


1Copenhagen Center for Arthritis Research, Center for Rheumatology and Spine Diseases, Rigshospitalet, Glostrup, 2Department of Clinical Medicine, University of Copenhagen, 3Center for Rheumatology and Spine Diseases, Rigshospitalet, Copenhagen, and 4Department of Dermatology and Allergy, Herlev and Gentofte Hospital, University of Copenhagen, Hellerup, Denmark
A nationwide e-based survey of patients with psoriasis was preformed to assess the pattern of musculoskeletal pain and its influence on patient-reported outcomes, including health-related quality of life and disability. A total of 561 respondents (56% of the screened psoriasis patients) reported physician- diagnosed psoriasis and completed the questionnaire. Respondents were grouped based on the presence of musculoskeletal pain and/or diagnosed psoriatic arthritis: 81% had psoriasis without arthritis (29% pain now, 23% pain previously, 39% no pain ever), and 19% had psoriatic arthritis. Patients with psoriasis with pain now had poorer quality of life compared with patients without pain and, importantly, similar to that of patients with arthritis. Furthermore, patients with pain now/previously reported higher self-assessed severity of psoriasis and lower satisfaction with current treatment than patients without pain. Two-thirds of patients with psoriasis with pain now/previously and one-third of patients with arthritis had never been examined by a rheumatologist, demonstrating an unmet need for adequate evaluation of such patients.
Key words: psoriasis; psoriatic arthritis; musculoskeletal pain; quality of life; survey.
Accepted Aug 18, 2021; Epub ahead of print Aug 24, 2021
Acta Derm Venereol 2021; 101: adv00553.
doi: 10.2340/00015555-3906
Corr: Sara Kamp Felbo, Copenhagen Center for Arthritis Research (COPECARE), Center for Rheumatology and Spine Diseases, Rigshospitalet, Valdemar Hansens Vej 17, DK-2600 Glostrup, Denmark. E-mail: sarahelenakamp@gmail.com
Musculoskeletal pain is frequent in patients with psoriasis without diagnosed psoriatic arthritis. This study used a population-based survey of patients with psoriasis to describe the impact of musculoskeletal pain on health-related quality of life and disability. The results show that patients with psoriasis and musculoskeletal pain have decreased quality of life, to a similar level of that of patients with psoriatic arthritis. Many of these patients have never been examined by a specialist in musculoskeletal symptoms, demonstrating an unmet need for adequate evaluation and, possibly, treatment of such patients.
Psoriatic arthritis (PsA) is a diverse inflammatory disease that affects 10–30% of patients with psoriasis (PsO) (1, 2). PsA presents in different clinical forms, with various patterns of synovitis, enthesitis, dactylitis and/or axial inflammation, and with varying skin and nail involvement (3). These diverse manifestations, along with varying degrees of disease severity and activity, may complicate diagnosis. Early diagnosis and treatment of PsA is critical in order to limit pain, permanent joint damage and persistent psychological impact of the disease.
PsO, both with and without concomitant arthritis, has an impact on health-related quality of life (HRQoL), including almost all aspects of life, such as work and daily activities, leisure and social activities, clothing, sleep, and feelings of depression/anxiety (4–7). Presence of PsA has been reported to have a higher impact on all aspects of HRQoL than presence of PsO alone (6–8); in particular, daily routines, leisure/sports activities, sleep and work/education are affected (7). Musculoskeletal (MSK) pain is frequent in patients with PsO without diagnosed PsA (9), but the impact of MSK pain on HRQoL in patients without diagnosed PsA is poorly understood.
The aim of the current study was to use a large Danish population-based survey to assess the pattern of MSK pain in patients with PsO and its influence on important patient-reported outcomes including HRQoL and disability.
