Chien-Hung Lai, MD1,2*, Walter Hong-Shong Chang, PhD1*, Wing P. Chan, MD3, Chih-Wei Peng, PT, PhD2, Li-Kuo Shen, RT, MS4, Jia-Jin J. Chen, PhD5 and Shih-Ching Chen, MD, PhD2
From the 1Department of Biomedical Engineering, Chung Yuan Christian University, Chung Li, 2Department of Physical Medicine and Rehabilitation, Taipei Medical University and Hospital, 3Department of Radiology, School of Medicine, Taipei Medical University, and Department of Radiology, Taipei Municipal Wan-Fang Hospital, 4Department of Radiology, Taipei Medical University Shuang Ho Hospital, Taipei, and 5Institute of Biomedical Engineering, National Cheng Kung University, Tainan, Taiwan. *The first two authors contributed equally to this paper and should be considered as first authors.
OBJECTIVE: To determine whether bone mineral density loss after spinal cord injury can be attenuated by an early intervention with functional electrical stimulation cycling exercises (FESCE) and to ascertain whether the effect persists after FESCE is discontinued.
DESIGN: A prospective study.
SUBJECTS: Twenty-four individuals with spinal cord injury, 26–52 days after spinal cord injury, were divided into FESCE or control groups.
METHODS: FESCE was applied in the initial 3 months and then suspended in the subsequent 3 months. Bone mineral density in the femoral neck and distal femur was measured using dual energy X-ray absorptiometry before training, immediately after the initial 3 months of training, and at the end of the subsequent 3 months.
RESULTS: The bone mineral density decrease rate in the distal femur in the FESCE group was significantly less than that in the control group during the initial 3 months. However, there was no significant difference in the subsequent 3 months.
CONCLUSION: FESCE in the early stages of spinal cord injury can partly attenuate bone mineral density loss in the distal femur. However, bone mineral density loss in the distal femur cannot be ameliorated completely by FESCE. In addition, the effect on the attenuation of bone loss in the distal femur faded once FESCE was discontinued.
Key words: bone mineral density; functional electrical stimulation cycling exercise; spinal cord injury.
J Rehabil Med 2010; 42: 150–154
Correspondence address: Shih-Ching Chen, Department of Physical Medicine and Rehabilitation, Taipei Medical University and Hospital, 252, Wu-Hsing Street, Taipei, Taiwan 110, ROC. E-mail: csc@tmu.edu.tw
Submitted May 12, 2009; accepted September 23, 2009
INTRODUCTION
Osteoporosis is a well-recognized complication in individuals with spinal cord injury (SCI), and bone loss is severe after injury. A decline in bone mineral density (BMD) can be detected in the paralysed limbs of individuals as early as 6 weeks after SCI (1). This BMD loss might be expected to reduce bone strength after SCI. The potential effect of bone loss is increased risk of fracture as a result of minor trauma, often during routine movements and activities (2). The estimated incidence of fracture after SCI is 1–34% (3), and complication rates are as high as 20–40% (4). Therefore, the prevention of osteoporosis and subsequent reduction in fractures due to bone pathology in individuals with SCI is an important issue.
In order to increase BMD or prevent bone loss in paralysed human limbs, the application of functional electrical stimulation cycling exercise (FESCE) is one of the strategies that involve active loading toward the extremities. The influence of FESCE on BMD in SCI individuals has been assessed in previous studies. The results showed site-specific BMD changes in the paralysed limbs after FESCE. Some reports suggested that FESCE has little or no effect on BMD of the lumbar spine, hip or proximal femur in individuals with chronic SCI (5, 6). In contrast, Mohr et al. (7) showed that FESCE could increase BMD of the proximal tibia (PT) in individuals with chronic SCI. Another study by Frotzler et al. (8) found an increase in BMD at the actively loaded distal femur (DF) in individuals undergoing FES cycling training. Our previous work (9) also showed that FESCE could increase BMD in the DF and PT of chronic SCI subjects.
