OBJECTIVE: To study the effect of comorbidity on the course of physical functioning in patients after stroke and with multiple sclerosis.
SUBJECTS: Patients after a first-ever supratentorial stroke (n = 198), who had been admitted for inpatient rehabilitaion, and patients with recently diagnosed multiple sclerosis (n =146).
DESIGN: Prospective, observational study over a period of 3 years.
Measurements: Physical functioning was measured with the motor score of the Functional Independence Measure at baseline (time of diagnosis), and at 6 months, and 1 and 3 year follow-ups. Cardiovascular, respiratory, musculoskeletal, diabetes mellitus, and other comorbidities were measured at baseline.
RESULTS: Patients after stroke and multiple sclerosis with comorbidity showed a significantly lower level of physical functioning over all 4 measurements. There was no difference in the course of physical functioning between patients after stroke with and without comorbidity. In patients with multiple sclerosis, a greater decrease in physical functioning over the 3-year follow-up was found in patients with comorbidity of the musculoskeletal system compared with patients without.
CONCLUSION: These findings indicate that similar improvements in physical functioning can be expected during rehabilitation of stroke patients with comorbidity compared with patients without these conditions. In patients with multiple sclerosis, musculoskeletal comorbidity requires further attention because of its association with a greater decrease in physical functioning.
Key words: comorbidity, functional outcome, neurological disorders, rehabilitation.
J Rehabil Med 2009; 41: 322–326
Correspondence address: A. J. Dallmeijer, Department of Rehabilitation Medicine, VU University Medical Center, PO Box 7057, NL-1007 MB Amsterdam, The Netherlands. E-mail: a.dallmeijer@vumc.nl
Submitted April 3, 2008; accepted November 14, 2008
INTRODUCTION
Comorbidity is a complex phenomenon that is considered to affect the course and outcome of the rehabilitation process (1). It refers to the existence of a set of chronic conditions present in patients with a particular (index) disease, which are not directly related to this index disease (2, 3). In general, comorbidity has been shown to have a negative impact on functional status and quality of life, and leads to a higher use of healthcare services (3, 4).
It is well established that comorbidity has a negative impact on the level of physical functioning in patients with neurological disorders (1, 5–9), and that the occurrence of comorbidity varies by disease group and the severity of the disease (10). Comorbidity may be an important predictor of rehabilitation outcome, and may, as such, affect the planning of treatment and resources. However, despite the obvious difference in functioning between neurological patients with and without comorbidity, little is known about the influence of comorbidity on the course of functioning of neurological patients, especially in the longer term. Inconsistent results have been reported in studies investigating the effect of comorbidity on the course of functioning (recovery) in stroke rehabilitation (6, 9, 11, 12). Some studies found a negative impact of comorbidity on functional gain (improvements in functioning expressed per day) during rehabilitation (9, 11, 12), while another study reported no effects (6). In the longer term also, in the post-rehabilitation period, no effect of comorbidity was reported (9). Multiple sclerosis (MS) is, in contrast to stroke, a progressive neurological disease with an expected decline in functioning over years. Although comorbidity is expected to affect the course of functioning in patients with MS, the relationship between comorbidity and physical functioning has, to our knowledge, not been investigated in this patient group.
The purpose of the current study was to evaluate the effect of comorbidity on the course of physical functioning in patients with stroke and with MS over a period of 3 years after the diagnosis.
METHODS
Subjects and design
This project was carried out as part of a prospective study on functional prognosis in neurological disorders (the FuPro-study). Patients with a first-ever supratentorial stroke, who had been admitted for inpatient rehabilitation, and patients with a recently diagnosed MS (< 6 months after diagnosis) participated in this study. The study was approved by the medical ethical committees of the University Medical Center in Utrecht (stroke), and the VU University Medical Center in Amsterdam (MS).