Survey population
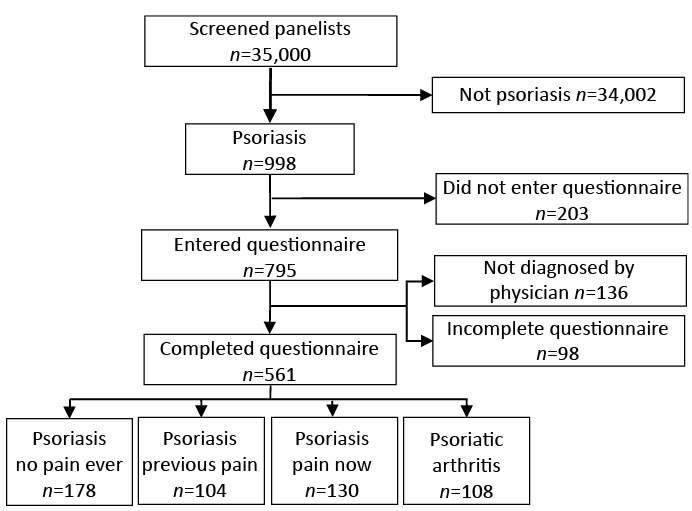
A national e-based questionnaire was performed among persons with self-reported PsO, carried out by the e-survey company “YouGov” using their panel in Denmark, which consists of individuals who participate in online studies on a wide variety of subjects. Fig. 1 displays the patient disposition. Panellists who self-reported PsO were invited by e-mail link to the survey and respondents completed an online questionnaire. The first question of the questionnaire was “Do you have psoriasis or psoriatic arthritis in any form” and participants indicating “ Yes, and I am diagnosed by a physician” continued to the full questionnaire.
Fig. 1. Patient disposition.
The study was approved by The Capital Region of Denmark Committee on Health Research Ethics (J. no. H-17032565).
Survey design
The questionnaire included 40 questions concerning skin and MSK symptoms, severity of disease, healthcare-contacts and treatment, and included standardized questionnaires on HRQoL (European Quality of life – 5 Dimensions (EQ5D (10)), Dermatology Life Quality Index (DLQI (11)) and Psoriatic Arthritis Impact of Disease (PsAID (12))) and disability (Health Assessment Questionnaire-Disability Index (HAQ (13)). A list of questions can be found in Appendix S1.
Musculoskeletal pain
Participants were divided into 4 groups, based on presence of PsA and presence of MSK pain. Participants indicating “Psoriatic arthritis” or “Both psoriasis and psoriatic arthritis” in answer to the question “Which type of psoriasis or psoriatic arthritis have you been diagnosed with by a physician?”, were grouped in the “PsA” group. Participants with PsO without PsA (“Psoriasis in skin, nails or scalp”) were asked: “Have you experienced pain in your joints or tendons?”, and were thereafter grouped in 3 subgroups: “PsO-no-pain-ever” (participants answering “No never”), “PsO-previous-pain” (participants answering “Yes, more than a year ago” or “Yes, within the past 12 months”), or “PsO-pain-now” (participants answering “Yes, I have it now”).
Statistical analyses
The characteristics of all participants and above-mentioned subgroups were described using descriptive statistics with numbers (%) for binary variables and medians (interquartile ranges) for continuous variables. For some analyses, groups were reduced to 3, with patients in the “PsO-previous-pain” group added to either the “PsO-no-pain-ever” group (“PsO-no-pain-now”) or the “PsO-pain-now” group (“PsO-pain-ever”). Differences between groups were compared; between multiple groups with χ2 test for binary data and Kruskal–Wallis test for continuous data, and between 2 groups (pairwise testing) with Fisher’s exact test for binary data and Mann–Whitney U test for continuous data. Correlations were calculated as Spearman’s correlation coefficient. Rho was defined as follows: negligible < 0.2, weak 0.2–0.39, moderate 0.40–0.59, strong 0.60–0.79 or very strong ≥ 0.80. Statistical significance was set at p < 0.05. Analyses were performed with R, version 3.6.1.