Most previous studies assessed the effects of FESCE on BMD for chronic cases of SCI. However, most researchers have agreed that rapid BMD loss occurs within the first 6 months after injury (10, 11). In fact, bone mass is significantly reduced throughout the femur of SCI individuals in the first year, compared with able-bodied individuals (12, 13). Also, bone loss may be associated with higher fracture rates of the femur in SCI individuals than in ambulatory controls (14). Therefore, early intervention is necessary to treat osteoporosis and reduce fracture rates associated with SCI.
A recent review by Biering-Sørensen et al. (15) reported that some studies explored the effect of FES on individuals in the early stages of an SCI, but only one of those studies carried out cycling exercise in SCI individuals. The results showed a trend for reduced bone loss in the tibial shaft in the FESCE group (16). It is not known whether FESCE is effective at attenuating BMD loss in the femur when applied to individuals in the early stages of SCI. Therefore, the purpose of this study was to determine whether FESCE can prevent or attenuate BMD loss in the femoral neck (FN) and DF of individuals in the early stages of SCI. We also investigated the effects once FESCE was discontinued.
MATERIAL AND METHODS
Subjects
Twenty-four medically stable subjects with SCI were recruited for this study 26–52 days after their injuries. Twelve of the subjects (10 men and 2 women; mean age 28.9 (range 22–37) years) underwent FESCE programmes as a group. The other 12 age- and sex-matched subjects (10 men and 2 women; mean age 28.3 (range 20–38) years) acted as the control group (Table I). The inclusion criteria were: having a neurologically complete SCI motor lesion (American Spinal Cord Association (ASIA) impairment scale (17) grade A) between C5 and T10; having muscle responses to trial electrical stimulation; and never having undergone FES therapy. The exclusion criteria were: unhealed or recent bone fractures; the presence of a metal instrument in the lower extremity; poorly controlled autonomic dysreflexia; heterotopic ossification; severe spasticity; a range of lower limb mobility that limited safe cycling; a history of cardiovascular disease; a history of pulmonary disease; a recent history of psychological disease; a history of parathyroid or thyroid disease; and the use of bone-acting drugs, calcium, or vitamin D.
The potential risks and benefits of participation were explained to each individual, and the study was approved by the Institutional Review Board of our hospital.
| Table I. Characteristics of individuals with spinal cord injury in the functional electrical stimulation cycling exercise (FESCE) and control groups |
| Subject | FESCE group | Control group |
| Age, years | Days post- injury | Level of injury | Age, years | Days post- injury | Level of injury |
| 1 | 22 | 30 | T6 | 20 | 42 | C6 |
| 2 | 26 | 46 | C5 | 27 | 39 | T5 |
| 3 | 23 | 35 | C7 | 33 | 30 | C8 |
| 4 | 29 | 32 | T6 | 25 | 29 | T9 |
| 5 | 36 | 28 | T8 | 31 | 26 | T6 |
| 6 | 35 | 34 | T7 | 26 | 46 | C5 |
| 7 | 28 | 45 | C6 | 23 | 32 | T1 |
| 8 | 32 | 29 | T2 | 36 | 29 | T5 |
| 9 | 25 | 42 | C5 | 28 | 33 | T7 |
| 10 | 23 | 32 | T5 | 38 | 51 | C6 |
| 11 | 37 | 33 | T2 | 21 | 35 | C7 |
| 12 | 31 | 38 | C7 | 31 | 27 | T6 |
| Mean (SD) | 28.9 (5.3) | 35.3 (6.1) | | 28.2 (5.7) | 34.9 (8.0) | |
| SD: Standard deviation. |
FESCE programme
Based on a cycling ergometer from a local manufacturer (Tonic Fitness Technology Inc. Tainan, Taiwan), the FESCE system was further constructed and developed as described in our previous study (18).
A trial stimulation of the quadriceps and hamstrings was performed to confirm the presence of useful muscle contractions and the capacity for cycling without manual assistance. FES was performed using 5 × 7 cm surface electrodes. Stimulation parameters were as follows: pulse frequency, 20 Hz; pulse duration, 300 μsec. The stimulation intensities were controlled by a microprocessor modulating a 4-channel stimulator developed by Chen et al. (19). Electrical stimulation was applied sequentially to the bilateral quadriceps and hamstrings to achieve a rhythmic pedalling motion. Active electrodes, placed on the quadriceps, were at the midpoint between the anterior superior iliac spine and the patella. Active electrodes, placed on the hamstrings, were at the midpoint between the iliac tuberosity and popliteal fossa. Reference electrodes were placed 2 cm above the patella and 2 cm above the popliteal fossa on the quadriceps and hamstrings, respectively.