Measurements
Physical functioning was measured with the motor score of the Functional Independence Measure (FIMTM) (13, 14). The FIMTM measures the degree of disability by measuring the level of independence in basic activities of daily living. The FIM motor scale consists of 13 items. Each item measures the level of dependency on a 7-point scale, ranging from complete dependence (score 1) to complete independence (score 7). Consequently, the FIM motor sum score ranges from 13 (complete dependence) to 91 (complete independence). Measurements were performed at baseline (time of the diagnosis or within 6 months), and at 6 months and 1- and 3-year follow-ups (after baseline).
Comorbidity was measured at baseline in both groups. In the stroke group, patients were asked if they had comorbidities in the following domains: cardiovascular, respiratory, musculoskeletal, diabetes mellitus, and other comorbidity. The answer (comorbidity “yes” or “no”) was registered for each domain. In the MS group, comorbidity was measured with the Cumulative Illness Rating Scale (CIRS) (15). The 13 CIRS items were converted to the comorbidity domains in the stroke group (see above). A CIRS score of 1 and higher was defined as having comorbidity. For both groups, the presence of comorbidity (comorbidity total) was reported as a dichotomous variable, defined as having comorbidity on at least 1 of the above-described domains, or not. Severity of MS was measured at baseline with the Expanded Disability Status Scale (EDSS) (16), and in patients after stroke with the Barthel Index (17).
Statistical analysis
The effect of comorbidity on the course of physical functioning was analysed in each patient group separately, using analysis of variance (ANOVA) for repeated measures, with the 4 repeated measures of the FIM motor score as dependent variables. The interactions between comorbidity and time (using the 4 repeated measurements) were evaluated. Two separate analyses were performed, using total comorbidity (having comorbidity “yes” or “no”), as independent variable in the first analysis, and using the 5 comorbidity domains (cardiovascular, respiratory, musculoskeletal, diabetes, other comorbidity) as independent variables in the second analysis. A Greenhouse-Geisser (GG) correction of the degrees of freedom was applied in case the assumption of sphericity was not fulfilled. All analyses were adjusted for age and severity of the disease by including these variables as covariates in the repeated measures analyses.
RESULTS
In the stroke group 265 patients were measured at baseline. Seven patients died within the first year, 12 patients had a recurrent stroke and were excluded from follow-up, 20 patients withdrew from the study or could not be traced. Nine patients had missing values for comorbidity and 19 patients missed one of the FIMTM measurements, resulting in a complete data-set for 198 patients. In the MS group, 156 patients were measured at baseline. Seven patients were lost to follow-up because they withdrew from the study and 3 patients had missing data on comorbidity or FIMTM, resulting in a complete data-set for 146 patients.
Baseline characteristics are shown in Table I. Patients with comorbidity were significantly older compared with patients without comorbidity in both stroke (p = 0.015) and MS (p = 0.032) groups. There was no significant difference in gender distribution between patients with and without comorbidity in both groups. Severity of the disease, measured with the Barthel Index at admission in the rehabilitation centre, showed no differences between groups in patients after stroke (p = 0.227). Patients with MS with comorbidity were more severely affected (had a higher EDSS score) than those without (p < 0.001).
| Table I. Characteristics of patients after stroke and patients with multiple sclerosis ( MS) at baseline |
| | Stroke (n = 198) | MS (n = 146) |
| No comorbidity (n = 80) | With comorbidity (n = 118) | No comorbidity (n = 81) | With comorbidity (n = 65) |
| Gender, men, n (%) | 42 (53) | 74 (63) | 27 (33) | 25 (38) |
| Age, years, mean (SD) [range] | 56.5 (10.5) [30–75] | 60.2 (10.6) [30–82] | 35.9 (9.5) [17–57] | 39.3 (9.6) [23–60] |
| EDSS, median (25–75 percentile) | – | – | 2.0 (1.5–3.0) | 2.5 (2.0–3.5) |
| BI, median (25–75 percentile) | 15 (10–19) | 13 (10–17) | – | – |
| EDSS: Expanded Disability Status Scale; BI: Barthel Index; SD: standard deviation. |
The frequency distribution of the comorbidity domains is listed in Table II. In the stroke group, 118 out of 198 (60%) patients reported any type of comorbidity. In the MS group, 65 out of 146 (40%) patients reported any type of comorbidity.