Participants
Of the 35,000 YouGov panellists screened for the presence of self-reported PsO, 998 (2.9%) indicated having PsO and were invited to participate in the survey. A total of 561 respondents (56% of panellists with self-reported PsO) reported physician-diagnosed PsO and completed the questionnaire between November 2018 and January 2020. Fig. 1 shows the patient disposition of screened and included patients, and the defined subgroups.
Demographics
Population characteristics for all respondents and subgroups are shown in Table I (demographics). Patients in the “PsO-previous-pain” and “PsO-pain-now” groups were generally younger, were more frequently female, had a higher BMI and had a higher frequency of not currently working/studying or being retired (i.e. on sick leave, early retiree, government subsidized job, unemployed or “other”) than patients in the “PsO-no-pain-ever” group. Smoking and alcohol use did not differ between the groups.
Table I. Demographics, clinical features of psoriasis/psoriatic arthritis, healthcare contacts, treatment, quality of life and disability of all patients and for defined subgroups
Clinical features of psoriasis and psoriatic arthritis
The prevalence of clinical features of PsO and PsA for all respondents and subgroups are shown in Table I (PsO/PsA features). To evaluate the prevalence of clinical findings in all patients with PsO and pain at some point, patients in “PsO-pain-now” and “PsO-previous-pain” were grouped as one: “PsO-pain-ever”. Overall, respondents had mostly mild psoriasis (body surface area; BSA) covered with psoriasis ≤ 3%). Patients in the “PsA” group reported higher BSA and higher frequency of psoriatic nail changes, dactylitis (sausage digit), and enthesitis (tender/swollen entheses) than patients without PsA. “PsO-pain-ever” reported frequencies of skin psoriasis features (BSA and nail psoriasis) comparable to “PsO-no-pain-ever”, but significantly higher frequencies of PsA features (dactylitis and enthesitis).
The location of skin psoriasis is shown in Fig. 2a and differed most between “PsO-no-pain-ever” and “PsA” groups. Specifically, armpits, toes and nails were more frequently affected in the latter (odds ratio (OR) 10, 5.6 and 4.8, respectively (data not shown)). The location of MSK pain in the “PsO-pain-ever” and “PsA” groups is shown in Fig. 2b. Pain in the wrists, ankles, fingers and toes were more frequent in the “PsA” group.
Fig. 2. Location of (a) psoriasis (past 12 months) and (b) musculoskeletal pain in patients in the defined subgroups. Statistical significance of pairwise test between the groups (by Fisher’s exact test) displayed as: *< 0.05, **< 0.01, ***< 0.001. PsO: psoriasis; PsA: psoriatic arthritis.
Healthcare contact and treatment
Data on contact with specialists in dermatology and rheumatology, time from symptom onset to diagnosis, and treatment are shown in Table I (healthcare contact and treatment). Most respondents had been examined by a dermatologist at some point, while frequency of examinations by a rheumatologist varied. Fig. 3 shows frequencies of contacts with dermatologist and rheumatologist in the 3 groups. It is noted that 72% of patients in the “PsO-pain-ever” group and 27% of patients in the “PsA” group, had never been examined by a rheumatologist. Time from onset of MSK symptoms to diagnosis of PsA (“PsA” group only) was longer (median 7.5 years) than time from skin-symptom onset to diagnosis of PsO (median 1.5 years). Treatment with both methotrexate and biological disease modifying anti-rheumatic drugs (bDMARDs) was more common in patients in the “PsA” group compared with the other groups, and the “PsO-pain-ever” group had significantly higher use of bDMARDs than the “PsO-no-pain-ever” group.
Fig. 3. Contacts to (a) dermatologist and (b) rheumatologist for patients in the 3 subgroups. PsO: psoriasis; PsA: psoriatic arthritis.
