OBJECTIVE: The aim of this study was to perform a systematic review of the effectiveness of comprehensive rehabilitation programmes for adults in the chronic phase after severe acquired brain injury.
METHODS: PubMed, PsychINFO and PsychLit were searched for articles published between 1990 and 2008 and a quality assessment was performed. The comprehensive programmes were subdivided into neurobehavioral interventions, residential community reintegration and day-treatment programmes. The extracted data included study characteristics, patient characteristics and intervention characteristics.
RESULTS: Thirteen studies met pre-established criteria. Two studies were randomized controlled trials, 5 were controlled comparative studies and 6 were uncontrolled longitudinal cohort studies. Overall, their methodological quality was limited. The investigated programmes led to substantial improvement in daily life functioning and community integration of severe chronic brain injury patients, with lasting effects at follow-up. Day-treatment programmes had the highest level of evidence.
CONCLUSION: Comprehensive rehabilitation programmes appear to be effective in terms of a reduction in psychosocial problems, a higher level of community integration and an increase in employment. Although this is the first review to differentiate between specific programmes, clear-cut clinical recommendations cannot yet be set out due to limited methodological quality and poor description of patient and intervention characteristics. Specific recommendations for future studies are given.
Key words: brain injury; rehabilitation; comprehensive rehabilitation; review; adult; middle-aged.
J Rehabil Med 2010; 42: 97–110
Correspondence address: Gert J. Geurtsen, Rehabilitation Centre Groot Klimmendaal, Department of Acquired Brain Injury, PO Box 9044, 6800 GG Arnhem, The Netherlands. E-mail: g.geurtsen@grootklimmendaal.nl
Submitted May 4, 2009; accepted October 27, 2009
INTRODUCTION
Severe acquired brain injury can have a tremendous impact on patients and family members. They must learn to live with a diminished potential for physical, emotional, cognitive, and social functioning (1). Many patients with severe acquired brain injury receive primary rehabilitation after hospital care. Carney et al. (2) consider “functioning as independently as possible in the patient’s own home and in society” to be the main goal of rehabilitation. To reach this goal, the rehabilitation process after brain injury needs to attain optimal community reintegration, including a good balance between social and vocational functioning, taking into account individual limitations (3). The ultimate goal is to gain a satisfying quality of life.
Apart from the direct consequences of injury, such as cognitive, emotional, behavioural problems and an impaired awareness of limitations (4), some patients develop secondary psychosocial problems later in life. These problems encompass anxiety, depression, and even alcohol and drug dependencies (5). These psychosocial problems in the chronic phase often hinder independent functioning and participation in society. The complexity and magnitude of these problems may require specialized comprehensive rehabilitation. Several comprehensive rehabilitation programmes addressing the long-term psychosocial consequences of brain injury have been developed (6). In their review, Malec & Basford (6) classified the comprehensive rehabilitation programmes for chronic sequelae of brain injury into: (i) neurobehavioral programmes: being “residential programmes that provide intensive behavioural treatment to brain injury patients with severe behavioural disturbances”; (ii) residential community reintegration programmes: providing “integrated cognitive, emotional, behavioural, physical, and vocational rehabilitation to patients who cannot participate in outpatient programmes because of either severe cognitive and behavioural impairments or the unavailability of outpatient services”; and (iii) holistic day-treatment programmes: offering “integrated, multimodal rehabilitation”, as defined and described by Ben-Yishay & Prigatano (7).
Cicerone et al. (8, 9) performed 2 literature reviews on the effects of cognitive and psychosocial rehabilitation, including research published up to 2002. They stated that “there is also evidence that gains in community functioning can be achieved by patients one or more years post-injury” and recommended comprehensive rehabilitation as a practice guideline for moderate to severe traumatic brain injury (TBI). However, they did not distinguish between the above-mentioned types of comprehensive treatment programmes, nor did they systematically address the impact of late rehabilitation.
Turner-Stokes (10) recently combined a Cochrane Review (previously published in 2005) with an approach using less rigorous design demands, yet excluding low-quality studies. She stated that: “although there is encouraging data from non-randomized clinical trials to support the benefits of behavioural management programmes, community rehabilitation and long-term intervention, this evidence is not yet sufficient to support strong recommendations”. This review contained only 4 studies concerning late rehabilitation, and the precise period for the inclusion of studies was not indicated. Moreover, the focus was primarily on the comparison of the 2 review approaches, whereas the specific patient characteristics and the content of the different comprehensive treatment programmes were not discussed.
Hence, little is known about the effectiveness of comprehensive treatment programmes for patients in the chronic phase after severe brain injury in view of their specific goals. Indeed, substantial differences between studies can be expected regarding the applied interventions within the various comprehensive programmes (i.e. neurobehavioural, residential community reintegration and holistic day-treatment), based on different patient characteristics. To our knowledge, no systematic review has yet been conducted to address these specific issues. The aim of this review was, therefore, systematically to address the following questions: (i) Are the different comprehensive treatment programmes for the management of long-term psychosocial problems in patients with severe acquired brain injury effective in terms of reducing these problems and improving community integration?; (ii) What are the specific patient characteristics for the various comprehensive treatment programmes?; and (iii) What are the essential intervention characteristics of these programmes?