| Table II. Number of patients for each comorbidity domain, measured at baseline in the stroke and multiple sclerosis (MS) group |
| Comorbidity at baseline*, n (%) | Stroke (n = 198) | MS (n = 146) |
| Cardiovascular | 93 (47) | 7 (5) |
| Respiratory | 13 (7) | 8 (6) |
| Musculoskeletal | 8 (4) | 20 (14) |
| Diabetes | 23 (12) | 6 (4) |
| Other | 99 (50) | 44 (43) |
| Comorbidity total | 118 (60) | 65 (44) |
| *Stroke: at admission to inpatient rehabilitation; MS: within 6 months after definite diagnosis. |
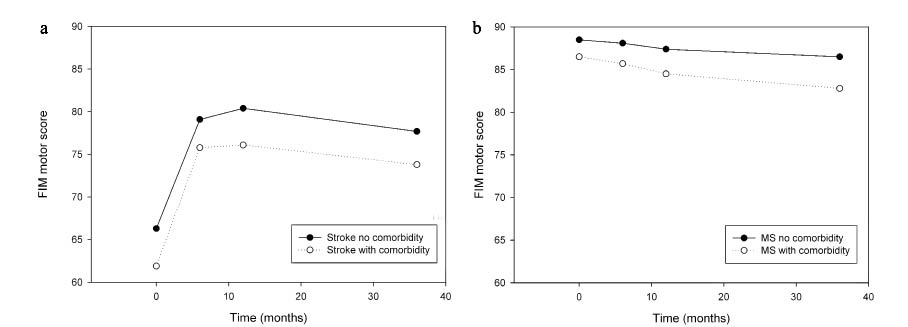
For patients with and without comorbidity, the 3-year course of physical functioning, expressed by the FIM motor scores are shown in Fig. 1a (stroke) and 1b (MS). FIM motor scores changed significantly over 3 years in both groups (p < 0.001), showing an initial improvement in stroke patients (in the first 6 months), followed by a stabilization of functioning, and a small gradual decrease over 3 years in the patients with MS.
The longitudinal analysis, adjusted for severity of the disease and age, showed that patients with comorbidity (total) had a significantly lower level of physical functioning compared with those without comorbidity in both groups (stroke: F(1,194) = 3.95, p = 0.048, MS: F(1,142) = 7.62, p = 0.007). Total comorbidity was, however, not related to the course of physical functioning in both stroke (F(3,582) = 0.22, p = 0.823, GG-epsilon = 0.74) (Fig. 1a) and patients with MS (F(3,426) = 2.22, p = 0.113, GG-epsilon = 0.64) (Fig. 1b), when adjusted for age and severity of the disease (Table III).
Fig. 1. Course of physical functioning (measured with Functional Independence Measure (FIM) motor score) in patients after (a) stroke and with (b) multiple sclerosis (MS), with and without comorbidity (raw data are pre- sented).