Patients’ perception of severity of PsO and PsA and satisfaction with current treatment was reported on a 5-level scale (Fig. 4). Severity of PsO (Fig. 4a) was perceived highest in patients in the “PsA” group, followed by “PsO-pain-ever” and “PsO-no-pain-ever”. Severity of PsA was reported higher than for PsO. Satisfaction with treatment of PsO (Fig. 4c) was relatively high in all groups, although lower in “PsO-pain-ever” compared with “PsO-no-pain-ever”. Satisfaction with PsA treatment was lower than for PsO (Fig. 4d).
Fig. 4. Self-assessed severity of (a) psoriasis and (b) psoriatic arthritis, and satisfaction with treatment of (c) psoriasis and (d) psoriatic arthritis in the defined subgroups. PsO: psoriasis; PsA: psoriatic arthritis.
Quality of life and disability
To evaluate the impact of current MSK pain on HRQoL and disability, patients in “PsO-no-pain ever” and “PsO-previous-pain” were grouped together (“PsO-no-pain-now”), see Table I (quality of life and disability). Patients in the “PsO-pain-now” group reported lower HRQoL (measured by DLQI score and EQ5D index and global visual analogue scale (VAS)) compared with patients in “PsO-no-pain-now”, and not significantly different from patients in the “PsA” group. Disability (HAQ) and PsAID scores were worse in the “PsA” group compared with the “PsO pain now” group (not evaluated in “PsO-no-pain-now”).
Subgroup responses to the individual items of EQ5D, DLQI and PsAID, respectively can be seen in Figs S1, S2 and S3. When comparing individual item scores between groups (data not shown) of DLQI, “PsO-pain-now” had significantly higher (poorer) scores on “itch, soreness”, “daily activities”, “clothing” and “treatment” than “PsO-no-pain-now”. No items differed significantly between “PsO-pain-now” and “PsA”. For EQ5D, “PsO-pain-now” had higher (poorer) scores on all items than “PsO-no-pain-now”, and only one item (“usual activities”) was significantly higher in the “PsA” group than the “PsO-pain-now” group. On the PsAID questionnaire, “PsO-pain-now” had lower (better) scores on all items than “PsA” apart from “sleep disturbance”, which did not differ significantly.
Correlations between the respondents’ self-assessed severity of PsO and PsA, and level of pain/discomfort (EQ5D pain/discomfort), and BSA, DLQI, EQ5D index and VAS, PsAID and HAQ for all respondents and for subgroups are shown in Table II. The correlation between self-assessed severity of PsO and BSA was moderate (rho 0.57 for all patients). Severity of PsO correlated strongly with skin-specific HRQoL (DLQI, rho 0.65, all patients) while correlations were weak to negligible with overall and arthritis specific HRQoL (EQ5D VAS, rho –0.29 and PsAID, rho 0.39, all patients). Self-assessed severity of PsA correlated best with overall HRQoL (EQ5D VAS, rho –0.50, all patients), as did the respondents’ level of pain (EQ5D index, rho –0.81, all patients).
Table II. Correlations between self-assessed severity of psoriasis and psoriatic arthritis, and level of pain/discomfort and different patient-reported outcomes
This population-based survey of Danish patients with PsO describes patterns of pain, skin symptoms, healthcare contacts, treatment, disability and HRQoL. MSK pain was frequent in patients with PsO without diagnosed PsA, and patients with PsO with MSK pain had lower HRQoL than patients with PsO without MSK pain. A high proportion of PsO patients with MSK pain had never been examined by a rheumatologist.
