OBJECTIVE: The aim of this study was to investigate differences in muscle stiffness between subjects with stiff shoulders and controls, and to determine the correlation between posterior shoulder muscle stiffness and range of motion of rotation.
DESIGN: Prospective, cross-sectional study.
SUBJECTS: Twenty subjects with stiff shoulder and 20 healthy subjects.
METHODS: Range of motion of rotation, and stiffness in 4 muscles (posterior deltoid, infraspinatus, teres minor and teres major), were measured in affected shoulders and control shoulders using a goniometer and a Myotonometer, respectively.
RESULTS: Patients with stiff shoulder had greater muscle stiffness than controls. Except for the teres major, significant correlations were found between internal rotation and stiffness of 3 muscles (r = 0.57–0.72). Among these 3 muscles, posterior deltoid muscle stiffness accounted for 51% of the variance in shoulder internal rotation beyond stiffness from the infraspinatus and teres minor muscles.
CONCLUSION: These findings support that muscle stiffness is related to shoulder range of motion. It is important to consider the posterior deltoid, infraspinatus, and teres minor muscles in the rehabilitation of patients with restricted internal rotation of the shoulder.
Key words: stiff shoulder; range of motion; muscle stiffness.
J Rehabil Med 2010; 42: 216–220
Correspondence address: Jiu-Jenq Lin, School and Graduate Institute of Physical Therapy, College of Medicine, National Taiwan University 3F, No. 17, Xu-Zhou Road, Taipei 100, Taiwan. E-mail: jiujlin@ntu.edu.tw
Submitted March 5, 2009; accepted November 4, 2009
INTRODUCTION
Stiff shoulder (SS), which is characterized by pain and functional restriction, is a common health problem (1–3). The prevalence of SS has been reported to be 2–10%, depending on the population of patients (4, 5). Reeves (2) subdivided SS into 2 types: “idiopathic frozen shoulder” and “post-traumatic stiff shoulder”. These subdivisions have distinctive historical and physical characteristics and are valuable in deciding a course of treatment. Frozen shoulder is defined as “an idiopathic contracture and loss of compliance of the glenohumeral joint capsule”. Post-traumatic stiff shoulder is defined as “a limitation in humeroscapular motion associated with soft tissue contracture after an injury”. Shoulder stiffness can affect individuals’ ability to function and, consequently, can decrease quality of life.
Various theories exist regarding the mechanisms of SS. Potential aetiological factors are: adhesive capsulitis (1), decreased capsular volume (6, 7), capsular contractions (8), rotator interval thickening and fibrosis (9), and subscapularis tendon thickening (9). Cyriax (10) proposed that stiffness in a shoulder joint capsule would restrict motion in a predictable pattern, a capsular pattern in which external rotation is more limited than abduction, which in turn is more limited than internal rotation. Other authors (11–13). have indicated that posterior shoulder stiffness, which is quantified by horizontal flexion range of motion (ROM) (cross-chest adduction), is significantly correlated with loss of humeral internal rotation ROM. Furthermore, several researchers (14–17) have hypothesized that the stiffness of specific muscles (e.g. rotator cuff) may contribute to posterior shoulder stiffness.
Clinically, it is important precisely to target the involved anatomical structure (muscle or capsule) that is the source of the joint restriction. Although mobilization and stretching are common treatments for improvement in shoulder stiffness (7, 18), they cannot selectively isolate restriction originating in the capsule or muscle(s). Several studies have concluded that the shoulder joint capsule plays a role in glenohumeral motion (1, 6–8). However, evidence to support the correlation of muscular problems with reduced shoulder ROM is limited. Based on a case report, Poser & Casonato (19) suggest that massaging the infraspinatus and teres minor muscles can result in 20 degrees of improvement in internal rotation. Therefore, we tested the muscular hypothesis related to ROM deficits in the shoulder. Our first hypothesis was that there would be a difference in muscle stiffness between subjects with SS and controls. Our second hypothesis was that there would be correlations between muscle stiffness and internal rotation deficit. The differences in the above relationships would exist among 4 muscles (posterior deltoid, infraspinatus, teres minor, and teres major).
