Object: To describe self-reported life satisfaction of younger persons after stroke and to investigate differences between men and women and factors associated with life satisfaction.
DESIGN: A cross-sectional study.
METHODS: Subjects were all persons after stroke, aged 18–55 years, registered in the Swedish National Quality Register for Stroke Care. A questionnaire was completed by 1068 individuals 8–36 months after stroke. Perceived Life Satisfaction was measured with LiSat-9.
RESULTS: Less than half of the participants were satisfied with life as a whole. For women, significant associations were found between not being satisfied with life as a whole and haemorrhage (odds ratio (OR) 4.00) as well as a deteriorated ability to concentrate (OR 2.11). For men, significant associations were found to be not having a significant other (OR 3.17), not working (OR 2.26) and deteriorated ability to concentrate (OR 2.04).
CONCLUSION: There were different factors for being satisfied with life as a whole between men and women, indicating a need for a more gender-specific rehabilitation than is currently used. The impact that deteriorated ability to concentrate has on life satisfaction is an important finding that needs to be considered in the rehabilitation process of younger patients after stroke.
Key words: stroke; life satisfaction; young adult; adult; middle age; gender.
J Rehabil Med 2010; 42: 155–161
Correspondence address: Jenny Röding, Department of Health Science, Luleå University of Technology, SE-971 87 Luleå, Sweden. E-mail: jenny.roding@ltu.se
Submitted January 28, 2009; accepted October 22, 2009
INTRODUCTION
Quality of life (QoL) is a broad concept covering several aspects such as health, social life and well-being (1). Life satisfaction, on the other hand, is seen as a purely subjective aspect of how people perceive their lives (2). Since stroke survival has been enhanced, more interest is being directed to QoL and life satisfaction related research (3). However, there are few studies on QoL or life satisfaction among young individuals after stroke (3–6). QoL outcomes for young patients after stroke are of special interest, since stroke has an impact on many domains of the survivors’ lives (3, 7, 8) and the fact that they are at the peak of their professional and family years (4, 9). Young survivors may face a lifetime of disability, which is another important reason for studying QoL (6).
Smout et al. (3) showed a 20% decrease in QoL in 20–55-year-old individuals after stroke, and Neau et al. (5) reported a decrease of up to 30% in Qol in their study of 16–45-year-old individuals after stroke. Shin et al. (6) found a wide variation in younger stroke individuals’ perceptions of QoL, and suggested that medical decision-making should be tailored to individual preferences. In a study on perceived physical and cognitive function we found that younger individuals after stroke who are independent in their personal activities of daily life (P-ADL) require better knowledge about their abilities and limitations (10). In order to achieve this they need information directly aimed at physical functioning.
Several studies have used the Life Satisfaction instrument LiSat-9 (11–13) to rate life satisfaction. According to Fugl-Meyer & Bränholm (13) the aim of rehabilitation should be to “mobilize the resources of individuals with impairment(s) so that, by having realistic goals, they may achieve optimal life satisfaction”.
We wanted to use life satisfaction as a measure to investigate to what extent individuals have adapted to their situation in life after stroke.
The aim of the present study was to describe self-reported life satisfaction in a large cohort of younger persons with stroke, treated in hospital and registered in the Swedish National Quality Register for Stroke Care (Riks-Stroke) aged 18–55 years 1–2 years after a stroke. We also wanted to investigate whether there were differences between men and women and to explore medical and social factors associated with life satisfaction.
METHODS
Participants
The present study included all persons after stroke between the ages of 18–55 years at the onset of stroke from the last 6 months of 2001 and the whole of 2002. The participants were recruited from Riks-Stroke (the Swedish national quality register for stroke). At that time-point it was estimated that Riks-Stroke included approximately 90% (14 of all hospital-treated individuals after stroke in Sweden. All new, acute stroke events (ICD-10; I61, I63 and I64) apart from transitory ischaemic attacks (TIA) and subarachnoidal haemorrhages (ICD-10; G45 and I60) are included in the register.