METHODS
Selection of articles
A systematic literature search was performed in the primary electronic databases covering this research area: PubMed, PsychINFO and PsychLit, including articles published between 1990 and 2008. The year 1990 was chosen as a starting point because Turner-Stokes (10) and Cicerone et al. (8, 9) covered the period before 1990 and found no high-quality studies concerning comprehensive rehabilitation programmes for patients with chronic brain injury. A quick search performed by the authors of this review confirmed this finding. Details of the search strategies are shown in Appendix I. Grey literature was identified by additional hand-searching of the reference lists of the review articles on evidence-based cognitive rehabilitation (2, 8–11). Moreover, reference lists from the other identified articles were screened to complete the initial list of references. The first author performed the literature search as well as the primary selection of articles based on their abstracts. The primary selection of articles for this review was performed based on the criteria described in Table I. When selection was not possible based on the abstract alone, or when abstracts were not available, inclusion or exclusion was based on the full text versions.
| Table I. Inclusion criteria for the selection of publications |
| | Inclusion criteria |
| Participants | Non-progressive severe acquired brain injury (TBI, stroke, tumour, hypoxia, encephalitis) in the chronic phase (> 1 year) |
| Treatment programmes | Neurobehavioural programmes, residential community reintegration programmes or (holistic) day-treatment programmes |
| Type of study | RCT, comparative or uncontrolled longitudinal cohort studies |
| Publication type | Peer-reviewed journal articles |
| Year of publication | 1990–2008 |
| Language | English |
| Age | Adults (19–64 years) |
| RCT: randomized controlled trial; TBI: traumatic brain injury. |
Studies were included only when they addressed the effect of comprehensive treatment in a randomized controlled trial (RCT), a controlled comparative study or an uncontrolled longitudinal cohort study. Cross-sectional studies or reviews were excluded, because these study designs cannot assess treatment effects or deliver new (original) information on treatment effects, respectively. Furthermore, studies could be included when they addressed the chronic phase of severe acquired brain injury in adult patients, aged 19–64 years. For this specific purpose, “chronic” was operationalized as one year post-onset (6). The majority (> 50%) of the patients included in the study had to be in the chronic phase, or the results of the chronic patients had to be described separately.
Quality assessment
After the first selection, the methodological quality of the RCTs was assessed using the CONSORT Statement Checklist (12–16). The quality of potentially relevant articles with other study designs was judged using an adaptation of the Consort Statement, which was constructed in a consensus meeting with all authors. A set of minimal criteria for internal validity was established. Studies were definitively included when they fulfilled each of the following criteria: (i) the inclusion criteria were described; (ii) the content of the intervention was described at least globally; (iii) the number of patients was a minimum of 20 for uncontrolled cohort studies and at least 10 patients per treatment condition for controlled comparative studies or RCTs; (iv) effect sizes and statistical significance were reported; (v) at least one brain injury severity measure was described; and (vi) loss to follow-up was less than 20% (17).
Data extraction
When the methodological quality was considered sufficient, the first (GJG) and second (CvH) authors reviewed the articles separately and extracted the following data: (i) study characteristics (design, outcome domains/measures, duration of follow-up, and reported effects; (ii) patient characteristics (inclusion and exclusion criteria, number of participants, sex, age, aetiology, severity, time post-onset, baseline functioning); and (iii) intervention characteristics (content, duration, intensity, inpatient or outpatient treatment, rehabilitation team). Consensus was obtained in all instances and no discrepancies had to be settled by an independent third reviewer.
RESULTS
Selection and assessment of studies
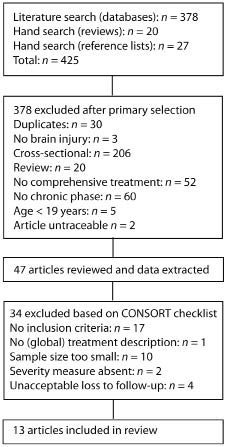
The primary literature search of databases, the hand search of the reference lists of review articles (2, 8–11), and the screening of the reference lists from all identified articles resulted in 425 potentially relevant studies. The primary selection based on title, abstract, and (when necessary) full text yielded 47 potentially relevant studies. These 47 studies were subjected to quality assessment, after which 13 studies were finally included for review (Fig. 1).
Fig. 1. Flowchart literature search
The characteristics of the design, patient population, and the treatment programme of the 13 selected studies are summarized in Tables II–IV. The studies can be categorized based on the applied treatment programme using the definitions set out by Malec & Basford (6): neurobehavioural programmes (n = 1), residential community reintegration programmes (n = 3), and day-treatment programmes (n = 9).