In the FESCE group, FES cycling programmes were conducted 3 times a week in the initial 3 months, and suspended for the subsequent 3 months. The individuals required an exercise protocol based on the muscle status of their lower limbs. Initially, the individual pedalled with minimal resistance load for as long as the individual could tolerate it. Then the cycling time was gradually increased up to 30 min.
BMD measurements
Dual-energy X-ray absorptiometry (DXA) (XR 36 WB, Norland, Wisconsin, USA) techniques were used to evaluate the BMD in the right FN and DF. DXA was used because of its high accuracy and precision for FN and DF (20). The BMD of FN was measured by standard methods (21). Because BMD in the DF is not a standard measurement site, we used a custom method to measure it. The BMD of the DF was determined using optional Norland XR-36 scanner research software and analyses. The region of interest (ROI) was set at the site between the femoral condyles and 2 cm above the knee joint space. The width of the ROI was set to 2.4 cm, and the length to 1.8 cm; finally, the scanning area was set to 2.4 cm × 1.8 cm. All the scans for a single individual used the same ROI dimensions and placement as the initial scan. In the FESCE group, the BMDs of FN and DF were measured at the beginning (first measurement), the end of the 3-month cycling programme (second measurement), and 3 months after discontinuing the cycling programme (third measurement). In the control group, the measurement of BMD was performed at the same time as that of the FESCE group.
The normalized BMDs were calculated using the following equations:
• Normalized BMD of the second measurement (%) = (BMD of second measurement/BMD of first measurement) × 100%.
• Normalized BMD of the third measurement (%) = (BMD of third measurement/BMD of first measurement) × 100%.
The BMD decrease rates in the initial 3-month period and in the subsequent 3-month period were calculated with the following equations:
• BMD decrease rate (%), first to second measurement = 100% – normalized BMD of the second measurement (%).
• BMD decrease rate (%), second to third measurement = normalized BMD of the second measurement (%) – normalized BMD of the third measurement (%).
Measurements from 15 able-bodied men served as reference values. The BMDs of the right FN and DF in able-bodied individuals were measured twice on separate days, with an interval of at least one week. The coefficients of variation for BMDs in the right FN and DF of the same individuals were 1.0%, and 1.1%, respectively.
Data analysis
The Wilcoxon signed-rank test was used to determine differences in the BMD at each site between the 2 measurements in the FESCE and control groups, respectively. The level of statistical significance was set to p < 0.05. The Mann-Whitney U test was used to determine differences between the 2 groups in age, time after injury, initial BMD measurement at each site, and the decrease in the BMD. Analyses were performed using SPSS, version 12 (SPSS Inc., Chicago, IL, USA). A p-value of < 0.05 was considered statistically significant.
RESULTS
The mean duration between injury and the first measurement was 35.3 days (SD 6.1) and 34.9 days (SD 8.0) in the FESCE and control groups, respectively. There were no statistically significant differences between the groups (Table I). Also, there were no significant differences in the BMDs of the FN and DF at the first measurement between the FESCE and control groups (Table II). Individuals in the FESCE group completed a mean of 80.3% of the scheduled training sessions, corresponding to a mean of 2.4 training sessions per week (SD 0.3).
