BACKGROUND: More evidence of the efficacy of caregiver interventions is needed. The aim of this study was to evaluate whether counselling in the home setting reduces the caregiver burden.
METHODS: Thirty-six patients after stroke, median age 53 years, with a close family member, were selected for an evaluation of the burden of care and 35 participated. They were part of a randomized controlled trial, comparing rehabilitation in the home setting with outpatient rehabilitation. In the home setting, counselling about the stroke and its consequences was included. Assessments with the Caregiver Burden scale were made at 3 weeks, 3 months and one year after discharge.
RESULTS: The burden of the 2 groups did not differ. After the intervention, there was a tendency to a lower burden for the home setting. The burden for the home setting was then unchanged from 3 weeks to 1 year, while outpatient rehabilitation showed a reduced burden over time. For the home setting, significant correlations to activity level were seen after the intervention.
CONCLUSION: A positive effect of counselling was seen, as the home setting burden tends to be lower after the intervention, while outpatient rehabilitation seems to adjust with time. The results suggest that counselling reduces burden and the remaining burden is associated with the patient’s ability.
Key words: caregiver, impact, intervention, longitudinal, activities of daily living, cognition, motor skill.
J Rehabil Med 2007; 39: 27–32
Correspondence address: Ann Björkdahl, Guldhedsgatan 19, 413 45 Göteborg, Sweden.
E-mail ann.bjorkdahl@rehab.gu.se
Submitted October 24, 2005; accepted May 23, 2006
1This article has been fully handled by one of the Associate Editors, who has made the decision for acceptance, as it originates from the institute where the Editor-in-Chief is active.
INTRODUCTION
In recent years a number of studies concerning caregiver burden, caregiver strain and emotional well-being have been published and almost all of them stress the high demands on the caregivers of patients after stroke (1–5). Several studies have tried to identify which factors impact the most on the subjective caregiver burden. In a study from Australia with a populationbased assessment of the impact of burden for long-term stroke survivors there was no significant relationship between emotional illness among caregivers and the degree of a patient’s physical disability (1). Nor was physical disability after stroke related to caregiver depression (2). Scholte op Reimer et al. (6) noted that partners of patients after stroke perceived most caregiving burden in terms of feelings of heavy responsibility, uncertainty about the patient’s care needs, constant worries, restraints in social life and feelings that patients rely on only their care. Several studies have found anxiety both in patients and caregivers to be an important factor of burden (7, 8). At the 3-month follow-up, patient and caregiver anxiety were the only significant independent determinants of caregiver burden in the study by McCullagh et al. (8). Decreased satisfaction with the amount of social contact, increased concern for providing future care, and a decrease in the positive personality characteristics of the former patient’s after stroke were factors associated with a higher burden for the primary support persons, in a study by Schulz and co-workers (9). The sense of coherence of the caregivers, which refers to one’s ability to respond to stressors, has also been found to relate to degree of burden and indicates that factors other than the direct effect of the stroke influence burden (10, 11).
Training for caregivers of patients after stroke in basic nursing and facilitation of personal care techniques during the patient’s rehabilitation reduced costs and caregiver burden and improved psychosocial outcomes in caregivers and patients (12). From the same study, McCullagh et al. (8) found that the training of caregivers in the management of disabled patients had an independent effect on reducing caregiver burden. Low et al. (13) draw the conclusion from their review that carers’ ability to cope with the stroke was enhanced both by the use of positive coping strategies and by stroke information. In a recent review of intervention studies for caregivers of stroke survivors, the conclusion was that there was not sufficient evidence to confirm the efficacy of interventions for caregivers but counselling programs appeared to have the most positive outcome (14). In a study from the Netherlands, comparing a group support program and a home visiting program for family caregivers, they found that both intervention programs were feasible and suggested a match of intervention type according to specific caregiver characteristics (15). Intervention types vary in their benefits: persons in the home visiting program in this study reported a lack of contact with fellow caregivers, whereas some of the group participants reported a lack of attention to their individual problems.