| Table II. Treatment programmes |
| Author, year (Ref) | Design/follow-up (FU) time | Outcome domains (measures) | Raw scores, % of change, significance | Reported effect* |
| Neurobehavioral treatment programmes |
| Wood et al., 1999 (30) | Uncontrolled retrospective study Selection: minimum treatment time 6 months pre + post + FU (minimum 12 months): FU mean 33 (range 12–61) months | Living arrangement Employment Care support Neurobehavioural problems Cost of care | Home/supported housing n = 33 rose to n = 51 post and n = 54 at FU, p = 0.0001 Pre employment/education 4%, post ?, FU 60.5%, p = 0.0001 Subdivided per time-since-injury p = 0.0001 No total pre-post-FU raw data reported. Subdivided per time-since-injury No total pre-post-FU raw data reported. Subdivided per time-since-injury | + compared with themselves + compared with themselves + compared with themselves + compared with themselves + compared with themselves |
| Residential community reintegration treatment programmes |
| Willer et al., 1999 (24) | Controlled study using individual systematic matching procedure Admission, discharge, 1 year FU. Control FU for 20 of 23 patients | HALS CIQ | E: Total pre 20.39, post 14.62, FU 15.62 C: Total pre 20.30, post 18.98, FU 19.20 p < 0.001 from pre-post, p > 0.05 post-FU Total CIQ group by trial interaction p < 0.001 | + +/– |
| Gray & Burnham, 2000 (28) | Uncontrolled cohort study: Admission, discharge. No FU | Level of care required at discharge for 305 of 349 patients (87.7%) RDRS for 305 of 349 patients (87.4%) FIM+FAM for 197 of 349 patients (56.4%) | 85.6% discharged to community locations; pre-post p < 0.001 Only significance reported: TBI pre-post p < 0.001 Motor pre-post p < 0.001 Cognitive pre-post p < 0.001 | + + + + |
| Geurtsen et al., 2008 (29) | Cohort study: Admission, discharge, FU 1 year. | CIQ CES-D EuroQol ERS Living arrangement Work | Pre 14.0, post 17.2, FU 16.8: pre-post p < 0.05, FU p > 0.05 Pre 20.1, post 12.7, FU 15.4: pre-post p < 0.05, FU p > 0.05 Pre 9.5, post 8.3, FU 8.4: pre-post p < 0.05, FU p > 0.05 Pre 2.3, post 3.2, FU 4.3: pre-post p > 0.05, FU p < 0.05 Independent living pre 41.6% rose to 75% post and 71% at FU Work pre 37.5% rose to 46% post and 58% at FU | +, maintained at FU +, maintained at FU +, maintained at FU 0 post, + at FU +, maintained at FU +, further increase at FU |
| Day-treatment programmes |
| Ruff & Nieman, 1990 (19) | RCT with 2 pre-treatment measurements and 1 post-treatment measurement No FU | KAS social obstreperousness KAS psychoticism KAS withdrawn/depression | E: pre 58.8 post 62.8; C pre 67.9 post 63.2; p > 0.10 E: pre 15.8 post 16.0; C pre 18.3 post 20.3; p > 0.10 E: pre 17.9 post 17.7; C pre 19.4 post 18.7; p > 0.10 | 0 0 0 |
| Christensen, 1992 (25) | Uncontrolled cohort study; pre-injury, pre-treatment, post-treatment, FU approximately 1 year | Work only Work (education + work-trial + gainful employment) | No raw data presented, % not in table, only in figure Pre-post p < 0.001; post-FU p > 0.1 Pre-post p < 0.001; post-FU p > 0.1 | + pre-post treatment, no change at FU |
| Rattok et al., 1992 (20) | Controlled trial with 3 treatment packages administered consecutively in same facility with same staff Pre-treatment, post-treatment measurements Randomization not specified, no blinding. No FU, only vocational outcome at 3 and 9 months | Neuropsychological measures Functional behavioural measures: competence in daily live Intra- and interpersonal functioning Vocational outcome at 3 and 9 months | 41 raw scores presented pre and post divided in near transfer (trained tasks) and far transfer (untrained tasks). Near: p varying from 0.001 to not significant in treatment × outcome ANOVA. Far: all not significant No raw data presented, only number of patients achieving significant improvement. E1-E3 p < 0.01, E1-E2 p not significant 4 raw scores presented pre and post; treatment × outcome ANOVA. All of them not significant Open environment: E1 70%, 52%; E2 78%, 78%; E3 83%, 61%. No p presented, no significant differences between treatments | + pre-post treatment, not much difference in treatment mix + pre-post treatment: E1 > E3, E2 seems > E3 + pre-post treatment, not much difference in treatment mix + pre-post treatment, no difference in treatment mix |
| Teasdale et al., 1993 (26) | Uncontrolled cohort study; Pre-injury, pre-treatment, post-treatment, FU approximately 1 year Comparison of TBI and stroke patients | Marital status Help in living situation Utilization of health services Work % working/education Work hours per week Leisure activities hours per week | Pre-injury 42%, pre 28% post 28%, FU 40% p = 0.06 Pre-injury 3%, pre 31% post 14%, FU 9% pre-post p < 0.05 Pre 2.4 post 0.7, FU 0.8, pre-post p < 0.05 Pre-injury 95%, pre 22% post 39%, FU 40% pre-post p < 0.05 Pre-injury 37.9, pre 9.2, post 15.8, FU 19.9 pre-post p < 0.05 Pre-injury 8.6, pre 5.4, post 5.1, FU 9.4 pre-post p > 0.05, pre-FU p < 0.05 | 0 pre-post treatment, 0 at FU. + pre-post treatment, 0 at FU. + pre-post treatment, 0 at FU. + pre-post treatment, 0 at FU. + pre-post treatment, 0 at FU. 0 pre-post treatment, + at FU. |
| Malec, 2001 (27) | Uncontrolled cohort study: Pre, post, FU 1 year | Work (VIS) unemployed Independent living (ILS) reaching individual goals (GAS) level of disability (PAI/MPAI) | Pre 84%, post 26%, FU 27% No p presented Pre 47%, post 69%, FU 72% No p presented Post 81% No p presented Pre 546.3, post 448.3; pre-post p < 0.0001 | + compared with themselves + compared with themselves + compared with themselves + compared with themselves |