In order to identify those who had died between onset and the current study, Riks-Stroke data were compared with national mortality data. The study was approved by the ethics committee of the Medical Faculty of Umeå University (Dnr 03-165).
Questionnaire
LiSat-9 (13) was used to rate perceived life satisfaction. The scale was incorporated in our questionnaire and its intention is to discover the participants’ self-reported levels of happiness (satisfaction with life as a whole) and 8 domain-specific life satisfaction items (ADL, Leisure, Vocational situation, Financial situation, Sexual life, Partnership relation, Family life and Contact with friends/acquaintances). For each item the participants were asked to report their actual level of satisfaction on a 6-grade ordinal scale (where 1 is equal to “very dissatisfied” and 6 is equal to “very satisfied”). Background factors taken from Riks-Stroke were also used. In addition we used questions that considered changes in social factors as well as physical and cognitive functions after stroke selected from the questionnaire, which in total consists of 97 questions. The construction of the questionnaire was based mainly on the results of a previous interview study of young people after stroke (15). Questions from valid and reliable instruments, such as LiSat-9 (29), parts of a Qol instrument for young haemorrhagic stroke individuals (HSQuale) by Hamedani et al. (16) and questions concerning P-ADL from the Bartel Index (17) were used. The questions from the different instruments were chosen in order to capture the same categories that emerged from the interviews (15).
All the questions were primarily intended to be answered by the participants themselves. If help was needed, this was noted in the questionnaire.
Enrolment
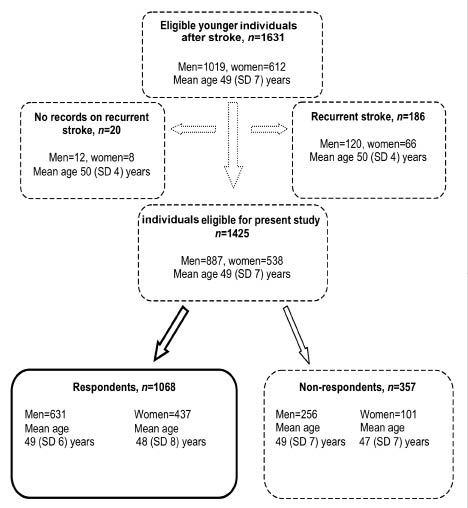
The questionnaire was sent to 1631 (1019 men and 612 women, mean age 49 years) eligible persons in October 2003. Of these, 186 had suffered a previous stroke and 20 persons had no record regarding recurrent stroke. Only those with a first ever stroke were included, and the study population therefore included 1425 participants. In January 2004, after 2 remainders had been sent out, 1068 (75%) people had returned the questionnaire (Fig. 1).
Fig. 1. Study population. Individuals collected from the Swedish national quality register for stroke, Riks-Stroke, during the last 6 months of 2001 and the whole of 2002 between the ages of 18 and 55 years. A total of 1068 individuals with a first stroke were included. The mean age and standard deviation (SD) are given.
Of the 25% (357 of 1425) non-responders, 298 were missing answers, 43 declined to participate and 16 addresses were missing. Out of the non-responders, more were men, diabetics, not fully conscious on admission at hospital, and more often diagnosed with haemorrhagic strokes. In addition, non-responders had been less frequently treated in a stroke unit.
Statistical analysis
The scores from LiSat-9 were dichotomized in order to separate those who were satisfied (grades 5–6) from those who were not satisfied (grades 1–4) (13). Multiple choice answers, selected from the 97-item questionnaire, as well as background factors from Riks-Stroke were also dichotomized. The aim was to separate those who were as good as before from those who had deteriorated. Differences between men and women as well as those satisfied and not satisfied with life as a whole were calculated using the χ² test.