MATERIAL AND METHODS
Subjects
Twenty patients with SS and 20 healthy subjects were recruited from a university hospital (Table I). Inclusion criteria for patients with shoulder problems were: (i) a limited ROM of internal rotation (internal rotation ROM < 20% to the sound side); and (ii) pain and stiffness in the shoulder region for at least 3 months. Exclusion criteria were: (i) surgery on the particular shoulder; (ii) rheumatoid arthritis; (iii) stroke with residual shoulder involvement; (iv) fracture of the shoulder complex; (v) rotator cuff deficiency; and (vi) resting pain, intolerable pain, or muscle spasm during active and/or passive motion.
| Table I. Subject demographics (stiff shoulders, n = 20, 9 men and 11 women; healthy controls, n = 20, 9 men and 11 women) |
| Variable | Stiff shoulders (n = 20) Mean (SD) | Healthy subjects (n = 20) Mean (SD) |
| Age, years | 57.9 (8.9) | 56.9 (7.4) |
| Internal rotation, ° | 30.4 (10.3) | 88.3 (4.6) |
| External rotation, ° | 56.2 (20.9) | 92.5 (6.8) |
| Duration of symptom, month | 14.8 (8.4) | |
| FLEX-SF score | 38.3 (5.3) | 50 |
| FLEX-SF: Flexilevel Scale of Shoulder Function. Scores were recorded from 1, with the most limited function, to 50, without any limited function in the subject. SD: standard deviation. |
Muscle stiffness measurement
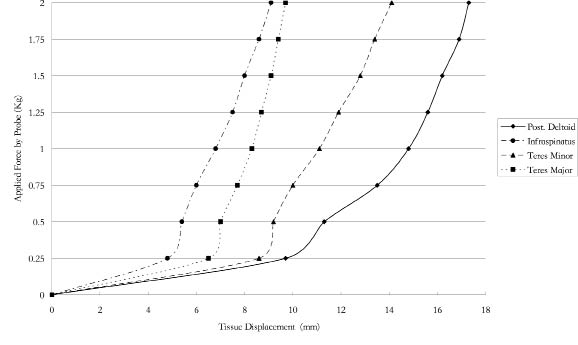
Muscle stiffness, defined as the change in passive tension per unit change in length, is an indication of a muscle’s passive resistance to elongation. In this study, we used a Myotonometer (Neurogenic Technologies, Inc., Montana, USA), a patented and computerized meter-type device, to measure relaxed muscle stiffness levels. The Myotonometer quantifies tissue stiffness by measuring the amount of resistance encountered when a probe is pushed downward onto the muscle and underlying tissue. The amount of tissue displacement (± 0.1 mm) caused by the pressure of the probe is recorded as related to the quantity of applied force. During the application of the probe, tissue displacement values are recorded at 8 force increments of probe pressure (0.25, 0.50, 0.75, 1.00, 1.25, 1.50, 1.75 and 2.00 kg). Force-displacement curves are generated from these data by computational software. Lesser penetration of the probe and a less sharp slope of the force-displacement curve indicate higher resistance (more stiffness). This use of the Myotonometer to measure muscle stiffness has been demonstrated to be valid and reliable (20–25).
Procedures
The involved shoulder and hand-matched control shoulder were tested, including measurements of ROM and muscle stiffness. First, ROM was assessed in a supine position for each subject. The subject’s arm was moved passively until the movement ceased (firm end-feel) of internal rotation with the arm held in 90 degree abduction by the tester. The recorder placed a handheld goniometer (Ever Prosperous Instrument, Inc., Taipei, Taiwan) with the 2 arms parallel to the forearm and trunk, respectively, and documented the ROM of rotation. During the test, the scapula was palpated at the lateral border and stabilized by hand. These measurements were aborted and restarted if the subject was unable to relax or if the scapula could not be stabilized effectively. Subjects did not report pain or discomfort during the test. Goniometry measurement of shoulder ROM has been demonstrated to be highly reliable in previous studies (intra-tester intra-class correlation coefficients (ICC) range: 0.80–0.93 from MacDermid et al. (26) and Riddle et al. (27)) as well as in our pilot study (ICC = 0.96).