| Table III. Results of analysis of variance for repeated measures for patients after stroke and multiple sclerosis (MS), with Functional Independence Measure (FIM) motor outcomes at baseline, after 6 months and after 1 and 3 years as dependent variables |
| Independent variables | Crude model (no adjustments) | Adjusted for age and disease severity |
| F | df | p-value | Partial eta squared | F | df | p-value | Partial eta squared |
| Stroke total comorbidity |
| t × comorbidity total | 0.20 | 3, 588 | 0.812a | 0.001 | 0.22 | 3, 582 | 0.823b | 0.001 |
| Stroke comorbidity domains |
| t × comorbidity cardiovascular t × comorbidity respiratory t × comorbidity musculoskeletal t × comorbidity diabetes mellitus t × comorbidity other | 1.31 0.47 1.57 2.17 1.11 | 3, 576 3, 576 3, 576 3, 576 3, 576 | 0.271a 0.616a 0.210a 0.118a 0.328a | 0.007 0.002 0.008 0.011 0.006 | 1.81 0.20 0.18 1.46 1.30 | 3, 570 3, 570 3, 570 3, 570 3, 570 | 0.160c 0.895c 0.855c 0.232c 0.274c | 0.009 0.001 0.001 0.008 0.007 |
| MS total comorbidity |
| time × comorbidity total | 3.33 | 3, 432 | 0.040d | 0.023 | 2.22 | 3, 426 | 0.113a | 0.015 |
| MS comorbidity domains |
| t × comorbidity cardiovascular t × comorbidity respiratory t × comorbidity musculoskeletal t × comorbidity diabetes mellitus t × comorbidity other | 0.11 1.33 5.64 1.32 0.98 | 3, 420 3, 420 3, 420 3, 420 3, 420 | 0.894e 0.265e 0.004e 0.293e 0.377e | 0.001 0.009 0.039 0.009 0.007 | 0.18 1.71 5.50 1.38 0.36 | 3, 414 3, 414 3, 414 3, 414 3, 414 | 0.832a 0.184a 0.005a 0.252a 0.689a | 0.001 0.012 0.038 0.010 0.003 |
| df: degrees of freedom; t: measurements over time (baseline, after 6 months and after 1 and 3 years); a: Greenhouse-Geisser (GG) correction is applied with epsilon = 0.64; b: GG-epsilon = 0.74; c: GG-epsilon = 0.73; d: GG-epsilon = 0.63; e: GG-epsilon = 0.65. |
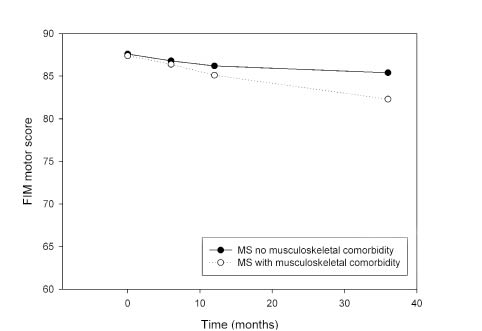
In the stroke group, no significant effects on the course of physical functioning were found when all comorbidity domains were included in the analysis (cardiovascular: F(3,570) = 1.81, p = 0.160, respiratory: F(3,570) = 0.20, p = 0.895, musculoskeletal: F(3,570) = 0.18, p = 0.855, diabetes: F(3,570) = 1.46, p = 0.232, other comorbidity: F(3,570) = 1.30, p = 0.274, GG-epsilon = 0.73) (Table III). When all 5 comorbidity domains were included in the analysis of the MS group, there was a significant effect of comorbidity of the musculoskeletal system domain on the course of motor functioning, showing a greater decrease in physical functioning in patients having comorbidity after 3 years’ follow-up (F(3,414) = 5.50, p = 0.005, GG-epsilon = 0.64). The other comorbidity domains had no significant effect on the 3-year course of physical functioning (cardiovascular: F(3,414) = 0.18, p = 0.832, respiratory: F(3,414) = 1.71, p = 0.184, diabetes: F(3,414) = 1.38, p = 0.252, other comorbidity: F(3,414) = 0.36, p = 0.689, GG-epsilon = 0.64) (Table III). Based on the estimated means of the ANOVA for repeated measured, a decline in physical functioning of (approximately) 5 points on the FIMTM was found in patients with MS with musculoskeletal comorbidity, compared with a decline of 2 points in patients without these conditions (Fig. 2). The analysis in both the stroke and MS group were adjusted for age and disease severity (Table III).
Fig. 2. Course of physical functioning for patients with multiple sclerosis (MS) with and without comorbidity of the musculoskeletal system. Estimated means from the repeated measures analysis of variance are presented.