| Cicerone et al., 2004 (21) | Uncontrolled comparative study; no randomization but allocation to treatment (with systematic bias in allocation): Pre, post No FU | Community Integration (CIQ) Satisfaction with community integration (QCIQ) Satisfaction with neuropsychological functioning (QCIQ) | ICRP Total pre 11.6, post 16.8 SRP Total pre 13.7, post 16.1 ANOVA p = 0.021 ICRP post 27.1, SRP post 29.7 p < 0.01 ICRP post 16.7, SRP post 18.2 p > 0.05 | + ICRP > SRP – SRP > ICRP 0 |
| Sarajuuri et al., 2005 (22) | Matched comparative study; no randomization but matching: Pre, FU 2 year | Productivity (working, studying, volunteer work) | E: 17 89%, C: 11 55% p = 0.017 | + E > C |
| Hashimoto et al., 2006 (23) | Comparative study; no randomization E + C. Pre + post. E treatment, C: convenience sample No FU Note: Selection or matching not specified | ADL (FIM/FAM) Societal participation (CIQ) | 17 FIM/FAM change scores in article comparison between both groups Total change E 3.52, C 0.58 p < 0.05 | + on speech, problem solving, memory, attention, social integration ( p < 0.05) 0 on rest ( p > 0.05) + on social, productivity and total score 0 on home score |
| Cicerone et al., 2008 (18) | RCT with pre-treatment, post-treatment and FU 6 months | Community Integration (CIQ) Perceived Quality of Life (PQoL) Neuropsychological functioning Perceived self-efficacy Vocational activity (VIS) | ICRP Total pre 11.2, post 12.9, FU 13.2 SRP Total pre 12.1, post 11.7, FU 12.9 ES = 0.59 ICRP pre 59.0, post 66.8, FU 66.1 SRP pre 61.2, post 62.2, FU 59.6 ES = 0.30 ICRP T-score pre 36.6, post 39.5 SRP T-score pre 35.9, post 39.5 ES = –0.20–0.09 ICRP Total pre 84.3, post 94.1, FU 92.4 SRP Total pre 82.6, post 84.8, FU 81.9 ES = 0.26 ICRP pre 3, post 16, FU 20 SRP pre 4, post 7, FU 14 | + ICRP > SRP + ICRP > SRP 0 SRP = ICRP + ICRP > SRP + ICRP > SRP |
| *Results are summarized as reported in the original studies. +: a positive difference in favour of the experimental group/compared with themselves; 0: no difference between the group/compared with themselves; –: a negative difference in adverse of the experimental group/compared with themselves; C: control; CDT: Comprehensive Day-treatment; CES-D: Centre for Epidemiological Studies-Depression; CIQ: Community Integration Questionnaire; E: experimental; ERS: Employability Rating Scale; ES: effect size; EuroQol: EuroQol group quality of life scale; FAM: Functional Assessment Measure; FIM: Functional Independence Measure; GAS: Goal Attainment Scaling; HALS: Modified Health and Activity Limitation Survey; ICRP: Intensive Cognitive Rehabilitation Programme; ILS: Independent Living Scale; KAS: Katz Adjustment Scale; MPAI: Mayo-Portland Adaptability Inventory; PAI: Portland Adaptability Inentory; PQoL: Perceived Quality of Life; QCIQ: Quality of Community Integration Questionnaire; RCT: randomized controlled trial; RDRS: Rappaport Disability Rating Scale; SRP: Standard Neurorehabilitation; VIS: Vocational Independence Scale. |
| Table III. Patient characteristics |
| Author, year (Ref) | Inclusion and exclusion criteria | Patients: n, M/F, age | Aetiology, time post-onset | Severity TBI: GCS, coma duration, PTA duration | Baseline functioning (at start of treatment) |
| Neurobehavioural treatment programmes |
| Wood et al., 1999 (30) | Unable to live independently and persisting history of aggressive behaviour. Criteria not specified. Minimum of 6 months of rehabilitation | n = 76, Drop-out 0 (0%) M/F: 57/19, Age: M: 38.0/F: 36.7 | TBI 58, stroke 12, anoxia 1, encephalitis 1, rest 4 Time post-onset 72.83 months (range 3–332) | PTA 23.5 days | Incapable of independent life in the community, dependent on others for their day to day social and domestic functioning. Neurobehavioural deficits on admission: aggression, disinhibition, mood disorders, impulsiveness, poor insight Cognitive: not described |
| Residential community reintegration treatment programmes |
| Willer et al., 1999 (24) | E: Severe brain injury, multiple disabilities and behavioural disabilities, often excluded from post-acute rehabilitation and referred to chronic care hospitals C: from the roster of a support group. | n =52 Drop-out 3 before treatment, 3 at FU: Total 6 (11.5%). M/F: E 20/3, C 20/3 Age: E 33.42 SD 11.31, C: 34.78 SD 10.72 | TBI Time post-onset 3.05 years | Coma > 72 h, most (18 of 23) > 3 weeks | E: Prior in acute care (1/23), inpatient rehabilitation (7/23), chronic care/psychiatric (7/23), own home/family (8/23), severe behavioural disabilities (not specified), not accepted by other regional programmes, HALS Total 20.39, CIQ Total 10.94. C: Lived with family (20/23), inpatient rehabilitation (2/23) or chronic care facility (1/23). HALS Total 20.30, CIQ Total 13.13 |
| Gray & Burnham, 2000 (28) | Severe brain injury, adult age, “slow to recover” with perceived potential to participate and benefit, but not appropriate for other community- or facility-based rehabilitation programmes | n = 349 Drop-out 0 (0%) M/F: 73.5%/26.6% Age: 39.4 | TBI 59%, Stroke 16%, SAH 9%, Anoxia 7%, rest 9%, missing 1% Mean 401.1 days | GCS 5.9 PTA in 89.6% > 7 days | RDRS 9.9, FIM+FAM motor score 67.5, FIM+FAM cognitive score 48.4. No description of behavioural or cognitive functioning. Almost 60% were referred from acute care facilities |