Subsequently, the stiffness of the posterior shoulder muscles was assessed. Each subject was tested while seated in a chair, and the patient was told to expose the shoulder area to be tested. The subject’s arm was positioned on a pillow and the subject was asked to relax the shoulder (Fig. 1). The head of the Myotonometer probe was placed over the 4 posterior shoulder muscles in random order (posterior deltoid: 2 fingerbreadths caudad to the posterior margin of the acromion; infraspinatus: 2 fingerbreadths below the medial portion of the spine of the scapula; teres minor: one-third of the way between the acromion and the inferior angle of the scapula along the lateral border; and teres major: 3 fingerbreadths above the inferior angle of the scapula along the lateral border). Each muscle was tested in 3 trials (each trial included 4 measurements). Myotonometer data recordings of all 8 force increments took approximately 1 s. For each force increment, it took about 125 ms. The intra-rater/inter-rater reliabilities were acceptable at a 1.5–2.00 kg force level of measurement (ICC > 0.9). Therefore, the displacement at 1.50, 1.75, and 2.00 kg of each muscle was calculated for data analysis based on the mean of 3 trials.
Fig. 1. The probe used to measure muscle stiffness was applied perpendicularly to the surface of muscle, such as the infraspinatus.
Data analysis
Data were analysed using SPSS 12 software (SPSS Inc., Chicago, IL, USA). Independent t-tests were used to compare the soft tissue displacement (posterior muscle stiffness) at 1.50, 1.75 and 2.00 kg between subjects with SS and controls. Pearson correlation coefficients were calculated to identify the result of muscle stiffness measurements that correlated significantly with rotation. For explanatory rotation, stepwise regression models were calculated using significant measurements of muscle stiffness as predictors. Prior to Pearson correlation/stepwise regression modelling, the normality of the rotation deficit values was assessed using the Shapiro-Wilk test. If the Shapiro-Wilk test was significant (p < 0.05), the data were considered non-normal, and the dependent variable was transformed as appropriate to fit normality.
RESULTS
An example of force-displacement curves using Myotonometer measurements of muscle stiffness is presented in Fig. 2. The mean amount of tissue displacement by different forces among 4 muscles are presented in Table II. All values of measurement of muscle stiffness and shoulder rotation ROM passed the Shapiro-Wilk test (p > 0.05) and normality was assumed. Our results supported the first hypothesis. There were displacement differences at 1.50, 1.75 and 2.00 kg of posterior muscle stiffness between subjects with SS and controls (p < 0.05) (Table II).
Fig. 2. Force-displacement curves using Myotonometer measurements of muscle stiffness (one subject).
