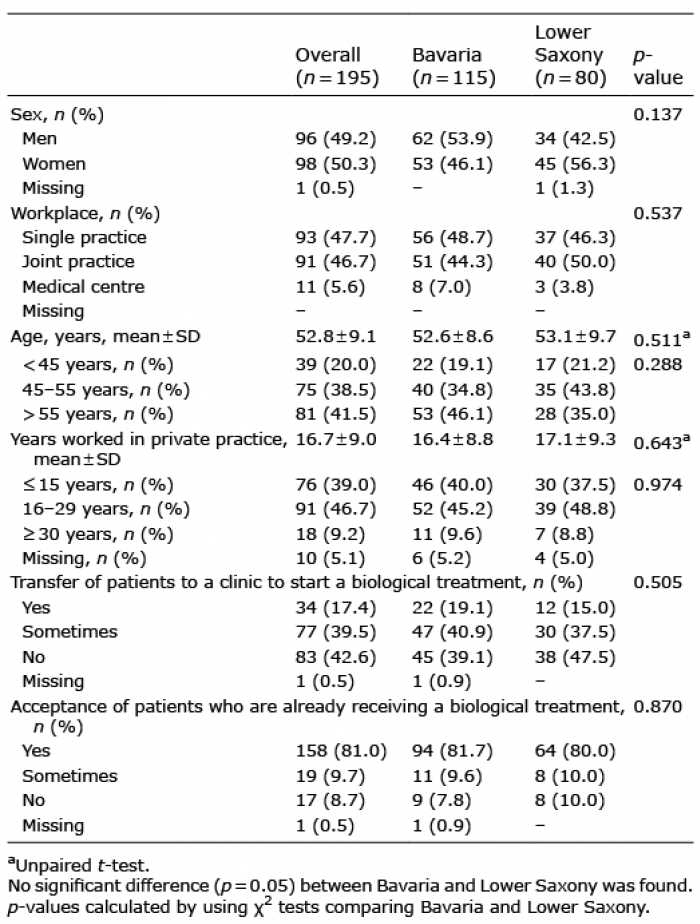
Overall, 195 dermatologists (49.2% male and 50.3% female; mean age: 52.8 ± 9.1 years) participated in the study, yielding an overall response rate of 20.6% (195/958). Furthermore, 115 participants (53.9% male and 46.1% female) were from Bavaria and 80 (42.5% male and 56.3% female) were from Lower Saxony. The majority of the participants were 55 years old or younger (n = 114; 58.5%). The proportion of male participants in Bavaria (n = 62; 53.9%) was higher than in Lower Saxony (n = 34; 42.5%), although the difference was not significant (p = 0.137) (Table I).
Table I. General population characteristics and descriptive analysis
Work experience
Overall, the participating dermatologists had a mean work experience of 16.7 ± 9.0 years in private practice, with 39.0% (n = 76) having a work experience of 15 years or less, 46.7% (n = 91) between 16 and 29 years, and 9.2% (n = 18) 30 years or more (Table I). The number of dermatologists working in a single practice (n = 93; 47.7%) and in a joint practice (n = 91; 46.7%) were similar, whereas only a few participants (n = 11; 5.6%) stated that they work in a medical care centre (Table I). The work experience of participants from Bavaria was comparable to that of participants from Lower Saxony (p = 0.974) (Table I).
Therapy with biologicals in general
More than half of all dermatologists at least sometimes transferred patients to a hospital to start treatment with biologicals (56.9%). In contrast, 8.7% stated that they did not accept new patients who started therapy with biologicals elsewhere (Table I).
The mean annual patient count for moderate to severe psoriasis was 104 ± 139 patients, with 29.4 ± 25.0% receiving biologicals (Table II). The mean annual patient count for CSU was 40 ± 53, with 15.0 ± 20.5% receiving biologicals (Table II). For AD, the mean annual patient count was 94 ± 141, with 11.1 ± 17.0% receiving biologicals (Table II).