| Geurtsen et al., 2008 (29) | Brain injury and having severe problems in social areas, emotional areas, and labour/work integration Exclusion criteria: suitability for other (outpatient) cognitive rehabilitation programmes, severe disruptive behaviour, complete lack of problem awareness, severe memory problems, and severe drug addiction | n = 24 Drop-out 2 (8.3%) M/F: 75%/25% Age: 28.5 | TBI 18, Stroke 3, tumour 2, encephalitis 1 Time post-onset: 5.4 years | GCS 5.9 Coma duration 15.1 days (range 3–42 days) | Behaviour: 33% had alcohol and drug abuse problems. 41.6% was living independently, 21% were following education and 37.5% were working CIQ Total 14.0, CES-D 20.1, ERS 2.3 Cognitive: Many slow in processing information, some had attention deficits, some participants had executive problems. Severe memory problems were infrequent |
| Day-treatment programmes |
| Ruff & Nieman, 1990 (19) | Age between 16 and 65 years, moderate to severe head injury (coma at least one hour), chronicity between 1–7 years, no premorbid history of psychiatric disorders requiring hospitalization, sufficient cognitive functioning, sufficient expressive and recessive language skills, sufficient vision, at least one functional hand, motivation and availability to participate in 8-week programme and evaluations | n = 24 Drop-out 1 (4.2%, missing data) E: n = 12 M/F 9/3 Age 28.3 (range 18–48) C: n = 12 M/F 8/4 Age: 31.1 (range 18–47) | Acquired brain injury: aetiology not specified. Time post-onset: E 44.3 months (10–86) C 52.2 months (24–85) Not significantly different | E coma 25.5 days (range 0.5–47) C: coma 48.3 days (range 5–95) Significantly different | Behaviour and cognitive not described |
| Christensen, 1992 (25) | Brain injury, 16 years and older, good family and/or social support, return to employment or education should be feasible, 7 years of grade school, insight into own situation and/or motivation, partly preserved ability to communicate, ambulatory Exclusion: progressive central nervous system illness, significant history of substance abuse, psychiatric illness requiring treatment, chronic deteriorating illness | n = 46 Drop-out 0 (0%) M/F 28/18 Age: 30 SD 10.8 (range 16–58) | TBI 47.8%, CVA 30.4%, Hypoxia 15.2%, Rest 6.5% Time post-onset 2.9 years (range 0.5–14.2) Note 1: Same patients as in Christensen, Pinner et al 1992 Note 2: TBI and CVA seem to be reported in Teasdale (1993) too. | TBI: no coma 4.6%, coma < 1 day 18.2%, rest > 1 day | Hemi-paresis 28%, impairments of fine motor dexterity 24%, dysarthria 13%, ataxia 9% |
| Rattok et al., 1992 (20) | TBI with at least 1 hour coma or hypoxia with at least 12 h of coma, at least 1 year post-injury, unsuccessful prior vocational or educational rehabilitation, residence in greater New York metropolitan area during study, age between 18 and 55 years, functional English, at least partial independence in basic self-care, independence in ambulation, at least one functional hand, continence, minimal IQ of 80, motivation for rehabilitation, intact basic level of social appropriateness, manageable in non-coercive environment No past or present significant psychiatric complications, no history of significant alcohol or drug abuse, no history of sociopathy, no major aphasic or dysarthric difficulties | n = 59 Drop-out 0 (0%) E1: n = 23, M/F 15/8, Age: median 26.8 E2: n = 18, M/F 16/2, Age: median 27.1 E3: n = 18, M/F 11/7, Age: median 28.5 | Acquired brain injury: 56 TBI and 3 Hypoxia Time post-onset: E1: median 32 months E2: median 33.8 months E3: median 40.2 months | Coma: E1: median 34.3 days E2: median 38.9 days E3: median 36.9 days | E1: BCI 6.2, self-esteem 11.48, self-appraisal 6.35, interpersonal empathy 18.39, social cooperation 19.05 E2: BCI 6.7, self-esteem 13.28, self-appraisal 6.78, interpersonal empathy 19.72, social cooperation 19.17 E3: BCI 7.2, self-esteem 13.12, self-appraisal 6.47, interpersonal empathy 20.82, social cooperation 20.50 41 cognitive tests pre and post measurement All scores displayed but no description of meaning/explanation |
| Teasdale et al., 1993 (26) | Brain injury, age at least 16 years, good family and/or social support, subsequent education or employment considered realistic, at least 7 years grade school, insight into own situation, at least partial ability to communicate, ambulatory No progressive central nervous system illness, no significant history of substance abuse, no long-term psychiatric illness requiring treatment, no chronic deteriorating illness | n = 36 Drop-out 1 (2.8%) TBI: M/F: 73%/27% Age: 27.2 (SD 9.1). CVA M/F: 43%/57% Age: 36.4 (SD 12.1) | TBI n = 22 CVA n = 14 Note: Same patients seem to be reported in Christensen et al., 1992 Time post-onset: TBI: 3.1 years (SD 2.8) CVA: 2.6 years (SD 2.2) | TBI: no coma 4.5%, coma < 7 days 36.4%, rest > 7 days 59.1% | None were active in employment and more than one-third had experienced failed attempts to return to work. 31% receiving help pre-treatment. Further characteristics not specified |
| Malec, 2001 (27) | Brain injury, limited self-awareness, cognitive impairments, ineffectual communication and social skills, limited emotional and behavioural self-control. Independent in mobility, functional communication, sufficient memory for carry over of new information, no significant risk to selves or others Note: only 25% referred for treatment admitted | n = 113 Drop-out during treatment 17, loss to FU 1. Total 18 (16%) Remaining n = 96 M/F: 73%/27% Age: 34.2 | TBI 72%, CVA 19%, Rest 9% Time post-onset 4.6 years Note: probably partly same patients as Malec 1993. Malec 1993: Dec 1986–Aug 1991; Malec 2001: 1988–1998 | GCS: Mild TBI 7% Moderate 7% Severe 82% | 47% living independently, 84% unemployed, 6% sheltered work, 3% supported, 3% transitional and 4% independent work placement MPAI-22 score: 546.3, determined mean 102.4 days before treatment Behaviour and cognitive not described |