In addition, multiple logistic regression was used to analyse several factors simultaneously. We assume that this study concerns a total population, but only at a certain time period, thus we have used the p-values as guidance for choosing predisposing factors. Hence, the multiple logistic regression model was based on significance values (p-value ≤ 0.05) from the χ² test of those satisfied and not satisfied with life as a whole. Men and women were analysed separately. “Not satisfied with life as a whole” was the dependent factor. For the men the independent factors were: P-ADL, living conditions, marital status, living with children, working situation, deteriorated ability to concentrate and run. Independent factors for the women were: diagnosis, P-ADL, treatment ward at hospital, working situation, deteriorated ability to concentrate and run. All statistical analyses were performed using SPSS version 15.0.
RESULTS
The questionnaires were completed by the participants themselves in 87% of cases. The response rate for the different questions was between 95% and 100%, with the exception of questions from the LiSat-9 regarding partnership/relation, sexual life and working situation, for which the response rate was 85%.
The majority, 79% (849 of 1068), of respondents were between 45 and 55 years. More than 1.5 years had passed between the onset of stroke and answering the questionnaire for 64% of the participants (681 of 1068). Eighty-five percent (872 of 1032) had suffered infarction. Eighty-two percent (813 of 990) had been treated in a stroke unit and 8% (80 of 1053) stated that they had been treated in a unit directly aimed at younger individuals. At the time of the questionnaire almost all of the participants, i.e. 97% (1018 of 1052), were living at home. Sixty-eight percent (717 of 1056) were living with a husband/wife/partner and 28% (294 of 1056) were living with children (Table I).
| Table I. Differences between men and women of the 1068 younger first ever stroke individuals. Total numbers of registered data and answers of the questions, numbers and proportion (%) of men and women, respectively, are given |
| | Men/total n (%) | Women/total n (%) | p-value* |
| Baseline data from the Riks-Stroke register |
| Age (n = 1068), years |
| 18–44 | 123/631 (20) | 96/437 (22) | |
| 45–55 | 508/631 (80) | 341/437 (78) | 0.325 |
| Atrial fibrillation at onset of stroke (n = 1054) |
| Yes | 21/626 (3) | 19/428 (4) | |
| No | 605/626 (97) | 409/428 (96) | 0.365 |
| Level of consciousness at onset of stroke (n = 1056) |
| Fully conscious | 49/624 (8) | 48/432 (11) | |
| Semi/unconscious | 575/624 (92) | 384/432 (89) | 0.071 |
| Hypertension therapy (n = 1055) |
| Yes | 177/625(28) | 114/430 (27) | |
| No | 448/625 (72) | 316/430 (73) | 0.518 |
| Previously known diabetes (n = 1065) |
| Yes | 92/628 (15) | 43/437 (10) | |
| No | 536/628 (85) | 394/437 (90) | 0.020 |
| Smoker (n = 944) | | | |
| Yes | 216/561 (39) | 177/383 (46) | |
| No | 345/561 (61) | 206/383 (54) | 0.041 |
| Treatment ward at hospital (n = 990) |
| Stroke unit | 494/588 (84) | 319/402 (79) | |
| Other | 94/588 (16) | 83/402 (21) | 0.060 |
| Diagnosis (n = 1032) |
| Infarction | 513/610 (84) | 359/422 (85) | |
| Haemorrhage | 91/610 (16) | 63/422 (15) | 0.671 |
| Time since stroke onset (n = 1068), years |
| < 1.5 | 224/631 (36) | 163/437 (37) | |
| ≥ 1.5 | 407/631(64) | 274/437 (63) | 0.547 |
| Self-reported data from the questionnaire |
| P-ADL status (n = 1039) |
| Independent | 524/614(85) | 343/425 (81) | |
| Dependent | 90/614 (15) | 82/425 (19) | 0.048 |
| Living condition at time of questionnaire (n = 1052) |
| At home | 604/624 (97) | 414/428 (97) | |
| Institutional living | 20/624 (3) | 14/428 (3) | 0.953 |
| Admitted to clinic specially aimed at younger (n = 1053) |