DISCUSSION
The results of this study showed that comorbidity, existing early in the disease process, did not affect the 3-year course of physical functioning in stroke patients, while comorbidity of the musculoskeletal system did show a small, but significant, negative effect on the course of functioning in patients with MS. Obviously, there was an association between comorbidity and the overall level of function in both groups, which is consistent with previous studies in patients after stroke (5, 6, 9). The lack of effect of comorbidity on the course of functioning in patients after stroke, despite a clear relationship with the level of functioning, is in agreement with Giaquinto (6). They also found no effect of comorbidity on recovery during rehabilitation in stroke patients, measured with the FIMTM, and reported a correlation between comorbidity and FIMTM score both at admission and discharge of rehabilitation. Also Studenski et al. (9) found no relationship between comorbidity and changes in physical functioning in the post-rehabilitation period, using other indicators of physical functioning (Barthel Index, instrumented activities of daily living (IADL) and physical functioning scale). However, results were in contrast with other studies (11, 12) investigating the gain in functioning during rehabilitation, using FIMTM score improvements, or rehabilitation efficiency (FIMTM scores divided by the length of stay). An important difference between our study and most studies on comorbidity in stroke patients is that the latter investigated changes in functioning during rehabilitation, while in our study, patients were measured at fixed follow-up periods (at 6-months, 1- and 3-years), irrespective of the duration of the inpatient rehabilitation period.
The results of the current study indicate that patients with MS with comorbidity of the musculoskeletal system have a greater decline in physical functioning compared with patients with MS without these conditions. Although this effect is rather small (a 3 point greater decline on the FIM motor score), it seems a relevant difference when comparing it with the overall decline in physical functioning in the whole group. However, also at 3 years after the diagnosis the mean level of functioning is relatively high in the MS group. The greater decline in the last 2 years of the study shows that musculoskeletal problems are likely further to affect the course of physical functioning in the longer term. Given the mild status of the disease at the time of comorbidity measurement (baseline: within 6 months after the diagnosis), it might be expected that the comorbidity rate will increase with the duration of the disease. Musculoskeletal comorbidity was the most frequently reported type of comorbidity in the MS group (except for the “other comorbidity” category) with a percentage of 14%, which was similar to a previous study reporting a percentage of around 10% (10). Although the clinical relevance of the findings need to be confirmed in future studies, results suggest that clinicians should notice musculoskeletal problems in patients with MS.
The focus of this study was to investigate the effect of comorbidity at the onset of the disease, in order to be able to predict the effect on long-term outcome. However, the level of functioning might also be influenced by combinations of, or additional comorbid conditions that appeared during the course of 3 years. A cross-sectional study in a large group of chronic disease patients revealed a synergistic effect of comorbidity on physical and mental functioning (4). Due to the small sample size we were not able to take into account the effect of the combination of different types of comorbidity on the course of functioning. Another limitation of the present study is that only the effect of comorbidity on physical functioning is reported, while effects on social and cognitive functioning may also be expected. Although the FIMTM cognitive domain was also measured in the present study, the high level of cognitive functioning resulted in large ceiling effects on the FIMTM cognitive score for both groups, making meaningful analysis impossible.
Comparison of comorbidity research is hampered by the variation in methods that are used to measure comorbidity (18). We used the CIRS in the MS group and converted these data to the predefined domains that were measured in the stroke group. This procedure may have limited the comparison with former studies. Nevertheless, the results did not change for the MS group when using the original CIRS score in the analysis (results not shown). In addition, comparison with other studies may be hampered by differences in outcome measures to measure physical functioning. Although the FIMTM is often used, most studies reported the total FIMTM score, which combines the physical and cognitive domains, thus limiting the conclusions on each of the domains. Finally, differences in characteristics of the study population, such as severity of the disease and age, may also be responsible for the conflicting findings in the literature. For this reason, all analyses in the present study were adjusted for age and severity of the disease.
It is concluded that, although a lower level of physical functioning was found in patients with comorbidity in both patients after stroke and patients with MS, comorbidity did not affect the course of physical functioning in patients after stroke, while patients with MS with comorbidity of the musculoskeletal system showed a less favourable course. Although the clinical relevance of the latter findings, as well as the effects of musculoskeletal comorbidity on the longer term should be further investigated, results indicate that musculoskeletal problems should be taken into account when planning treatment in patients with MS.