| Cicerone et al., 2004 (21) | ICRP: medical stable, independent self-care skills, cognitive able to participate in treatment, TBI, 18 years or older, adequate language expression and comprehension, family member or other participate in treatment plan Exclusion: current substance abuse or psychiatric disturbance SRP: inclusion and exclusion criteria not specified | n = 56 Drop-out 0 (0%) ICRP n = 27. SRP n = 29. M/F: ICRP 17/10 SRP 23/6 Age: ICRP 37.8, SRP 37.1 | All TBI Time post-onset: ICRP 33.9 months, SRP 4.8 months | Moderate to severe TBI 89% mild TBI 11% | ICRP: CIQ: Total 11.6, Home 3.1, Social 7.0, Productivity 1.4 Neuropsychological functioning: overall T score: 35.5. Behaviour not described SRP: CIQ: Total 16.7, Home 3.5, Social 6.8, Productivity 3.4. Behaviour and cognitive not described |
| Sarajuuri et al., 2005 (22) | E + C: Inclusion: independence daily life, only slight physical disabilities, age 16–55 years, completed compulsory education, adequate potential to achieve productivity Exclusion: significant psychiatric history, alcohol or drug abuse, previous brain injury, another malignant disease during follow-up Matching on: age, sex, education level, injury severity, time since injury, pre-injury employment | n = 42, drop-out 3 (7.1%). Remaining n = 39 described E: n = 19, M/F 16/3 Age at injury: 30.5 All TBI 42.4 months C: n = 20 M/F 17/3 Age at injury: 29.5 | All TBI Time post-onset: 46.6 months | E: GCS 7.9 C:GCS 8.0 | Both groups behaviour and cognitive not described E 6 (32%) failed in attempting to return to work/school. 1 productive part-time, 18 not productive C 6 (30%) failed in attempting to return to work/school |
| Hashimoto et al., 2006 (23) | E + C: Near independent in ADL, goal of returning to work or school, having no place to visit frequently except outpatient clinic | n = 37 Drop-out 0 (0%) E: n = 25, M/F: 18/7 Age: 26.6 (range 19–56) C n = 12, M/F not specified. Age: 28.7 | E: TBI 22, CVA 2, Tumour 1 Time post-onset 527.3 days C:10 of 12 severe TBI, rest? Time post-onset 487.6 days | E: 19 of 25 severe 5 moderate; 1 not clear | 3 used wheelchair and needed some help in ADL, FIM motor range 64–91, FIM Cognition range 17–34, FIM Total range 88–125 WAIS-R VIQ range 63–116, PIQ range 46–125. TIQ range 61–123 CIQ scores not mentioned Behaviour and cognitive not described |
| Cicerone et al., 2008 (18) | Inclusion for rehabilitation: medical stable, independent self-care, clinical judgement to benefit from comprehensive rehabilitation Inclusion for treatment study: TBI, at least 3 months post-injury, 18–62 years, adequate language expression and comprehension, require at least 4 months comprehensive treatment, clinical appropriate for both treatments, capable of attending treatment 3 days a week, be capable of giving informed consent Exclusion: active psychiatric illness, substance abuse or pain preventing compliance to treatment | n = 68 Drop-out 6 (8.8%) ICRP n = 34 SRP = 34. M/F: ICRP 25/9 SRP 21/13 Age: ICRP 38.7, SRP 34.5 | All TBI Time post-onset 43.3 months | Severe TBI 59% moderate TBI 24% mild TBI 13% undetermined 3% | 4% a previous TBI 13% history of psychiatric illness 21% history of substance abuse ICRP: CIQ: Total 11.2, Home 3.8, Social 6.4, Productivity 1.0 Neuropsychologic functioning: overall T score: 36.6. Behaviour not described SRP: CIQ: Total 12.1, Home 4.0, Social 7.3, Productivity 0.9. Neuropsychological functioning: overall T score: 35.9. Behaviour not described |
| ADL: activities of daily living; BCI: Behavioral Competence Index; BI: brain injury; C: control; CES-D: Centre for Epidemiological Studies-Depression; CIQ: Community Integration Questionnaire; CVA: cerebral vascular accident; E: experimental; ERS: Employability Rating Scale; FAM: Functional Assessment Measure; FIM: Functional Independence Measure; FU: follow-up; GCS: Glasgow Coma Scale; HALS: Modified Health and Activity Limitation Survey; ICRP: Intensive Cognitive Rehabilitation Programme; IQ: intelligence quotient; MPAI: Mayo-Portland Adaptability Inventory; PIQ: Performal IQ; PTA: post-traumatic amnesia; SAH: subarachnoid haemorrhage; SD: standard deviation; SRP: standard neurorehabilitation.TBI: traumatic brain injury; TIQ: total IQ; VIQ: verbal IQ; WAIS-R: Wechsler Adult Intelligence Scale-Revised. |
| Table IV. Intervention characteristics |
| Author, year (Ref) | Intervention | Treatment characteristics: duration/intensity | Treatment team | In- or out-patient |
| Neurobehavioural treatment programmes |
| Wood et al., 1999 (30) | Social and neurobehavioral rehabilitation directed at recovering behavioural and functional skills for semi-independent living in the community relying heavily on therapy care assistants | Duration mean 14.3 (range 6–32) months Intensity not specified | Relying heavily on therapy care assistants, rather than on professional therapy staff. Staff-patient ratio and treatment team not specified | Inpatient |
| Residential community reintegration treatment programmes |
| Willer et al., 1999 (24) | E: Structured social environment based on neurobehavioral model by trained and guided paraprofessionals; goal-directed rehabilitation: content not specified C: Home-based services provided by licensed professionals (in home or long-term care facility): content not specified | E: treatment by professionals (physician, OT, PT, ST) and trained paraprofessionals. Duration: 8 months C: variable range of home-based or outpatient services (support group, OT, PT, neuropsychological). Intensity variable. Duration: continuously even after 2–3 years Intensity not specified | E: staff-patient ratio not specified. Treatment team: professionals (physician, OT, PT, ST), neuropsychologist team coordinator and trained paraprofessionals C: none or OT, PT, neuropsychologist, case manager or home-maker service. Staff-patient ratio not specified | E: Inpatient C: Outpatient |