| Yes | 52/621 (8) | 569/621 (92) | |
| No | 569/621 (92) | 404/432 (98) | 0.254 |
| Marital status at time of questionnaire (n = 1056) |
| Husband/wife/partner | 417/625 (67) | 300/431 (70) | |
| Living alone | 208/625 (33) | 131/431 (30) | 0.324 |
| Living with children at time of questionnaire (n = 1056) |
| Yes | 170/625 (27) | 124/431 (29) | |
| No | 455/625 (73) | 307/431 (71) | 0.576 |
| Working situation at time of questionnaire (n = 1023) |
| Working | 358/603 (59) | 210/420 (50) | |
| Not working | 245/603 (41) | 210/420 (50) | 0.003 |
| Ability to concentrate compared with prior to stroke (n = 1043) |
| Unchanged | 281/617 (46) | 144/426 (34) | |
| Deteriorated | 336/617 (54) | 282/426 (66) | < 0.001 |
| Ability to run a shorter distance compared with prior to stroke (n = 937) |
| Unchanged | 154/566 (27) | 79/371 (21) | |
| Deteriorated | 412/566 (73) | 292/371 (78) | 0.041 |
| χ2 test. Bold figures indicate significance. P-ADL: personal activities of daily life. |
Women were to a higher degree smokers, P-ADL dependent, did not work at time of questionnaire and perceived a more deteriorated ability to concentrate as well as run a shorter distance now than before the stroke compared with the men. The men had more often been treated for diabetes before the stroke than the women (Table I).
Fifty-three percent of the young persons after stroke were not satisfied with life as a whole. There were 21% who were not satisfied with their P-ADL, 48% not satisfied with their leisure situation, 66% not satisfied with their vocational situation, 63% not satisfied with their financial situation, 68% not satisfied with their sexual life, 42% not satisfied with their partnership relation, 35% not satisfied with their family life, and 41% not satisfied with their contact with friends/acquaintances. The women were significantly less satisfied with their vocational and financial situation than the men (Table II).
| Table II. Self-reported values of life satisfaction according to LiSat-9 amongst 1068 younger individuals after stroke. Total numbers of answers, numbers and proportion (%) of men and women, respectively, are given |
| | Satisfied | Not satisfied | p-value |
| Men/total, n (%) | Women/total, n (%) | Men/total, n (%) | Women/total, n (%) |
| Life as a whole (n = 1020) | 292/609 (48) | 183/411 (45) | 317/609 (52) | 228/411 (56) | 0.283 |
| ADL (n = 1031) | 480/612 (78) | 330/419 (79) | 132/612 (22) | 89/419 (21) | 0.900 |
| Leisure (n = 1021) | 326/606 (54) | 202/415 (49) | 280/606 (46) | 213/415 (51) | 0.108 |
| Vocational situation (n = 955) | 213/537 (37) | 114/382 (30) | 360/537 (63) | 268/382 (70) | 0.019 |
| Financial situation (n = 1024) | 248/609 (41) | 135/415 (33) | 361/609 (59) | 280/415 (67) | 0.008 |
| Sexual life (n = 985) | 177/593 (30) | 134/392 (34) | 416/593(70) | 258/392 (66) | 0.152 |
| Partnership relation (n = 914) | 312/544 (57) | 221/370 (60) | 232/544 (43) | 149/370 (40) | 0.474 |
| Family life (n = 981) | 372/572 (65) | 265/409 (65) | 200/572 (35) | 144/409 (35) | 0.937 |
| Contact friends/ acquaintances (n = 1027) | 366/609 (60) | 239/418 (57) | 243/609 (40) | 179/418 (43) | 0.350 |
| Bold figures indicate significance. ADL: activities of daily life. |
Separate analyses of men and women showed that women who had had a haemorrhage diagnosis and were treated in a stroke unit were more likely to not be satisfied with life as a whole (Table III). Men who were living in an institution, with no significant other and without children living at home were more likely to not be satisfied with life as a whole (Table IV). For both women and men P-ADL dependency, not working, deteriorated ability to concentrate and to run a shorter distance were significant factors for not being satisfied with life as a whole (Tables III and IV).