| Table II. Bone mineral density (BMD) (mean (standard deviation)) values and normalized BMD at the first, second, and third measurements in the femoral neck (FN) and distal femur (DF) in the functional electrical stimulation cycling exercise (FESCE) and control groups |
| Site | Group | First measurement | Second measurement | Third measurement |
| Femoral neck | FESCE | 0.927 g/cm2 (0.189) | 0.884 g/cm2 (0.171)* | 0.842 g/cm2 (0.168)+ |
| | | 100% | 95.410% (0.612) | 90.869% (1.061) |
| | Control | 0.913 g/cm2 (0.097) | 0.867 g/cm2 (0.095)* | 0.825 g/cm2 (0.092)+ |
| | | 100% | 94.881% (0.459) | 90.251% (1.019) |
| Distal femur | FESCE | 1.003 g/cm2 (0.064) | 0.981 g/cm2 (0.063)* | 0.913 g/cm2 (0.058)+ |
| | | 100% | 97.776% (0.967) | 90.986% (0.845) |
| | Control | 1.003 g/cm2 (0.110) | 0.936 g/cm2 (0.103)* | 0.868 g/cm2 (0.097)+ |
| | | 100% | 93.349% (0.533) | 86.539% (0.971) |
| *p < 0.05 for difference between the first and second measurements. +p < 0.05 for difference between the second and third measurements. |
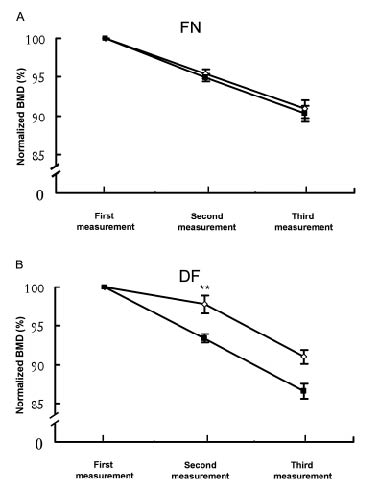
At the second measurement, the BMDs of the FN and DF were significantly lower than at the first measurement in both groups (p < 0.05) (Table II). In the initial 3-month period, the absolute BMD decrease in the FN did not differ between the groups. However, the decrease in absolute BMD values of DF in the FESCE group were significantly less than those in the control group (0.02 g/cm2 (SD 0.01) vs 0.07 g/cm2 (SD 0.01), p < 0.01). These BMD decrease rates are equivalent to 2.23% (SD 0.97) for the FESCE group and 6.65% (SD 0.90) for the control group. There was a significant difference in the BMD decrease rate in the DF between the FESCE and control groups (p < 0.01) (Fig. 1). The slope of the normalized BMD of FN in the FESCE group was similar to that in the control group (Fig. 1A), whereas the slope of the normalized BMD of DF in the FESCE group was less than that in the control group during the initial 3-month period (Fig. 1B).
Fig. 1. Normalized bone mineral density (BMD) at the first, second, and third measurements and the BMD decrease rate in the functional electrical stimulation cycling exercise (FESCE) and control groups. (A) No significant differences in the BMD decrease rate of femoral neck (FN) were observed between FESCE and control groups during the initial and the subsequent 3 months. (B) A significant difference in the BMD decrease rate of distal femur (DF) between groups was found only in the initial 3-month period (**p < 0.01). Empty diamonds: FESCE group # filled squares: control group.
At the third measurement, the BMDs of the FN and DF showed significant decreases from the second measurements in both groups (p < 0.05) (Table II). There were no significant differences in the absolute BMD decrease in the FN and DF between the FESCE group and the control group during the subsequent 3-month period. The slopes in the normalized BMDs were similar (Fig. 1).
DISCUSSION
To our knowledge, few researchers have studied whether FESCE programmes could lessen BMD loss of the femur in the early stages of SCI. The BMD in the FN and DF decreased significantly between the first and second measurements in the FESCE and control groups, with attenuation of the BMD reduction in the DF but not in the FN during the FESCE period. These results imply that there were site-specific changes from the FESCE programme, which partly reduced bone loss in the DF. Further studies are needed to determine whether a further decrease in bone loss could be obtained by a higher cycling resistance or more frequent training course than that used in our study.
The BMD decrease rate in the DF was lessened by the initial 3 months of FESCE, whereas no differences in the BMD decrease rate were found in the subsequent 3-month period in either group. This result implies that the effects of 3-month FESCE are insufficient for slowing down the BMD loss during a further 3 months without FESCE. These results are in contrast to the findings of Frotzler et al. (22), who showed that following 12 months of high-volume FES-cycling, BMD was preserved after 12 months of without training in individuals with chronic SCI. The reasons for this difference are unclear. It might be that Frotzler et al. and we recruited different test individuals and performed FESCE with different training protocols from those used in our study. However, this possibility remains to be confirmed.