| Gray & Burnham, 2000 (28) | Comprehensive multidisciplinary rehabilitation in a hospital setting for slow-to-recover brain injury patients | Duration: mean 359 days Intensity not specified | Staff-patient ratio not specified Treatment team: medicine, psychiatry, nursing, PT, OT, dietetics, ST, psychology, neuropsychology, social work, recreation therapy | Inpatient |
| Geurtsen et al., 2008 (29) | Three modules (indepentent living, social-emotional, work). Training in safe therapeutic environment with continuous feedback on behaviour. Training skills. Increasingly applying learned skills in daily life at home. Relatives are actively involved and supported | Duration 198.9 days Intensity: 254 h therapy | Staff-patient ratio not specified Treatment team: neuropsychology, physiatry, neuropsychiatry, OT, cognitive therapy, social work, ST, PT, nurses | Inpatient |
| Day-treatment programmes |
| Ruff & Nieman, 1990 (19) | E: cognitive remediation: attention, visuospatial abilities, learning and memory, problem-solving C: day-treatment programme focussed on psychosocial functioning and activities of daily living | Duration: E and C: both 8 weeks 4 days a week Intensity: 36 h. E: daily 1 h group therapy, 3 h cognitive remediation and 20–30 min wrap-up session C: daily 1 h group therapy, 3 h psychosocial functioning and activities daily living and 20–30 min wrap-up session | Staff-patient ratio and treatment team not specified | Outpatient |
| Christensen, 1992 (25) | Group treatment 10–15 persons: Cognitive training, special education lessons, psychotherapy, voice therapy, workshops, physical training, lectures, relatives group | Duration/intensity: Phase 1: 4 months group treatment, 4 days a week for 6 h per day Phase 2: monthly group meeting. Furthermore coordination of gaining employment, education and disability pensions. Intensity not specified | Staff-patient ratio not specified. Treatment team: neuropsychologist, clinical psychologist, special education teacher, ST, voice therapist, PT | Outpatient |
| Rattok et al., 1992 (20) | All 3 treatment packages: Attention training 80 h, Community activities 60 h E1: Cognitive remediation 120 h, Small-group interpersonal exercises 100 h, Personal counselling 40 h E2: Cognitive remediation 0 h, Small-group interpersonal exercises 200 h, Personal counselling 60 h E3: Cognitive remediation 200 h, Small-group interpersonal exercises 0 h, Personal counselling 60 h | Duration /intensity: 400 h during 20 consecutive weeks 5 h per day 4 days per week Those judged by staff to be viable for work trials were assigned to vocational counsellor. Vocational trials ranged from 12 weeks to 6 months. Actual job search and placement was initiated by vocational counsellor. Patients were followed up indefinitely on work status and general adjustment. Some were placed immediately after remedial phase without work trials | One psychologist per 2 patients Staff-patient ratio not specified | Outpatient |
| Teasdale et al., 1993 (26) | Group treatment 10–12 patients: cognitive therapy, speech and language therapy and psychotherapy (individual and group), special education when required and physical exercise. Relatives group sessions twice a month | 4–5 months group treatment 4 days a week for 6 h per day. Followed by 6 months contact and meetings with emphasis on return to work or educational environment | Staff-patient ratio and treatment team not specified | Outpatient |
| Malec, 2001 (27) | Most group treatment according to model of Prigatano and Ben-Yishay and others. General goals: self-awareness, coping and compensation skills, personal organization, emotional and behavioural self-management, participation in work and leisure activities, health maintenance | Duration: Graduates: 189.5 days (27.07 weeks) Drop-outs: 43.4 days (6.2 weeks) Intensity not specified | Staff-patient ratio not specified. Treatment team: neuropsychologist, OT, OT-assistant, PT, recreational therapist, rehabilitation nurse, social worker, speech pathologist, vocational counsellor, physiatrist | Outpatient |
| Cicerone et al., 2004 (21) | ICRP: structured and integrated individual and group treatment; cognitive remediation, increasing awareness; interpersonal communication; psychotherapy; family support; work trials and placements SRP: primarily physical, occupational, speech and neuropsychological therapies determined to individual needs. Some recreational, educational, or psychological counselling when needed | Duration ICRP 3.8 months ICRP 4 days per week 5 h per day (typically 15 h therapy per week) + 1 day per week work trial. Intensity: approximately 248 therapy and 116 work h SRP: initially 15 h per week and adjusted varying from 12 to 24 h per week. Intensity not specified Duration SRP 3.9 months | ICRP Staff-patient ratio not specified. Treatment team: not described, vocational therapist supervises work trials SRP: Staff-patient ratio not specified. Treatment team: PT, OT, neuropsychological therapists, recreational therapist, vocational/educational therapist, psychological counsellor | Outpatient |