There is still a need for further investigation of what affects caregiver burden and how to influence the degree of burden with interventions. The aim of this study was to evaluate if an intervention with information about stroke and its consequences, as well as practical advice and training in the home setting reduces or affects the burden of care for next-of-kin. In order to achieve this, a randomized controlled study was performed with intervention in the home setting compared with ordinary day rehabilitation.
MATERIAL AND METHODS
Patients
Thirty-six patients with a prior stroke that had someone close (cohabitant) who could answer the questionnaire were selected for an evaluation of the burden over time of informal caregivers, i.e. family. They were part of a randomized controlled study of 59 patients, comparing rehabilitation in the home setting (the home group) with outpatient rehabilitation at the clinic (the day clinic group). From the possible 36 next-of-kin, one did not answer the questionnaire on any occasion, so the total number of responders was 35 (Table I). The sample of patients was quite well recovered, with a median score on the National Institute of Health Stroke Scale (NIHSS) of 5 (maximum score 36, the lower score the less deficit) and a median sum score of 76 (maximum score 91, which means total independence) on the Functional Independence Measure, FIMTM motor scale at discharge from the rehabilitation ward. The groups did not differ in any aspect. The Ethics Committee at Göteborg University approved of the study.
| Table I. Descriptives of the 2 groups of patients after stroke |
| | Home group | Day clinic group | Total |
| Patients in the randomized study 3 | 0 | 29 | 59 |
| Patients with a next-of-kin | 19 | 17 | 36 |
| Median age of patients (years) | 53 | 53 | 53 |
| Time since onset of stroke (mean days) | 88 | 89 | 89 |
| Next-of-kin answering questionnaire (n) | 18 | 17 | 35 |
| Number of husbands as responders | 6 | 3 | 9 |
| Number of wives as responders | 12 | 12 | 24 |
| Number of grown-up children answering | 0 | 2 | 2 |
| Families with children under the age of 18 years | 2 | 1 | 3 |
Intervention
The intervention began directly after discharge from the rehabilitation ward and lasted for 3 weeks. In the home group, family or friends and helpers were involved and information was given to them and the patient about the stroke, its consequences and how to deal with them. An occupational therapist and a physiotherapist offered individually tailored training, based on the patient’s needs and desires, focussing on activities in their natural context; a top-down approach to facilitate adaptation. The content varied from personal care to shopping and trying out leisure activities. As skills and strategies were directly implemented into real life it was easy for the family members to follow the progress and be aware of the ability of the patient. A multiprofessional team offered training at the day clinic to which the person commuted 3 times a week. There was a possibility for the next-of-kin to participate occasionally. However, this was not always feasible due to working hours, etc. for the next-of-kin. Therefore, over all accessibility for the family was not as easy as for the home group, and fewer opportunities were given to ask questions and get direct answers in conjunction with the training. The focus of the intervention in the day clinic group was more a bottom-up approach that focused on the training of deficits or components of function (impairment), and therefore it became more difficult for the patient as well as for the next-of-kin to understand how things at the clinic could be transferred into real life.
Instruments
Caregiver burden was assessed with the Caregiver burden scale (CB scale) (16). It is a questionnaire with 22 questions (answered in written by the carer) concerning burden from the aspects of the caregiver’s health, feeling of psychological well-being, relations, social network, physical workload and environmental aspects that might be important. When the scale was developed, factor analysis was used to yield 5 indices – general strain (8 questions), disappointment (5questions), isolation (3 questions), emotional involvement (3 questions) and environment (3 questions) (16). The items are scored from 0 to 3 (Not at all, Hardly, Somewhat and Definitely), maximum score 66. In the randomized study of home rehabilitation several instruments were used to measure different aspects of outcome. In order to investigate which aspects might influence burden, the CB scale was used as a measure of burden and was correlated with the following instruments: the FIMTM (divided into Motor score and Social/cognitive score), Assessment of Motor and Process Skills (AMPS), European Brain Injury Questionnaire (EBIQ), patient and close relatives version, the questionnaire of Life satisfaction by Fugl-Meyer (17) (LiSat 9, the overall factor Life in general), NIHSS and Barrow Neurological Institute Screening of higher cerebral functions (BNIS). The NIHSS and BNIS measured body functions, such as physical and cognitive function (18, 19). The FIMTM and AMPS evaluated activity limitations (20, 21). The EBIQ is a questionnaire concerning perceived social, cognitive and emotional problems of the stroke victim, which was given both to the patients and to the next-of-kin (22). The aspect of life satisfaction was only available from the patient (LiSat 9).