ACKNOWLEDGEMENTS
This investigation was performed as part of the “Functional prognostication and disability study on neurological disorders”, supervised by the Department of Rehabilitation Medicine of the VU University Medical Center, Amsterdam, and was funded by the Netherlands Organization for Health Research and Development (grant: 1435.0001).
REFERENCES
1. Patrick L, Knoefel F, Gaskowski P, Rexroth D. Medical comorbidity and rehabilitation efficiency in geriatric inpatients. J Am Geriatr Soc 2001; 49: 1471–1477.
2. Elixhauser A, Steiner C, Harris DR, Coffey RM. Comorbidity measures for use with administrative data. Med Care 1998; 36: 8–27.
3. Gijsen R, Hoeymans N, Schellevis FG, Ruwaard D, Satariano WA, van den Bos GA. Causes and consequences of comorbidity: a review. J Clin Epidemiol 2001; 54: 661–674.
4. Rijken M, van Kerkhof M, Dekker J, Schellevis FG. Comorbidity of chronic diseases: effects of disease pairs on physical and mental functioning. Qual Life Res 2005; 14: 45–55.
5. DiLibero F, Fargnoli M, Pittiglio S, Mascio M, Giaquinto S. Comorbidity and rehabilitation. Arch Gerontol Geriatr 2001; 32: 15–22.
6. Giaquinto S. Comorbidity in post-stroke rehabilitation. Eur J Neurol 2003; 10: 235–238.
7. Lew HL, Lee E, Date ES, Zeiner H. Influence of medical comorbidities and complications on FIM change and length of stay during inpatient rehabilitation. Am J Phys Med Rehabil 2002; 81: 830–837.
8. Stineman MG, Ross RN, Williams SV, Goin JE, Granger CV. A functional diagnostic complexity index for rehabilitation medicine: measuring the influence of many diagnoses on functional independence and resource use. Arch Phys Med Rehabil 2000; 81: 549–557.
9. Studenski SA, Lai SM, Duncan PW, Rigler SK. The impact of self-reported cumulative comorbidity on stroke recovery. Age Ageing 2004; 33: 195–198.
10. Nuyen J, Schellevis FG, Satariano WA, Spreeuwenberg PM, Birkner MD, van den Bos GA, et al. Comorbidity was associated with neurologic and psychiatric diseases: a general practice-based controlled study. J Clin Epidemiol 2006; 59: 1274–1284.
11. Ferriero G, Franchignoni F, Benevolo E, Ottonello M, Scocchi M, Xanthi M. The influence of comorbidities and complications on discharge function in stroke rehabilitation inpatients. Eura Medicophys 2006; 42: 91–96.
12. Turhan N, Saracgil N, Oztop P, Bayramoglu M. Serum albumin and comorbidity relative to rehabilitation outcome in geriatric stroke, and possible links with stroke etiology. Int J Rehabil Res 2006; 29: 81–85.
13. Keith RA, Granger CV, Hamilton BB, Sherwin FS. The functional independence measure: a new tool for rehabilitation. Adv Clin Rehabil 1987; 1: 6–18.
14. Linacre JM, Heinemann AW, Wright BD, Granger CV, Hamilton BB. The structure and stability of the Functional Independence Measure. Arch Phys Med Rehabil 1994; 75: 127–132.
15. Linn BS, Linn MW, Gurel L. Cumulative illness rating scale. J Am Geriatr Soc 1968; 16: 622–626.
16. Kurtzke JF. Rating neurologic impairment in multiple sclerosis: an expanded disability status scale (EDSS). Neurology 1983; 33: 1444–1452.
17. Collin C, Wade DT, Davies S, Horne V. The Barthel ADL Index: a reliability study. Int Disabil Stud 1988; 10: 61–63.
18. de Groot V, Beckerman H, Lankhorst GJ, Bouter LM. How to measure comorbidity. a critical review of available methods. J Clin Epidemiol 2003; 56: 221–229.