In all, 45% of respondents diagnosed with PsO, but without diagnosed PsA, reported MSK pain now or in the past 12 months. This is in line with a previous global survey, the Multinational Assessment of PsO and PsA (MAPP) study (9), and a Scandinavian survey, the NORPAPP-study (14), which found 44% and 42% of patients with PsO to have MSK pain, respectively. MSK complaints (discomfort/pain) is also frequent in the general Danish population (40%) (15). However, the pattern of complaints appears to be different, as they reported low back, neck, shoulders and knees being the most frequent sites of complaints in the general population (15), whereas the current study found that knees and fingers were the most common pain sites in patients with PsO. In the current cohort, patients with PsO with MSK pain reported more frequent dactylitis- and enthesitis-like symptoms than patients with PsO without MSK pain (15% vs 1% and 13% vs 2%). The numbers for patients with diagnosed PsA (41% and 42%) were comparable to those found in the MAPP-study (45% and 31%) (16). These results indicate that a noticeable proportion of patients with PsO with MSK pain may have undiagnosed PsA. Most of these patients (72%) had never been examined by a rheumatologist. As PsA may be a diagnostic challenge (17) this is a worryingly high number, suggesting that almost three-quarters of these patients have never had a clinical evaluation by a specialist to determine if their pain was a sign of PsA or due to other causes. Underdiagnosis of PsA in patients with PsO has previously been recognized in other cohorts (1, 8, 18), with lack of awareness of PsA among physicians and patients as a possible explanation (19).
The frequent delay in diagnosis of PsA is also documented by the long time from onset of MSK symptoms to PsA diagnosis in participants with physician-diagnosed PsA: a delay which has also been identified by rheumatologists as the greatest challenge in managing PsA (20). In patients with PsA, 27% reported never having been examined by a rheumatologist. Furthermore, many patients with PsA were not satisfied with their arthritis treatment, whereas they reported that treatment of the skin component was satisfactory. This, in combination with a low treatment rate (29% for methotrexate and 16% for bDMARDs), indicates that PsA is not only underdiagnosed, but seemingly also undertreated. This bDMARD treatment rate is in line with the MAPP-study (14%) (16), whereas the NORPAPP-study found higher treatment rates (bDMARD 31.8%) (21) and fewer patients with PsA who had never seen a rheumatologist (14.3%). Differences could be related to regional differences in healthcare organization and prescribing patterns.
Both self-assessed severity of PsO and satisfaction with current treatment for PsO were lower in patients with PsO with MSK pain compared with patients with PsO without pain. This was not explained by their BSA severity, supporting the importance of pain for the patient’s perception of health. Work productivity has previously been reported lower in patients with PsA than in patients with PsO alone (7, 8). The current study used a simple status as currently being/not being occupied with work (full- or part-time), studies or being retired, and it was found that patients with PsO with MSK pain had higher rates of “not currently being occupied” than patients with PsO without pain and not statistically significantly different from patients with PsA, suggesting that MSK pain is important for work productivity in patients with PsO.
Quality of life is known to be affected by PsO (4) and even more by concomitant PsA (2, 16, 22). Although skin-specific HRQoL (DLQI) showed no or small effect of PsO on patient’s life (median score <5) for all subgroups in this study, patients with PsO and current MSK pain reported significantly higher DLQI than patients with PsO without MSK pain, despite their BSA not being higher. The difference was most prominent for questions on itching, soreness etc. of the skin, affection of daily activities and issues regarding treatment. All specific areas of general HRQoL (EQ5D mobility, self-care, usual activities, pain/discomfort, anxiety/depression), as well as overall measures (EQ5D index and VAS), were also reported worse by patients with PsO with MSK pain than patients with PsO without MSK pain, and was not significantly different from patients with diagnosed PsA. Taken together, this indicates that MSK pain is an important contributor to the disease impact. Other factors associated with worse HRQoL in patients with PsO are female sex, younger age, and more clinically severe disease (higher psoriasis activity and severity index) (4). Patients with PsO with MSK pain in the current study cohort were indeed younger and more frequently female, which may have affected the results, but did not have higher BSA. Patients with PsA reported higher disability score (HAQ 0.875) than patients with PsO and MSK pain (0.5), as also reported in the MAPP-study (modified HAQ 0.49 and 0.39, respectively) (9).