Assessments
Blinded assessors made evaluations at discharge and after the intervention at 3 weeks as well as at follow-up at 3 months and 1 year after discharge. We believe that the burden of being a carer could not be assessed at discharge as caring until then had mostly been provided from the clinic. Therefore, the CB scale was not introduced until after 3 weeks of intervention.
Data analysis
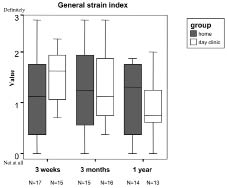
The number of questionnaires from the next-of-kin at the different occasions varied somewhat (home group n = 14 –17, day clinic group n = 13–16) (Fig. 1). The reason for missing data was due to non-responders from the next-of-kin; this was due to the fact of a positive response to be part of the study, but not being present at the meeting with the patient (forgetting to post the material).
Fig. 1. Distribution of the ‘‘general strain’’ index for the home group and the day clinic group at the different assessments, 3 weeks, 3 months and one year after discharge. Median values, 10th, 25th, 75th, 90th percentiles are given.
We used the Mann-Whitney U test to analyse differences between the groups on the CB scale. The analyses were made on the total score and the 5 indices. Each of the groups was also analysed with the Sign test, the test for paired samples, in order to analyse how the burden in the groups changed over time. The test was made between the 3-week evaluation and 3 months, between 3 months and one year as well as between 3 weeks and one year. The significance level was set at p < 0.05.
The aspects that was assumed might relate to burden were physical and cognitive impairment (NIHSS, BNIS), dependence in personal care (FIMTM) instrumental activity limitations (AMPS), the patient’s and next-of-kin experience of social, cognitive or emotional problems after the stroke (EBIQ) and the patient’s life satisfaction (LiSat 9). In order to analyse how these aspects might influence the caregiver burden, total score and the ‘‘general strain’’ index of the CB scale were used. The reason for using the ‘‘general strain’’ index was that it seemed to be the one most likely to be affected by an intervention of information and guidance. The correlations were made by data from discharge correlated to the CB scale from 3 weeks after discharge. Correlations were also made with data from the follow-up at one year in order to investigate whether the impact was the same later on in the rehabilitation. To detect differences between the groups the correlations were made with the 2 groups separately. In order to reduce the risk of mass significance a higher level of significance was used for the correlations, p < 0.01.
RESULT
The response rate was 80% of the available sample for caregiver’s burden, assessed over time (i.e. 2 occasions). All but one of the next-of-kin acknowledged burden in at least some of the questions of caregiver’s burden, at the first assessment. The maximum sum score of the CB scale is 66 and reflects a definite burden on all questions. The median sum score of the sample was 27 (0–52) at 3 weeks, 21 (0–50) at 3 months and 19 (0–45) at the 1-year follow-up.
Between the 2 groups there were no significant differences either on total score or on the different indices on any of the CB scale assessments. Concerning change over time, the only significant change was found for the day clinic group, between 3 months and one year on the ‘‘general strain’’ index. A visual analysis of Fig. 1 suggests a tendency to a lower burden on the ‘‘general strain’’ index for the next-of-kin in the home group compared with the next-of-kin in the day clinic group at 3 weeks. The burden for the home group stays about the same on the 2 follow-up assessments. At the same time the day clinic group, with a higher burden at 3 weeks, has a reduced burden over time and the largest reduction is seen between 3 months and one year, which also is verified with the Sign test as significant. As an example of this tendency, the question in the ‘‘general strain’’ index ‘‘Do you sometimes feel as if you would like to run away from the entire situation you find yourself in?’’ was acknowledged by 30% of the next-of-kin in the home group and 60% in the day clinic group at 3 weeks, but at one year the numbers were 50% in the home group and 40% in the day clinic group. On the other 4 indices both groups were similar.