Table II. Patient treatment characteristics and descriptive analysis
Barriers to the usage of biologicals
More than 10% of participants identified the barriers “external factors”, “insufficient reimbursement”, “fear of regress”, and “high costs” in the category “external factors” as strong (Table III). Similar percentages were observed for the barriers “lack of time for treatment adjustment” and “complexity of medical pre-examination” in the category “physicians’ concerns” and the barrier “sufficiency of conventional therapy” in the category “concerns regarding biologicals themselves” (Table III). In the group “patients’ concerns”, no barrier was considered strong by more than 10% of the participants. “Disapproval by supervisors” and “previous regress claims” were considered as “not applicable” by more than 80% of participants. This might be due to a low frequency of regress claims and the absence of a supervisor in a large majority of the participants, since many office-based physicians work in single-physician offices and have no supervisor. Combined with a logical ad hoc conclusion, these barriers were disregarded for the subsequent evaluation of means for each barrier category.
Table III. Strength of barriers to the prescription of biologicals divided into 4 barrier categories
The mean prevalence for each barrier category was calculated by adding percentages of individual answers for each barrier and dividing the result by the number of barriers within the respective group (Fig. 1). Strong barriers were identified by 25.2% of participants in the group “external factors”, which is approximately 4–6 times higher than the percentage in all other groups, where strong barriers were reported by less than 7% of participants. Moderate barriers were perceived particularly in the categories “patients’ concerns” and “external factors”, with 36.7% and 25.9% of the participants, respectively. The relative ratio of strong to moderate barriers was approximately 1:1 (25.2% vs 25.9%) in the group “external factors”. This was lower in the other groups with a relative ratio of 1:2 (6.6% vs 14.1%) in the category “physicians’ concerns”, 1:2.5 (4.1% vs 9.8%) in the category “concerns regarding biologicals themselves”, and 1:6 (5.9% vs 36.7%) in the category “patients’ concerns”. In the categories “concerns regarding biologicals themselves” and “physicians’ concerns”, the answers “not applicable” and “no barrier” were given by 86.1% and 79.5% of the participants (Fig. 1).
Fig. 1. Proportional perception of barriers by dermatologists divided into barrier categories. Values for the barriers “disapproval by supervisor” in the category “physicians´ concerns” and “previous regress claims” in the category “external factors” are excluded. Missing values are excluded. Strong barriers were highest in the group “external factors” compared with in the other groups.
Combined strong and moderate barriers were analysed both for individual barriers and barrier categories (Fig. 2). The highest prevalence of barriers was found in the categories “external factors” (mean 51.1%) and “patients’ concerns” (mean 42.5%). Particularly prominent barriers were “high costs” (54.6%), “fear of regress” (50.0%), and “insufficient reimbursement” (48.4%) in the category “external factors”. “Previous regress claims” in this category was mentioned by only a small number of participants (7.2%) and was excluded for the calculation of means (Fig. 2). In the category “concerns regarding biologicals themselves”, barriers related to the efficiency of biologicals were considered not particularly prevalent (less than 10%), whereas barriers related to “concerns with regard to safety” (21.6%) and “sufficiency of conventional therapy” (32.5%) had a substantially higher prevalence. No significant differences in the strengths of combined strong and moderate barriers were found between Bavaria and Lower Saxony (Table SI).
Fig. 2. Strong and moderate barriers divided up by categories. Colour schemes were categorized as follows: 0–9.9%: green; 10–29.9%: yellow; 30–49.9%: orange; ≥50%: red. Values for the barriers “Disapproval by supervisor” in the category “physicians’ concerns” and “previous regress claims” in the category “external factors” were not considered in the calculations of mean values. Most prominent barrier categories were “patients’ concerns” and “external factors” compared with “physicans’ concerns” and “concerns with regard to biologicals”.
Predictors for the prescription of biologicals
Univariate and multivariate logistic regressions were performed to identify barriers possibly associated with the prescription of biologicals for psoriasis, CSU, and AD (Table SII). In univariate regressions, 11 out of 18 barriers for psoriasis, 9 out of 18 barriers for CSU, and 8 out of 18 barriers for AD were negatively associated with prescription behaviour, having an adjusted odds ratio (aOR) including a 95% confidence interval (95% CI) of less than 1.0. For psoriasis, lowest aORs were found for “no experience with biologicals” (0.13; 0.05–0.30), “complexity of medical pre-examination” (0.21; 0.11–0.43), “lack of time for treatment adjustment” (0.24; 0.12–0.50), and “insufficient knowledge” (0.24; 0.10–0.55). For CSU, lowest aORs were found for “insufficient efficiency” (0.09; 0.01–0.73), “inappropriate risk benefit profile” (0.22; 0.06–0.82), and “no experience with biologicals” (0.22; 0.1–0.45). For AD, lowest aORs were found for “insufficient efficiency” (0.09; 0.01–0.70)), “inappropriate risk benefit profile” (0.13; 0.03–0.58), “insecurity with guidelines” (0.19; 0.08–0.48), and “no experience with biologicals” (0.20; 0.10–0.42). Finally, biologicals were prescribed more frequently for the treatment of CSU by male doctors than by female doctors and more frequently for the treatment of AD in Lower Saxony than in Bavaria (Table SII).