| Table III. Association between self-reported satisfaction with life as a whole and background factors in 437 younger female individuals after stroke |
| | Satisfied/total n (%) | Not satisfied/total n (%) | p-value* |
| Baseline data from the Riks-Stroke register |
| Age (n = 411), years |
| 18–44 | 41/183 (22) | 52/228 (23) | 0.923 |
| 45–55 | 142/183 (78) | 176/228 (77) |
| Atrial fibrillation at onset of stroke (n = 402) |
| Yes | 5/177 (3) | 11/225 (5) | 0.293 |
| No | 172/177 (97) | 214/225 (95) |
| Level of consciousness at onset of stroke (n = 407) |
| Fully conscious | 161/181 (89) | 199/226 (88) | 0.778 |
| Semi/unconscious | 20/181 (11) | 27/226 (12) |
| Hypertension therapy (n = 404) |
| Yes | 51/181 (28) | 58/223 (26) | 0.625 |
| No | 130/181 (72) | 165/223 (74) |
| Previously known diabetes (n = 411) |
| Yes | 18/183 (10) | 24/228 (11) | 0.818 |
| No | 165/183 (90) | 204/228 (89) |
| Smoker (n = 359) |
| Yes | 75/160 (47) | 90/199 (45) | 0.755 |
| No | 85/160 (53) | 109/199 (55) |
| Treatment ward at hospital (n = 379) |
| Stroke unit | 126/170 (74) | 175/209 (84) | 0.021 |
| Other | 44/170 (26) | 34/109 (16) |
| Diagnosis (n = 396) |
| Infarction | 161/174 (93) | 176/222 (79) | < 0.001 |
| Haemorrhage | 13/174 (7) | 46/222 (21) |
| Time passed since stroke onset (n = 411), years |
| < 1.5 | 124/183 (68) | 135/228 (59) | 0.106 |
| ≥ 1.5 | 59/183 (32) | 93/228 (41) |
| Self-reported data from the questionnaire |
| P-ADL status (n = 400) |
| Independent | 158/177 (89) | 165/223 (74) | < 0.001 |
| Dependent | 19/177 (11) | 58/223 (26) |
| Living conditions at time of questionnaire (n = 403) | 0.423 |
| At home | 176/180 (98) | 215/223 (96) |
| Institutional living | 4/180 (2) | 8/223 (4) |
| Admitted to clinic specially aimed at younger patients (n = 406) |
| Yes | 12/183 (7) | 14/223 (6) | 0.909 |
| No | 171/183 (93) | 209/223 (94) |
| Marital status at time of questionnaire (n = 406) |
| Husband/wife/partner | 124/181 (69) | 158/225 (70) | 0.709 |
| Living alone | 57/181 (31) | 67/225 (30) |
| Living with children at time of questionnaire (n = 406) |
| Yes | 50/181 (28) | 69/225 (31) | 0.503 |
| No | 131/181 (72) | 156/225 (69) |
| Working situation at time of questionnaire (n = 397) |
| Working | 107/174 (62) | 92/223 (41) | < 0.001 |
| Not working | 67/174 (38) | 131/223 (59) |
| Ability to concentrate compared with prior to stroke (n = 402) |
| Unchanged | 78/176 (44) | 57/226 (25) | < 0.001 |
| Deteriorated | 98/176 (56) | 169/226 (75) |
| Ability to run a shorter distance compared with prior to stroke (n = 350) |
| Unchanged | 50/156 (32) | 25/194 (13) | < 0.001 |
| Deteriorated | 106/156 (68) | 169/194 (87) |
| χ2 test. Bold figures indicate significance. P-ADL: personal activities of daily life. |
| Table IV. Association between self-reported satisfaction with life as a whole and background factors in 631 younger male individuals after stroke |