It is well known that weight-bearing and forced stress due to muscle contraction play an important role in bone mineralization, and there is a marked decrease in BMD during periods of prolonged immobilization (23). Individuals with SCI usually have a rate of bone resorption that exceeds the rate of new bone deposition. This situation leads to a net loss in BMD and results in osteoporosis (11, 24). We observed that BMD declined by approximately 1.7% and 2.2% per month in the FN and DF, respectively, of SCI individuals in the control group. Our results are in accordance with the findings of Kiratli et al. (12), who showed that BMD was reduced by approximately 1.8% and 2.1% per month in the FN and DF, respectively, in the first year after SCI.
For several reasons, we chose to measure BMD of the FN and DF. First, the loss in bone mass is greater in the cancellous bone sites (FN and DF) than in the cortical midshaft during the first years (12). Secondly, measurements of the femur may have more significant results, as the stimulated muscles induce direct force stress on the femur (16). Thirdly, the femur is a common fracture site. Subjects with SCI have a 23.4-fold fracture rate compared with able-bodied individuals (14).
Why was the FN not similarly affected by FESCE? In our previous study (9), we showed that the FN is less affected by FESCE than the DF. Briefly, it is possible that the force load around the knee joint (DF) might be greater than the force load around the hip joint (FN) during quadriceps contraction, because among 4 components of the quadriceps femoris, only the rectus femoris crosses the hip joint at the proximal site, whereas all 4 components of the quadriceps cross the knee joint. Schultheis (25) demonstrated that mechanical stimulation through tension development at the muscle insertion point could increase BMD. Other studies also reported that the tension stress, owing to the contraction of the muscles and the movements of the joint, could increase local blood flow and augment the local status of bone formation (26, 27).
Electrical field or electromagnetic field stimulation itself has been applied with beneficial effect to the treatment of bone tissue in vitro and in vivo. Capacitively coupled electric fields and pulsed electromagnetic fields have been used in vitro to stimulate proliferation, differentiation, and/or matrix production in bone cell cultures (28, 29). Moreover, several animal experiments have reported that electrical stimulation can stimulate bone formation. The study by Hagiwara & Bell (30) showed that electrical stimulation promotes new bone formation in the early stages of mandibular distraction in rabbits. A SCI animal study by Lee et al. (31) also showed that electrically induced muscular contractions reduced BMD loss in 10 rabbits immediately after SCI. For individuals with SCI, FES therapy is non-invasive and well-tolerated. Hartkopp et al. (32) reported a fracture through the lateral femoral condyle of an osteoporotic and paraplegic individual caused by electrical stimulation. A safe protocol for FESCE should take into account minimizing the risk of fractures during FESCE. However, the application of FESCE to individuals in the early stages of SCI is relatively safe because the BMD is still above the fracture threshold for these subjects. In addition, the attenuation of BMD reduction in the DF in subjects undergoing FESCE in the early stages of SCI might have a clinical benefit because greater bone loss and common fracture sites are around the knee (33–35). However, for more clinical relevance, further investigations are needed to clarify whether a higher cycling resistance, a more frequent training course, and a longer duration of the total FESCE training period could have further benefit in attenuating the bone loss of individuals in the early stages of SCI.
In conclusion, intervention with FESCE in the early stages of SCI can partly attenuate BMD loss in the DF, but not in the FN. However, the BMD loss in the DF was not ameliorated completely during the period of FESCE. In addition, the effect on the attenuation of bone loss of DF faded once FESCE was discontinued. FESCE protocols should be further investigated to clarify the optimal effects of FESCE on BMD in the early stages of SCI.
ACKNOWLEDGEMENTS
The authors would like to thank all the subjects for participating in the study. We also thank Professor Hui-Wen Lin from the Biostatistical Center of the Taipei Medical University for the statistical analysis advice. This work was supported by the National Science Council, Taiwan, ROC, under grants NSC 89–2614-E-038–001 and 90–2614–E–038-001.
REFERENCES