Multivariate logistic regression for the prescription behaviour in psoriasis identified the barriers “no experience with biologicals” (0.11; 0.04–0.33), “complexity of medical pre-examination” (0.30; 0.12–0.74), and “high costs” (0.40; 0.20–0.81) as negative predictors associated with a low prescription rate (Fig. 3A). “No experience with biologicals” was identified as the only negative predictor for the prescription of biologicals in CSU (0.23; 0.10–0.50) (Fig. 3B) and AD (0.19; 0.09–0.44) (Fig. 3C).
Fig. 3. Positive or negative associations of variables and barriers with the stated quantity of prescription of biologicals in the treatment of: (A) psoriasis, (B) chronic spontaneous urticaria and (C) atopic dermatitis. Multiple logistic regressions using the median split of the prescription of biologicals in the respective disease as dependent variable. Odds ratios (coloured columns) and 95% confidence intervals (corresponding lines) are given for each independent variable. The value “no barrier/ does not apply” was used as reference. For multivariate analysis, backward selection was used.
The aim of this study was to evaluate the prevalence of barriers to prescribing biologicals in the treatment of moderate to severe psoriasis, CSU, and moderate to severe AD for dermatologists working in office-based practices from 2 different German federal states (Bavaria and Lower Saxony). Strongest barriers were associated with “high therapy costs”, “low reimbursements”, and “fear of regress claims”. The barriers “no experience with biologicals”, “complexity of medical pre-examination”, and “high therapy costs” were found to be negatively associated with the prescription of biologicals.
Bavaria and Lower Saxony are large federal states located in the southern and in the northern part of Germany, which makes a direct comparison between them interesting due to their different geographical locations and local health regulations. The general characteristics of dermatologists from Bavaria and Lower Saxony were comparable regarding sex, age, professional experience, and workplace. Similarly, no significant differences in the prevalence of strong and moderate barriers to the prescription of biologicals were found between both federal states. The distribution of barriers appears to not be limited by region despite the different entities and associations that outline the guidelines for dermatological care, including those for the prescription of biologicals.
Annual patient numbers varied widely between individual dermatologists for all 3 diseases, demonstrating that the study population covered a broad professional spectrum. Mean annual patient numbers for moderate to severe psoriasis and AD were more than twice as high as that for CSU. Notably, the percentage of patients treated with biologicals was substantially higher for psoriasis than for the other diseases. This may be explained by the particularly severe disease symptoms, course, and comorbidities for psoriasis, as well as the long-time experience of using a variety of available biologicals to treat this disease (19, 30). The lower prescription of biologicals for CSU and AD may be explained by the limited experience and availability of biologicals, as only a single biological, dupilumab, has been approved for the treatment of AD as of September 2017 (31, 32).
The high incidence of strong barriers in the category “external factors” demonstrates that the prescription of biologicals is encumbered by economic and legal factors. This finding is in accordance with previous results for Bavaria from 2017 (28). Economic and legal barriers to the guidance-compliant prescription of biologicals have seemingly persisted in the last 3 years. In the categories “physicians’ concerns”, “patients’ concerns”, and “concerns with regard to biological themselves”, strong barriers were of much lower prevalence, emphasizing the importance of non-medical factors in the usage of biologicals.
Since biologicals have been shown to be highly effective in the treatment of chronic dermatological disease, it raises the question of how to improve the prescription of biologicals to benefit patient-centred care (24, 25, 33, 34). One method may be the clarification of existing regulatory guidelines for the prescription of biologicals to reduce uncertainties for the prescribing dermatologists. Furthermore, co-operation between German federal states, and amendments of guidelines to expand the usage of biologicals, may be advantageous, although difficult to realize due to the large number of regulatory and political entities involved in such a process.