Correlations were performed both with total score CB scale and the ‘‘general strain’’ index and they gave similar results, i.e. the same correlations, but with the ‘‘general strain’’ index giving stronger or significant correlations. Therefore, we have chosen to present the results of the correlations with the ‘‘general strain’’ index (Table II). The burden of caregivers in the home group correlated significantly, at 3 weeks, with FIM motor scale, FIM social/cognitive scale, AMPS process skill and the EBIQ completed by the next-of-kin. Also at 3 weeks, the burden of the day clinic group did not correlate with any instrument other than the EBIQ completed by the next-of-kin. At the 1- year follow-up there were significant correlations in the day clinic group between the burden of caregivers and the patient’s life satisfaction, FIM social/cognitive scale, while no significant correlations were found for the next-of-kin in the home group. There were significant correlations between the burden of care and EBIQ by the next-of-kin for both groups.
| Table II. Goodman Kruskal’s Gamma correlations between the general strain index of the Caregiver burden scale and the instruments listed in the table with the values of correlation and significance |
| Instrument | Home group | Day clinic group |
| Value | p-value | Value | p-value |
| Discharge | | | | |
| LiSat 9, Life in general | –0.292 | 0.151 | –0.279 | 0.155 |
| FIM motor item | –0.504 | 0.003 ** | –0.265 | 0.287 |
| FIM social/cognitive item | –0.488 | 0.001*** | –0.021 | 0.918 |
| AMPS motor skill | –0.510 | 0.011 | –0.030 | 0.908 |
| AMPS process skill | –0.434 | 0.010** | 0.010 | 0.962 |
| NIHSS sum score | 0.256 | 0.206 | –0.098 | 0.707 |
| EBIQ patient sum score | 0.286 | 0.145 | 0.160 | 0.516 |
| EBIQ next-of-kin rating | 0.623 | 0.000*** | 0.486 | 0.006** |
| 1 year | | | | |
| LiSat 9, Life in general | –0.170 | 0.576 | –0.667 | 0.000*** |
| FIM motor item | –0.284 | 0.058 | –0.362 | 0.117 |
| FIM social/cognitive item | –0.225 | 0.267 | –0.697 | 0.000*** |
| AMPS motor skill | –0.122 | 0.554 | –0.111 | 0.653 |
| AMPS process skill | –0.373 | 0.081 | –0.123 | 0.629 |
| NIHSS sum score | 0.307 | 0.080 | 0.303 | 0.270 |
| EBIQ patient sum score | 0.130 | 0.632 | 0.569 | 0.025 |
| EBIQ next-of-kin rating | 0.674 | 0.000*** | 0.704 | 0.000*** |
| **p < 0.01, ***p < 0.001. AMPS: Assessment of Motor and Process Skills, NIHSS: National Institute of Health Stroke Scale, EBIQ: European Brain Injury Questionnaire. |
DISCUSSION
In this study where the intervention was aimed at facilitating adaptation to the new situation and the return home after a stroke, there were no significant differences between the 2 groups, on any of the assessments. However, there seems to be a tendency to a lower burden for the next-of-kin in the home group than for the next-of-kin in the day clinic group directly after the intervention. The burden of the home group then stayed similar from 3 weeks to one year, while the day clinic group had a reduced burden over time. Correlations with other instruments made in order to examine factors influencing burden showed significant correlations to activity level after the intervention, but only for the next-of-kin in the home group. There were 2 limitations in this study that made it difficult to detect a difference between the 2 interventions and groups. The first limitation was the small sample size and the use of an instrument (CB scale) with only 4 different levels of response, which required a large difference between the 2 groups to obtain significance. The other limitation was that we did not have data on the burden of the next-of-kin both before and after the intervention, which would have made it easier to draw conclusions about the effect of the intervention. However, if we had asked the next-of-kin about their burden before the intervention, which began the first day after discharge, it would have been difficult to get reliable data, as they not yet had taken care of the patient after the stroke other than for one or 2 days on some weekends.