| | Satisfied/total n (%) | Not satisfied total n (%) | p-value |
| Baseline data from the Riks-Stroke register |
| Age (n = 609), years |
| 18–44 | 63/292 (22) | 58/317 (18) | 0.311 |
| 45–55 | 229/292 (78) | 259/317 (82) |
| Atrial fibrillation at onset of stroke (n = 604) |
| Yes | 9/289 (3) | 12/315 (4) | 0.641 |
| No | 280/289 (97) | 303/315 (96) |
| Level of consciousness at onset of stroke (n = 602) |
| Fully conscious | 262/288 (91) | 291/314 (93) | 0.445 |
| Semi/unconscious | 26/288 (9) | 23/314 (7) |
| Hypertension therapy (n = 604) |
| Yes | 87/289 (30) | 89/315 (28) | 0.617 |
| No | 202/289 (70) | 226/315 (72) |
| Previously known diabetes (n = 606) |
| Yes | 36/290 (12) | 54/316 (17) | 0.106 |
| No | 254/290 (88) | 262/316 (83) |
| Smoker (n = 542) |
| Yes | 97/259 (38) | 112/283 (40) | 0.612 |
| No | 162/259 (62) | 171/283 (60) |
| Treatment ward at hospital (n = 566) |
| Stroke unit | 219/266 (82) | 254/300 (85) | 0.454 |
| Other | 47/266 (18) | 46/300 (15) |
| Diagnosis (n = 589) |
| Infarction | 235/278 (85) | 260/311 (84) | 0.758 |
| Haemorrhage | 43/278 (15) | 51/311 (16) |
| Time passed since stroke onset (n = 609), years |
| < 1.5 | 196/292 (67) | 196/317 (62) | 0.173 |
| ≥ 1.5 | 96/292 (33) | 121/317 (38) |
| Self-reported data from the questionnaire |
| P-ADL status (n = 595) |
| Independent | 268/288 (93) | 242/307 (79) | < 0.001 |
| Dependent | 20/288 (7) | 65/307 (22) |
| Living condition at time of questionnaire (n = 605) |
| At home | 289/291 (99) | 299/314 (95) | 0.002 |
| Institutional living | 2/291 (1) | 15/314 (5) |
| Admitted to clinic specially aimed at younger patients (n = 602) |
| Yes | 18/292 (6) | 31/310 (10) | 0.085 |
| No | 274/292 (94) | 279/310 (90) |
| Marital status at time of questionnaire (n = 606) |
| Living with husband/wife/partner | 235/292 (81) | 169/314 (54) | < 0.001 |
| Living alone | 57/292 (19) | 145/314 (46) |
| Living with children at time of questionnaire (n = 606) |
| Yes | 94/292 (32) | 71/314 (23) | 0.008 |
| No | 198/292 (67) | 243/314 (77) |
| Working situation at time of questionnaire (n = 586) |
| Working | 215/280 (77) | 135/306 (44) | < 0.001 |
| Not working | 65/280 (23) | 171/306 (56) |
| Ability to concentrate compared with prior to stroke (n = 598) |
| Unchanged | 167/287 (58) | 107/311 (34) | < 0.001 |
| Deteriorated | 120/287 (42) | 204/311 (66) |
| Ability to run a shorter distance compared with prior to stroke (n = 550) |
| Unchanged | 106/269(39) | 46/281 (16) | < 0.001 |
| Deteriorated | 163/269 (61) | 235/281 (84) |
| χ2 test. Bold figures indicate significance. P-ADL: personal activities of daily life. |
Multiple logistic regression, also analysing men and women separately, showed an association between not being satisfied with life as a whole and haemorrhage, as well as deteriorated ability to concentrate for women, and living without a significant other, not working and deteriorated ability to concentrate for men (Table V).