When correlating self-assessed disease severity with patient-reported outcomes, the current study not surprisingly found that PsO severity correlated better with skin-specific measures (DLQI and BSA) than arthritis-specific (PsAID) or general measures (EQ5D). Conversely, severity of PsA correlated better with arthritis and general measures than skin-specific measures. The level of pain/discomfort was strongly correlated with EQ5D, PsAID and disability, with highest correlations in the PsA group. DLQI had better (but still weak) correlations with pain/discomfort in patients without MSK pain than in patients with MSK pain or PsA, indicating that their response might be more related to skin-pain/discomfort.
The strengths of the current study include that patients were not identified at dermatology departments or through patient organizations, and may therefore be perceived to better represent the broad population of people with PsO and PsA, as many patients with PsO do not regularly see healthcare personnel for their condition (9). Furthermore, we used standardized, validated patient-reported outcome measures, making direct comparisons with other studies possible (4).
The current study is limited by factors related to all surveys, such as participants’ correct recall of facts (recall bias) and understanding of questions (response bias). The specific diagnoses of PsO and PsA also rely on physicians giving the correct diagnosis and on patients correctly understanding the diagnoses given. While the misdiagnosis rate for PsO is presumably the same in all subgroups, and therefore would not largely affect these comparisons, a misdiagnosis of PsA could affect subgroup comparisons. In addition,YouGov panellists may, despite representable sex and age distributions, represent a population active in finding information, which might therefore have better coping strategies (7).
In conclusion, almost half of patients with PsO without diagnosed PsA have MSK pain, and this subgroup of patients has significantly worse HRQoL compared with patients with PsO without MSK pain (at a level comparable to patients with PsA). Three out of 4 patients have never been examined by a rheumatologist. This demonstrates an unmet need for adequate evaluation of the cause of pain, as early diagnosis and treatment of possible PsA could improve quality of life and prevent further deterioration in physical functioning in these patients.
The authors acknowledge the participating respondents who contributed to this study. The study was financially supported by research grants from Amgen, Celgene and The Danish Rheumatism Association. The Danish Rheumatism Association and The Danish Psoriasis Research Foundation have supported the work of SKF. The sponsors had no influence on study design, data analysis or manuscript preparation.
Conflicts of interest. SKF received research support from Amgen/Celgene. Lene Terslev received speaker’s fee from AbbVie, Janssen, Roche, Novartis, Pfizer, MSD, BMS and GE. IJS have nothing to disclose. LS has been a paid speaker for AbbVie, Eli Lilly, Novartis, and LEO Pharma, and has been a consultant or has served on Advisory Boards with AbbVie, Janssen Cilag, Novartis, Eli Lilly, LEO Pharma, UCB, Almirall, Bristol-Myers Squibb, and Sanofi. She has served as an investigator for AbbVie, Sanofi, Janssen Cilag, Boehringer Ingelheim, Pfizer, AstraZeneca, Eli Lilly, Novartis, Regeneron, and LEO Pharma, and has received research and educational grants from Novartis, Sanofi, Bristol-Myers Squibb, Janssen Cilag, and LEO Pharma. CZ has been a scientific consultant, advisor, investigator, or speaker for Eli Lilly, Jansen Cilag, Novartis, Abbvie, Takeda, Amgen, Almirall, CSL, UCB, Regeneron, MSD, and Leo Pharma. MØ received research support, consultancy fees and/or speaker fees form AbbVie, BMS, Boehringer Ingelheim, Celgene, Eli-Lilly, Hospira, Janssen, Merck, Novartis, Novo, Orion, Pfizer, Regeneron, Roche, Sandoz, Sanofi and UCB.