Barriers to the prescription of biologicals because of “external factors” have been reported in other countries. In the USA, concerns have been raised regarding the high costs of biologicals (35, 36). Other barriers in this category, such as “low reimbursement” and “fear of regress”, are based on health regulations specific to Germany and, thus are probably less relevant for other countries. The prevalence of such barriers may be minimized in the future with the introduction of biosimilars, leading to a reduction in treatment costs (37). However, new requirements for cost reductions, such as biosimilar quotas (38), could possibly increase concerns and confusion among dermatologists and represent a newly emerging barrier.
When considering strong and moderate barriers together, the category “patients’ concerns” was the second most prevalent group. These patients’ concerns might be addressed by increasing the available information on biological therapies with online tools tailored to support patient decision-making (39) and by strengthening co-operation between dermatologists and patient representatives and organizations.
Barriers in the category “concerns with regard to biologicals themselves” were only of low prevalence and less related to the efficiency of biologicals and more to their safety and lack of necessity. These barriers may be further reduced by selecting biologicals with optimal efficacy and safety profiles for individual patients (40, 41).
Notably, dermatologists’ own concerns were mainly “complexity of medical pre-examination”, “lack of time for treatment adjustment”, and “no experience with biologicals”, with the latter being identified as a negative predictor for a higher prescription rate of biologicals in all 3 investigated diseases. This demonstrates the need for adequate professional education regarding the usage of biologicals in chronic skin diseases. Participating in professional seminars and co-operating with experienced physicians may address this need. For example, co-operation between private practitioners and clinics for the treatment of dermatological patients with biologicals was stated to occur frequently. Thus, there appears to be a working relationship in the investigated German federal states between dermatologists in private practice and hospitals. In the USA, the relationship between physicians in clinics and in private practices appears to be based mostly on competition and not on co-operation (42).
According to data from the German Association of Panel doctors (GKV) approximately 35% of all German office-based dermatologists prescribe 100% of all modern systemic therapies in psoriasis. As a consequence there is increasing specialization among the dermatologists accompanied by a loss of knowledge in a majority of dermatologists. This loss of knowledge needs also be addressed in future attempts to overcoming barriers.
Further research is necessary, with the goal of overcoming barriers to the prescription of biologicals, in order to improve patient-centred care in chronic dermatological diseases.
Study limitations and strengths
Several aspects must be considered when assessing the generalizability of findings and limitations of the study. The study being conducted in 2 different federal states does provide a broader perspective on the situation in Germany, but nevertheless does not consider information from all 16 federal states, which each have their own governing bodies and different regulations. A generalization of the present results for Germany as a whole is therefore not possible. Further limitations might result from a potential selection bias in favour of physicians regularly prescribing biologicals, whereas physicians disinterested in the usage of biologicals would be less likely to participate. In addition, only 3 chronic skin diseases were investigated. Furthermore, information on patients’ concerns regarding treatment with biologicals were not directly obtained from the patients themselves, but from their physicians. A potential limitation of the study may also arise from specifically asking questions for barriers aside the situation prior to the COVID-19 pandemic, during the difficult situation in physician’s practices in 2020. This might explain that the overall response rate of 20.4% is not as high as in a previous study (28), but still should be considered adequate under these special circumstances. A strength of this investigation is its anonymized approach, which probably minimizes any social desirability bias. The broad spectrum of participants regarding age, practice size, and work experience is a further argument for generalizability.