| Table V. Multiple logistic regression. Association between not being happy with life as a whole and significant background factors in the 1068 younger individuals after stroke. Men and women were analysed separately |
| Dependent | Independent | OR | 95% CI |
| Men |
| Not satisfied with life as a whole | P-ADL dependent | 1.687 | 0.874–3.255 |
| | Institutional living at time of questionnaire | 8.299 | 0.999–68.948 |
| | Living without husband/wife/partner | 3.173 | 2.047–4.919 |
| | Living without children | 1.168 | 0.755–1.809 |
| | Not working | 2.256 | 1.462–3.480 |
| | Deteriorated ability to concentrate | 2.038 | 1.332–3.119 |
| | Deteriorated ability to run | 1.442 | 0.884–2.354 |
| Women |
| Not satisfied with life as a whole | Haemorrhage | 3.999 | 1.680–9.520 |
| | P-ADL dependent | 1.788 | 0.812–3.896 |
| | Not treated in stroke unit | 0.548 | 0.290–1.036 |
| | Not working | 1.527 | 0.878–2.654 |
| | Deteriorated ability to concentrate | 2.111 | 1.201–3.709 |
| | Deteriorated ability to run | 1.753 | 0.919–3.347 |
| OR: odds ratio; CI: confidence interval. |
DISCUSSION
In this national coverage study of younger persons with stroke we found that more than half of the 1068 participants were not satisfied with life as a whole. The most important factor for not being satisfied with life as a whole for women was associated with haemorrhage, and for men living without a significant other.
Our results could be compared with another Swedish study of individuals after mild stroke, < 75 years, with a mild stroke, where 53% were not satisfied with life as a whole (12). In another study of younger Israeli individuals after stroke (mean age 57.7 years) similar results were found; 61% rated themselves not satisfied with life as a whole. However, the authors stress that the difference could be explained by cultural differences (18). These results can be compared with 2 studies on healthy Swedish persons (18–64 years) in which the LiSat-11 was used. They showed that 30% were not satisfied with life as a whole (19, 20).
The women in this study were less satisfied with their vocational and financial situation than the men. These differences are difficult to explain, as we have not found any other studies with similar results. In contrast, in our previous interview study on a limited number of subjects it was the men who expressed a need for security concerning their financial situation (15). At the same time, we cannot conclude that this has an impact on the life satisfaction. Neither can it explain why the women were less satisfied with their vocational and financial situation than the men in this study.
Reeves et al. (21) have, in their review, found that stroke-related outcomes, including disability and QoL, are poorer in women than men, although the reasons for this are not well understood. There is a need to study the underlying biological, epidemiological and clinical causes and manifestations of stroke in women. Our previous studies (10, 15) have shown differences between men and women in terms of both need (gender-related concerns about the rehabilitation process, the need to involve the family in the rehabilitation process, and financial issues) and deteriorated physical and cognitive functions. Hence, we decided to analyse men and women separately.
Both men and women who were P-ADL dependent, who did not work, had a deteriorated ability to concentrate and deteriorated ability to run, were more likely to be less satisfied with life as whole. The fact that P-ADL has an impact on life satisfaction has also been found in other studies (11, 12, 19, 20). However, to our knowledge no studies have investigated the consequences on life satisfaction of higher level of physical functioning; as, for example, ability to run in relatively restored persons who have had a stroke. This study shows that there is such an association, both for men and women. Presumably, P-ADL independence is not sufficient to measure life satisfaction in the younger stroke population since a higher level of physical functioning, here reported as sustained ability to run, had an influence on life satisfaction.
There were 2 independent factors for women associated with not being satisfied with life as a whole. The surprising result for the women in this study was the association between not being satisfied with life as a whole and having a haemorrhage. Two conclusions can be drawn from this. First, absence from obvious neurological deficits does not guarantee that the patient has made a complete recovery from the haemorrhage (25). Favourable outcomes for individuals after haemorrhagic stroke have been questioned, although, in spite of good motor recovery, they still exhibit cognitive and emotional disturbances (16, 25, 26). It is common that survivors of haemorrhagic stroke are left with subtle and invisible disabilities such as fatigue, cognitive difficulties, and/or one-sided weakness (27). These disabilities can in some ways be more problematic than the visible ones (7) and have an impact on life satisfaction (12, 27). Secondly, in our previous study (15) we found that, since the impairment was invisible and therefore not as legitimate as other impairments, participants felt a sense of not being understood and a fear of what other people would think (15). A previous study of young female survivors after haemorrhagic stroke has shown that disability must be visible for the women to feel that it is worth taking seriously. They also hide their disabilities in order to be socially accepted and, by doing so, allow others to continue believing that disability must be visible (7). The conclusion that can be taken from this study and translated into ours is that such behaviour must influence life satisfaction, regardless of stroke diagnosis. For example, Gray et al. (28) have shown that women after ischaemic stroke report a lower quality of life than men.