To overcome this second limitation we tried to gather information from the tests for change of burden over time, together with the visual analysis of the box plots of the burden at different points in time, in order to make a hypothesis of the course of burden from discharge to the end of the intervention. There seems to be a small difference in burden between the groups at 3 weeks (after the intervention), with the next-of-kin in the home group experiencing less burden. This was exemplified above where the home group acknowledged less burden than the day clinic group, at 3 weeks, on the question ‘‘Do you sometimes feel as if you would like to run away from the entire situation you find yourself in?’’. At this period until the 3 week assessment, the intervention period, the home group had had the opportunity to discuss with the team about how to adapt to the new situation and how to support the patient; i.e. had received hands on support. From that point the next-of-kin in the home group stayed at a similar level of perceived burden during the first year after discharge. This was in contrast to the next-of-kin in the day clinic group, who perceived less burden over time, with also a significant change of burden between 3 months and one year. The obtained results could be due to the fact that the intervention may have reduced the initial burden of the next-of-kin in the home group, and this reduction sustained in part. The next-of-kin in the day clinic group did not get education and support to the same extent and had to learn about the stroke and how to deal with it through time, which would account for the tendency to a higher burden than the home group after the intervention followed by a reduction of burden through time. On some of the questions, as exemplified above, the burden of care was acknowledged more at one year than at 3 weeks in the home group. This can be due to the fact that we have no control over (or information about), the presence or absence of important persons who could give support at one year when the team no longer were doing this. The day clinic group, on the other hand, acknowledged less burden at one year than at 3 weeks, probably due to a gradual adaptation. There is some evidence in the literature that education and information reduce caregiver strain, which supports this hypothesis (14, 23).
The results from the correlations also support the hypothesis regarding the variation of burden through time. There can be various causes of perceived burden and therefore there may not be a direct relation to one instrument or aspect. In this study, however, after an intervention we get correlation to one aspect, i.e. activity level, but only for one of the groups, the home group. This may lead to the conclusion that there had been something in the intervention for the home group that had reduced some aspect of burden and what was still remaining was closely related to the patient’s level of functioning. With the design of the 2 interventions we wanted to test if the possibility for the patient and the next-of-kin of getting direct feedback on performance in the natural context with meaningful tasks and explanations as to why problems occur, as well as the possibility of discussing strategies to handle the problems, would make the next-of-kin less worried, more confident in what to expect of the patient and more able to support the stroke victim. The result from the correlations supports this theory as the burden in the home group correlated with the more objective measure of activity limitations. However, the EBIQ by the next-of-kin also correlated significantly with burden for both groups. This was not surprising, since the instrument concerns the degree of problems perceived by the caregiver, which is probably close to what is burdensome.
By the 1-year follow-up there was no longer any correlation between caregiver burden and level of functioning for either group. Instead the significant correlations at this point were on the instruments concerning satisfaction and the perception of degree of social, emotional and cognitive problems, together with the FIM social/cognitive scale, and this time only for the next-of-kin in the day clinic group. A possible explanation could be that without the easy access to information or education about the stroke, the next-of-kin and the patients will learn by themselves to handle the situation, but may feel unsatisfied as they lack enough knowledge about the causes of the problems as well as the understanding of the stroke consequences. None of the earlier studies aiming at explaining the impact of stroke on caregiver burden have included an intervention, such as for the home group in the present study, with possibilities for counselling. This might be part of the explanation for the results stating that caregiver burden not relates to the disability of the stroke victim (1, 2, 4, 6) or as in the case of Bakas et al. (24) who described time-consuming and difficult tasks as being predictive of negative caregiver outcome and Schulz et al. (9) reporting caregiver burden as being associated with the amount of social contacts and the feeling of control of their lives. The caregivers in these above mentioned studies were similar to the next-of-kin in the day clinic group in this study.