| Table II. Amounts of tissue displacement by different forces among 4 muscles |
| Muscle | Force, kg | Stiff shoulders (n = 20) | Healthy subjects (n = 20) |
| Displacement, mm Mean (SD) | Displacement, mm Mean (SD) |
| Posterior deltoid | 1.50 | 9.1 (3.9)* | 12.1 (1.8) |
| 1.75 | 10.6 (3.8)* | 13.6 (2.2) |
| 2.00 | 11.8 (3.5)* | 14.2 (2.5) |
| Infraspinatus | 1.50 | 5.7 (2.5)* | 7.7 (1.7) |
| 1.75 | 6.6 (2.6)* | 8.4 (1.8) |
| 2.00 | 7.4 (2.6)* | 9.7 (1.9) |
| Teres major | 1.50 | 7.8 (2.9)* | 11.2 (3.9) |
| 1.75 | 9.0 (2.9)* | 13.0 (1.4) |
| 2.00 | 10.0 (2.8)* | 14.5 (1.8) |
| Teres minor | 1.50 | 7.0 (3.2)* | 12.2 (2.2) |
| 1.75 | 8.0 (3.2)* | 13.1 (2.1) |
| 2.00 | 8.7 (3.0)* | 14.7 (1.8) |
| *There was a significant displacement difference between stiff shoulders and healthy controls. SD: standard deviation. |
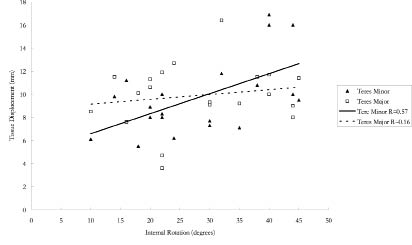
The second hypothesis was also supported. Significant correlations were found between measurements of muscle stiffness and shoulder internal rotation ROM in 3 of the 4 muscles measured; all but the teres major muscle (r = 0.57–0.72 for the posterior deltoid, infraspinatus, and teres minor, p < 0.05; r = 0.16–0.28 for the teres major, p > 0.05) (Table III and Fig. 3). Among the 3 muscles with significant correlations, the posterior deltoid and infraspinatus had higher correlations than the teres minor (r = 0.65–0.72 for the posterior deltoid and infraspinatus; r = 0.57–0.61 for the teres minor). However, there were no significant correlations between measurements of muscle stiffness and shoulder external rotation ROM (r = 0.11–0.38, p > 0.05). The stepwise regression model further indicated that approximately 51% of the variance in shoulder internal rotation could be attributed to posterior deltoid muscle stiffness (Table IV). On the other hand, the measurements of muscle stiffness of the infraspinatus and teres minor muscles were excluded from the stepwise regression model.
| Table III. Correlation coefficients for the association between muscle stiffness and internal rotation range of motion of the shoulder |
| | Force, kg | Internal rotation | External rotation |
| Posterior deltoid | 1.50 | 0.72** | 0.36 |
| | 1.75 | 0.71** | 0.37 |
| | 2.00 | 0.71** | 0.38 |
| Infraspinatus | 1.50 | 0.68** | 0.25 |
| | 1.75 | 0.66** | 0.26 |
| | 2.00 | 0.65** | 0.26 |
| Teres major | 1.50 | 0.28 | 0.11 |
| | 1.75 | 0.22 | 0.11 |
| | 2.00 | 0.16 | 0.12 |
| Teres minor | 1.50 | 0.61* | 0.31 |
| | 1.75 | 0.57* | 0.30 |
| | 2.00 | 0.57* | 0.32 |
| *p < 0.05, **p < 0.01. |
Fig. 3. Representative scatter plots for correlations between tissue displacement under 2 kg applied force and range of motion of internal rotation.
| Table IV. Stepwise regression results for shoulder internal rotation from muscle stiffness of the posterior deltoid, infraspinatus, and teres minor |
| Posterior deltoid | B (SE) | β | R-square |
| 1.50 kg | 1.93 (0.45) | 0.72* | 0.51 |
| 1.75 kg | 1.95 (0.45) | 0.71* | 0.51 |
| 2.00 kg | 2.12 (0.50) | 0.71* | 0.50 |
| *p < 0.05. The muscle stiffness measurements of the infraspinatus and teres minor muscles were excluded from the stepwise regression model. SE: standard error. |
DISCUSSION
Patients with restricted internal rotation of the shoulder had less displacement (more stiffness) of posterior muscles of the shoulder compared with controls. The result of the measurement of stiffness of the posterior muscles of the shoulder was also associated with reduced internal rotation of the shoulder. Although previous studies have proposed that the posterior muscles of the shoulder play a role in posterior stiffness of the shoulder (11, 17), they did not provide empirical data as evidence. The present study provides the data to support this relationship. Furthermore, the results indicate that stiffness of each muscle contributes differently to internal rotation of the shoulder.