 Click to show fullsize
Click to show fullsize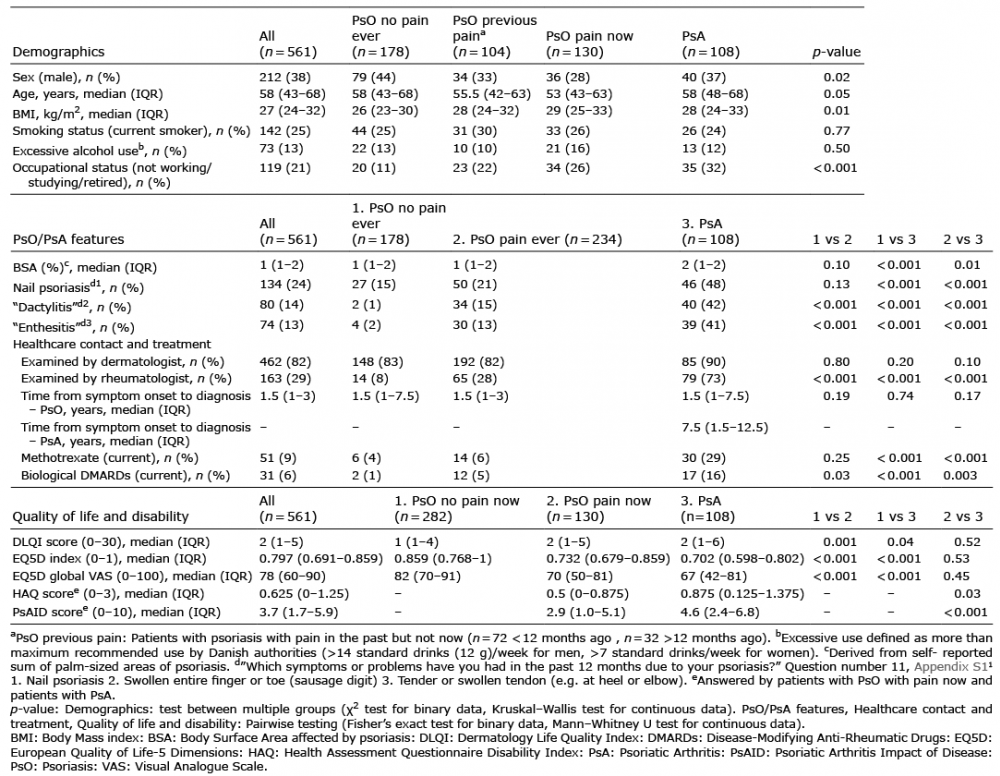 Click to show fullsize
Click to show fullsize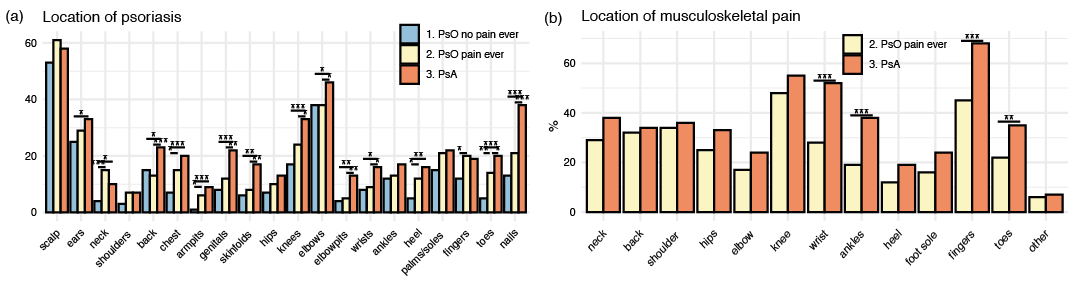 Click to show fullsize
Click to show fullsize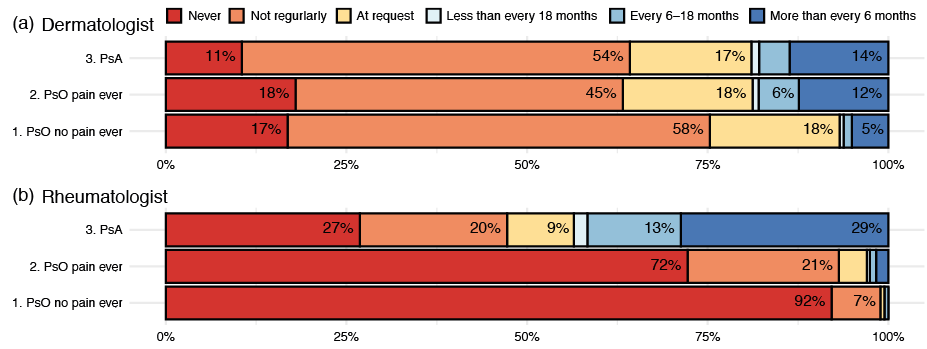 