If the significant correlation of burden of the caregivers and the patient’s ability in the home group after the intervention was due to the intervention, why does this correlation not persist at the 1-year follow-up? Schulz et al. (9) examined the psychosocial impact of stroke on primary support persons and found different predictors of burden at different times. Their explanation was that in the beginning the physical sequel was the most obvious problem and created most distress and in addition the caregivers did not yet have enough experience with the condition to appreciate the potentially long-lasting impact on their own lives. If this is true it may contribute to an explanation of why the correlations between burden and functioning at 3 weeks have disappeared by the 1-year follow- up. In the caregiver burden scale some of the questions concern the constraints on the life of the next-of-kin the stroke causes and these may have become more significant by time. Another important factor of burden in the study by Schulz et al. (9) was a decrease over time in relationships with whom the caregivers could discuss problems associated with the stroke. During the intervention of the present study the family had access to counselling, which was not the case at one year.
Both in the present study and the one by Schulz et al. (9), the stroke was relatively mild, which may be of importance when generalizing the results to other samples. They also found that older age was associated with less distress and in the present study there was a relatively young sample. With younger patients after stroke the need for a next-of-kin would be less than with elderly because of the tendency for younger patients after stroke to make a more complete recovery (25). However, the elderly patients often also have an elderly next-of-kin, who often are more fragile than the younger next-of-kin. On the other hand rehabilitation of young patients after stroke is associated with a variety of social problems, including marital break-up, child-care responsibilities, and return to employment, which are uniquely important in this age group (25). In this sample there were 3 female stroke victims who were separated and the number is not very different from the normal population, but what is notable was that it was 3 females in a sample of 25 men and 9 women.
In the present study we have been able to show that there is a substantial burden on next-of-kin of ‘‘younger’’ patients after stroke, even though they are well recovered and able in basic activities such as personal care. Earlier findings suggest that information and counselling have a positive effect both on patient outcome and caregiver burden (13, 14) and in this study there are tendencies and significant findings, that put together, support these findings. However, the need to gather stronger evidence is apparent in order to be able to implement proper interventions.
ACKNOWLEDGEMENTS
We acknowledge the valuable scientific input of Professor Gunnar Grimby.
This study has in part been supported by the following: The Swedish Research Council (VR K2002-27-VX-14318-01A), the Swedish Foundation for Health Care Sciences and Allergy Research, the County of Västra Götaland, the Swedish Medical Society (Olle Höök), Wilhelm and Martina Lundgren Foundation, Asker Foundation, the Royal Scientific Society (KVVS), the Swedish Stroke Victim´s Association, The Swedish Order of St John, Wennerström Foundation, Linder Foundation, Hjalmar Svensson Foundation, Almlöv Foundation, Jakobsson Foundation, KappAhl Foundation.
REFERENCES
1. Anderson CS, Linto J, Stewart-Wynne EG. A population-based assessment of the impact and burden of caregiving for long-term stroke survivors. Stroke 1995; 26: 843–849.
2. Dennis M, O’Rourke S, Lewis S, Sharpe M, Warlow C. A quantitative study of the emotional outcome of people caring for stroke survivors. Stroke 1998; 29: 1867–1872.
3. Bugge C, Alexander H, Hagen S. Stroke patients’ informal caregivers. Patient, caregiver, and service factors that affect caregiver strain. Stroke 1999; 30: 1517–1523.
4. Wyller TB, Thommessen B, Sodring KM, Sveen U, Pettersen AM, Bautz-Holter E, et al. Emotional well-being of close relatives to stroke survivors. Clin Rehabil 2003; 17: 410–417.
5. van Exel NJ, Koopmanschap MA, van den Berg B, Brouwer WB, van den Bos GA. Burden of informal caregiving for stroke patients. Identification of caregivers at risk of adverse health effects. Cerebrovasc Dis 2005; 19: 11–17.
6. Scholte op Reimer WJ, de Haan RJ, Rijnders PT, Limburg M, van den Bos GA. The burden of caregiving in partners of long-term stroke survivors. Stroke 1998; 29: 1605–1611.