To improve restricted internal rotation of the shoulder, the posterior deltoid, infraspinatus, and teres minor are most often targeted for treatment. In one case report, Poser & Casonato (19) demonstrated that massaging the infraspinatus and teres minor muscles can result in improvement in internal rotation. Massage was expected to increase muscle compliance, thus resulting in decreased passive stiffness (28). Hence, stiffness of the infraspinatus and teres minor can be regarded as factors in limitation of internal rotation of the shoulder. In accordance with their results, our data demonstrated that the results of measurements of stiffness of the infraspinatus and teres minor muscles correlated significantly with reduced internal rotation. Additionally, the posterior deltoid also showed significant correlations with reduced internal rotation in our study. Thus, relief of stiffness in these 3 muscles may result in improvement in internal rotation of the shoulder. From the anatomical point of view, the posterior deltoid, infraspinatus, and teres minor are external rotators of the shoulder, whereas the teres major is an internal rotator of the shoulder. Our data, which showed no significant correlation between the teres major and internal rotation, confirmed the anatomical and biomechanical roles of the teres major.
It is interesting to note that, from the stepwise regression model, stiffness in the posterior deltoid plays a major role in shoulder internal rotation among 3 muscles. Relief of posterior deltoid stiffness seems to be the major factor in improvement in shoulder internal rotation, accounting for approximately 50% of such improvement. This phenomenon could be explained by the functions of the posterior deltoid and infraspinatus/teres minor. The direction of the muscle fibres indicates that the posterior deltoid has an adduction component (29) in addition to an external rotation component, while the other 3 muscles provide only an external rotation component. In our study, the measurement of rotation ROM was conducted in the abduction position, which increases the tension of the posterior deltoid. Thus, stiffness of the posterior deltoid has a higher correlation with reduced internal rotation than does stiffness of the infraspinatus/teres minor. Additionally, we assume that if we could measure the stiffness in the abduction position without other possible confounding factors (other soft tissue tightness and the stretch reflex phenomenon), the correlation between internal rotation and posterior deltoid muscle stiffness would probably be higher. On the other hand, the other 50% of variance of restricted shoulder internal rotation may be caused by the posterior capsule or other muscles. Further research is required to test this assumption.
Limitations of the study should be noted. Myotonometer measurements can be compromised by the proximity of other soft tissue in addition to the target muscle. Because the 4 muscles are close to each other, the composition of soft tissues above the 4 muscles should be similar. The different values of the result of stiffness measurement between the 4 muscles in our study confirmed that the Myotonometer measurements focused on the stiffness characteristics of each target muscle. In our testing procedure, it was difficult to differentiate which tissue contributed to the feeling of firmness. To our knowledge, no studies have confirmed the assumption that the feeling of firmness stems only from the joint capsule. Although stiff shoulder is commonly regarded as a capsular problem, our results indicated that the muscle played an important role in restricted ROM. In addition to the 4 muscles tested, other muscles, such as the lassitimus dorsi/supraspinatus or the joint capsule, may contribute to internal rotation deficit. Although our results favoured the target muscles, the posterior deltoid as well as the infraspinatus/teres minor, the treatment effect should be tested in a clinical trial. Further studies should focus on other populations, and the treatment effects of muscle release techniques.
In conclusion, stiffness of the posterior shoulder muscles was correlated with reduced internal rotation. Stiffness of the posterior deltoid, infraspinatus, and teres minor muscles correlated significantly with reduced internal rotation. Of the 3 muscles tested, the posterior deltoid played the most important role in reduced internal rotation, accounting for approximately 50% of reduction in internal rotation. The other half of the variance in restricted shoulder internal rotation requires further study.
ACKNOWLEDGEMENTS
The authors wish to thank the participating subjects. Research funding was provided by the National Science Council (NSC 96-2628-B-002-035-MY3).
REFERENCES