Click to show fullsize
Click to show fullsize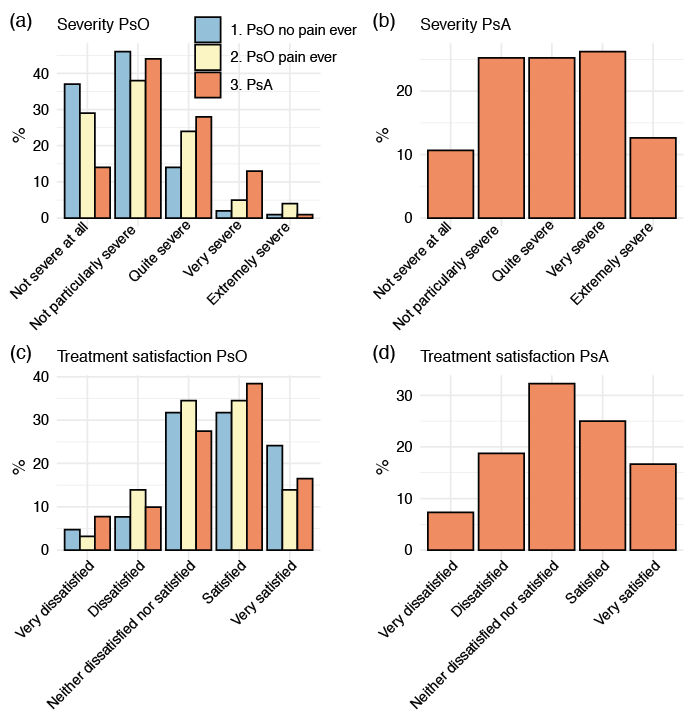 Click to show fullsize
Click to show fullsize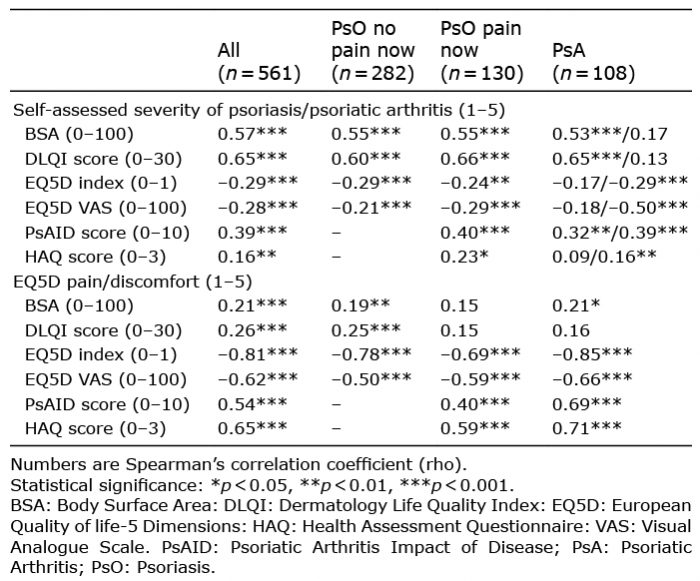 Click to show fullsize
Click to show fullsize