Men who were not living with a significant other or without children living at home were less likely to be satisfied with life as a whole. The fact that having a steady partnership makes it more likely, for both men and women, to have a high level of life satisfaction has been reported in other studies (22). It is also known that a good marriage/relationship has a positive impact on health for both men and women (23, 24). There were 2 more independent factors for men associated with not being satisfied with life as a whole; however, the strongest association was with not living with a significant other. Nagayoshi et al. (29) have, in their study on life satisfaction in Japanese outpatients with stroke, also found that males who were living alone were less likely to be satisfied than their female counterparts.
Another important finding in this study is that men who did not work had a 2.5 higher risk of not being satisfied with life as a whole then those who worked. This was not the case amongst the women. The need for men to be working is known from other studies. It can be assumed that the men perceive their work as more important than do women. It is possible that the women are more used to being at home and taking responsibility for the home compared with men. Thus the men perceive greater differences due to their new situation. Results from our previous interview study showed the need for men to be able to support themselves in order to be satisfied (15). An interesting question that can be raised from these results is the difference between men and women when rating what values are most important for their total life satisfaction, e.g. how much importance do women attach to their vocational and financial situation when rating their overall life satisfaction compared with the men?
For both men and women deteriorated ability to concentrate was a factor for not being satisfied with life as a whole. In a previous study we have shown that there is an association between not being able to concentrate and several physical limitations (10, 15). Since cognitive deficits have also been shown to be a reason for not returning to work (30, 31) we suggest that cognitive abilities need to be considered more carefully when rehabilitating the younger stroke population.
Methodological considerations
One limitation of this study was that the whole questionnaire was not tested for reliability and validity. However, most of the questions were from established and tested instruments, enhancing the trustworthiness. Although LiSat-9 has only been tested for validity and reliability for structured interviews it has been used as postal questionnaire concerning stroke and mild brain injury (11, 32).
Another issue to be considered was the large number of questions, especially in regard to the fact that many of the participants had concentration deficits. This could, of course have an impact on the results. However, the response rate was between 95% and 100% for the different questions, with the exception of questions from the LiSat-9 on partnership/relation, sexual life and working situation. The reason for this may be that the subjects did not consider these questions appropriate. As a whole, it could therefore be assumed that subjects did not perceive the questionnaire difficult to answer due to concentration limitations.
Both speech deficits and side of lesion may have an impact on life satisfaction, but our data and analyses did not indicate that these factors were of importance for further analysis.
In conclusion, the fact that more than half of the 1068 younger population after stroke, of whom a majority were P-ADL independent, were not satisfied with life as a whole 1–2 years after the stroke could be interpreted as meaning that all aspects of rehabilitation had not been covered, when rehabilitation is considered as the ability to achieve optimal life satisfaction despite impairment. The impact that a deteriorated ability to concentrate has on life satisfaction is an important finding that needs to be considered in the rehabilitation process of younger individuals after stroke. The need for sex-specific interventions (21) in order to improve post-stroke recovery cannot be neglected, and more studies, both clinical and outcome measures, are warranted to reduce disability after stroke.
ACKNOWLEDGEMENTS
We would like to thank The Swedish Stroke-Association and The Foundation for Stroke Research, Northern Sweden, Umeå University for financial support. We would also like to thank physical therapy student Sara Eriksson for help with the initial data interpretation and literature review.
REFERENCES