Conclusion
This study demonstrates the continuing prevalence of barriers to the prescription of biologicals in the treatment of moderate to severe psoriasis, CSU, and moderate to severe AD for dermatologists working in office-based practices. The strongest barriers are related to economic and legal issues, namely “high therapy costs”, “low reimbursements”, and “fear of regress claims”. These topics appear to remain inadequately addressed by existing regulatory guidelines in the German federal states of Bavaria and Lower Saxony. The barriers “no experience with biologicals”, “complexity of medical pre-examination”, and “high therapy costs” are found to be negatively associated with the prescription of biologicals. Overcoming these barriers may strengthen usage of modern therapies and thereby prioritize patient-centred care in chronic skin diseases. This goal may be achieved by improved education of dermatologists in legal, economic, and medical matters associated with the prescription of biologicals. Finally, despite the challenges that multiple regional governing entities pose, the clarification, harmonization, and amendment of existing regulatory guidelines in Germany to expand the allowed usage of biologicals is highly recommended.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize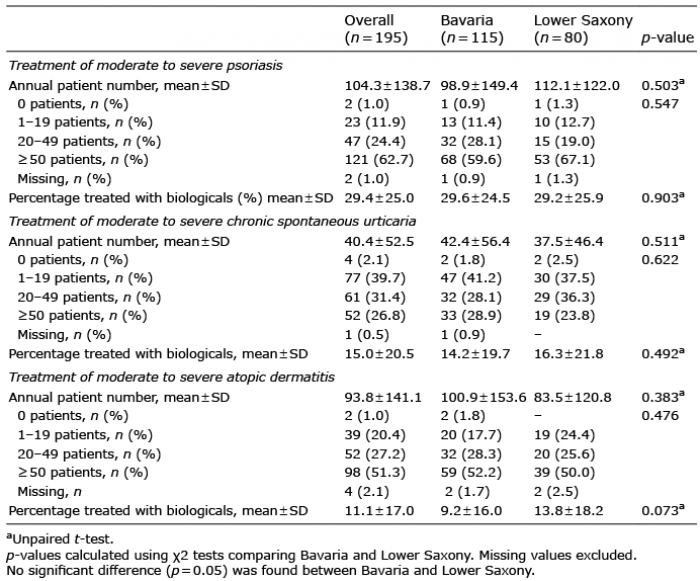 Click to show fullsize
Click to show fullsize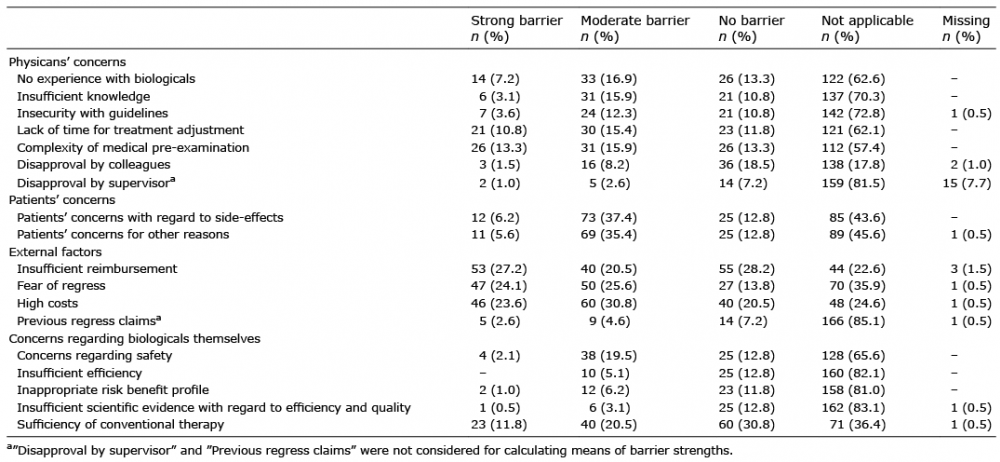 Click to show fullsize
Click to show fullsize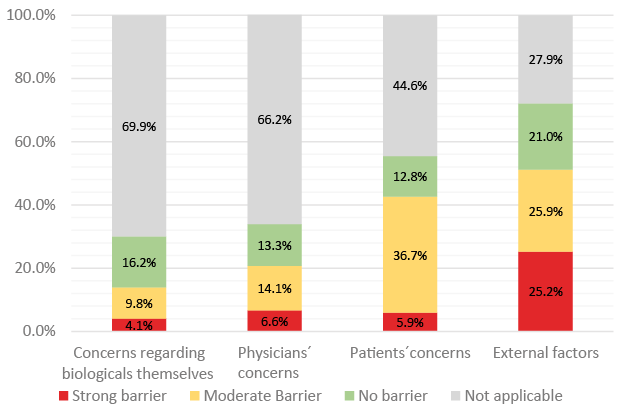 Click to show fullsize
Click to show fullsize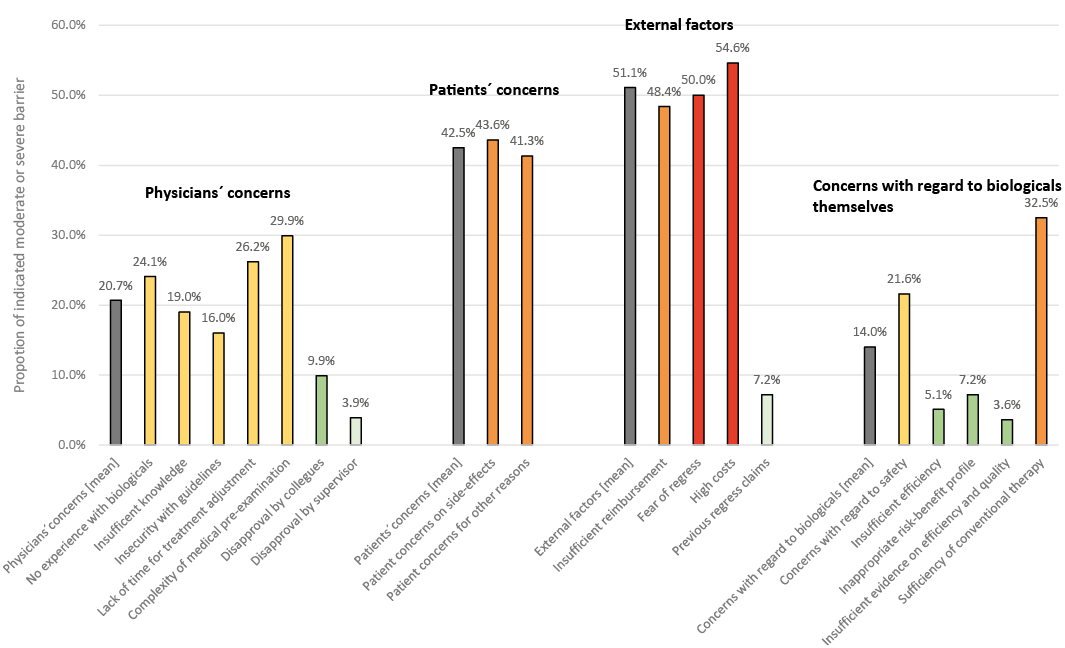 Click to show fullsize
Click to show fullsize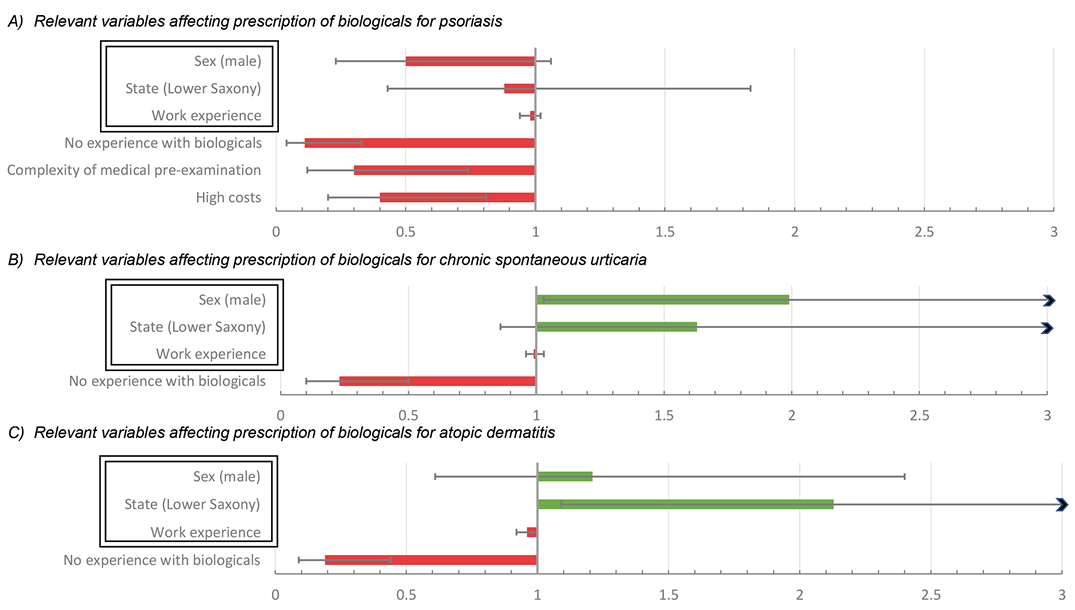 Click to show fullsize
Click to show fullsize