7. Smith LN, Norrie J, Kerr SM, Lawrence IM, Langhorne P, Lees KR. Impact and influences on caregiver outcomes at one year poststroke. Cerebrovasc Dis 2004; 18: 145–153.
8. McCullagh E, Brigstocke G, Donaldson N, Kalra L. Determinants of caregiving burden and quality of life in caregivers of stroke patients. Stroke 2005; 36: 2181–2186.
9. Schulz R, Tompkins CA, Rau MT. A longitudinal study of the psychosocial impact of stroke on primary support persons. Psychol Aging 1988; 3: 131–141.
10. Nilsson I, Axelsson K, Gustafson Y, Lundman B, Norberg A. Wellbeing, sense of coherence, and burnout in stroke victims and spouses during the first few months after stroke. Scand J Caring Sci 2001; 15: 203–214.
11. Forsberg-Wärleby G, Möller A, Blomstrand C. Spouses of first-ever stroke victims: sense of coherence in the first phase after stroke. J Rehabil Med 2002; 34: 128–133.
12. Kalra L, Evans A, Perez I, Melbourn A, Patel A, Knapp M, et al. Training carers of stroke patients: randomised controlled trial. BMJ 2004; 328: 1099.
13. Low JT, Payne S, Roderick P. The impact of stroke on informal carers: a literature review. Soc Sci Med 1999; 49: 711–725.
14. Visser-Meily A, van Heugten C, Post M, Schepers V, Lindeman E. Intervention studies for caregivers of stroke survivors: a critical review. Patient Educ Couns 2005; 56: 257–267.
15. Schure LM, van den Heuvel ET, Stewart RE, Sanderman R, de Witte LP, Meyboom-de Jong B. Beyond stroke: description and evaluation of an effective intervention to support family caregivers of stroke patients. Patient Educ Couns 2006; 62: 46–55.
16. Elmstahl S, Malmberg B, Annerstedt L. Caregiver’s burden of patients 3 years after stroke assessed by a novel caregiver burden scale. Arch Phys Med Rehabil 1996; 77: 177–1782.
17. Viitanen M, Fugl-Meyer KS, Bernspang B, Fugl-Meyer AR. Life satisfaction in long-term survivors after stroke. Scand J Rehabil Med 1988; 20: 17–24.
18. Brott T, Adams HP Jr, Olinger CP, Marler JR, Barsan WG, Biller J, et al. Measurements of acute cerebral infarction: a clinical examination scale. Stroke 1989; 20: 864–870.
19. Prigatano GP, Amin K, Rosenstein L. Validity studies on the BNI screen for higher cerebral functions. BNI Quarterly 1995; 9: 2–9.
20. Hamilton BB, Granger CV, Scherwin FS, Zielnzny M, Tashman JS. A uniform national data system for medical rehabilitation. In: Furhrer MJ, ed. Rehabilitation outcomes: analysis and measurements. Baltimore: Brookes Publishing Co; 1987, p. 137–147.
21. Fisher AG. AMPS, Assessment of Motor and Process Skills. Development, standardization and administration manual, Fifth edn. Fort Collins, Colorado: Three Star Press; 2003.
22. Teasdale TW, Christensen AL, Willmes K, Deloche G, Braga L, Stachowiak F, et al. Subjective experience in brain-injured patients and their close relatives: a European Brain Injury Questionnaire study. Brain Inj 1997; 11: 543–563.
23. Forster A, Smith J, Young J, Knapp P, House A, Wright J. Information provision for stroke patients and their caregivers. Cochrane Database Syst Rev. 2001: CD001919.
24. Bakas T, Austin JK, Jessup SL, Williams LS, Oberst MT. Time and difficulty of tasks provided by family caregivers of stroke survivors. J Neurosci Nurs 2004; 36: 95–106.
25. Teasell RW, McRae MP, Finestone HM. Social issues in the rehabilitation of younger stroke patients. Arch Phys Med Rehabil 2000; 81: 205–209.