| Sarajuuri et al., 2005 (22) | E: Interdisciplinary neuropsychologic rehabilitation and psychotherapy based on Christensen, Prigatano, Ben-Yishay C: selection from patients seen for neuropsychological examination with previous conventional clinical care and rehabilitation (in- and outpatient) | 5 days per week 8.30–16.00 per day. Intensity not specified Duration 6 weeks. Afterwards neuropsychological follow-up support and coaching in work or education C: no active treatment | E: Staff-patient ratio not specified. Treatment team: 3 neuropsychologists, neurologist, rehabilitation nurse, social worker, 2 ST, OT, PT. Consultations by neuropsychiatrist, neuroradiologist and physiatrist C: no active treatment | E: Inpatient C: Previous inpatient/outpatient |
| Hashimoto et al., 2006 (23) | Group treatment: brain injury education, social skills training, positive behavioural support, redesigning subject’s environment | 4 groups with different duration/intensity varying from 4×4 h per week for 6 months to 2 h for 2 days per week for 3–4 months | Staff-patient ratio not specified. Treatment team: doctor, nurse, social worker, clinical psychologist, ST, vocational rehabilitation counsellor, OT, welfare facility life advisor, PT, rehabilitation gymnastic trainer | Outpatient |
| Cicerone et al., 2008 (18) | ICRP: integrating interventions for cognitive deficits, emotional difficulties, interpersonal behaviours and functional skills within a therapeutic community with performance feedback and active self-evaluation. Individual (4 h) and group (11 h) therapy SRP: individual interdisciplinary treatment, primarily discipline-specific interventions. Physical, occupational, and speech therapies. One hour neuropsychological treatment. Some patients psychological, recreational, vocational or educational. Individual (≥ 12 h) and group (≤ 3 h) therapy | ICRP + SRP Duration: 16 weeks Intensity: 15 h per week therapy = 240 h | ICRP: Staff-patient ratio not specified. Treatment team: not described, neuropsychologist SRP: Staff-patient ratio not specified. Treatment team: PT, OT, ST, neuropsychological therapist, recreational therapist, vocational/educational therapist, psychological counsellor | Outpatient |
| C: control; E: experimental; ICRP: intensive cognitive rehabilitation programme; OT: occupational therapy; PT: physical therapy; SRP: standard neurorehabilitation; ST: speech and language therapy. |
Study outcomes
The applied study designs, measurement instruments and observed treatment effects are described in Table II. Two studies were RCTs (18, 19) and 5 other studies were (non-randomized) controlled comparative studies (20–24). Two of these used matching (22, 24). The remaining 6 studies were uncontrolled longitudinal cohort studies. Study outcomes are discussed on the basis of study design and applied treatment programme.
Randomized controlled trials
Day-treatment programmes. In a RCT by Cicerone et al. (18) the experimental treatment was a comprehensive day-treatment group programme, emphasizing the integration of interventions directed at deficits, emotional difficulties and interpersonal behaviour with feedback from the group on the performance of the patient and active self-evaluation aimed at adaptation to chronic limitations. The control treatment was an interdisciplinary individual day-treatment programme targeting deficits including the retraining of cognitive functions. Both the experimental and control group comprised 34 patients. Treatment duration was 15 h per week for 16 weeks. Validated instruments (Community Integration Questionnaire (CIQ)) and the Perceived Quality of Life scale (PQoL)) were used as primary outcome measures and the follow-up period was 6 months. The experimental treatment had a moderate clinical effect on community functioning (assessed with the CIQ) and a small clinical effect on life satisfaction (assessed with the PQoL) compared with the control treatment. The experimental treatment showed significantly greater improvements than the control treatment and these gains were maintained at 6 months follow-up.
The RCT performed by Ruff & Nieman (19) also compared 2 day-treatment programmes. The experimental group received cognitive remediation and problem-solving training, whereas the control group received a programme aimed at enhancing psychosocial functioning and activities of daily living. Both the experimental and control groups comprised 12 patients who received treatment for 12 h per week during 8 weeks. A validated outcome instrument (Katz Adjustment Scale (KAS)) was used, but there was no follow-up. Both treatments appeared equally effective: patients became less socially withdrawn and depressed. Unfortunately, despite randomization, there were baseline differences for coma duration, with a shorter duration in the experimental group. This inequality at baseline was most likely due to the small number of patients. Another drawback of this study was the potential lack of contrast between the experimental and control treatment.
Residential community reintegration programmes. No RCT was identified.
Neurobehavioral programmes. No RCT was identified.
Controlled comparative studies
Day-treatment programmes. In the first comparative study, Rattock et al. (20) compared 3 day-treatment mixes. Their treatment programme was changed over the years and patients undergoing these separate mixes were compared. Differences in treatment were related to the availability and duration of cognitive remediation, the participation in small-group interpersonal exercises and the duration of personal counselling. The treatment groups comprised 18–23 patients. Patients received 400 h of treatment during 20 consecutive weeks. A combination of validated neuropsychological measures (such as the Wechsler Adult Intelligence Scale, Benton Visual Retention Test, etc.) and descriptive non-validated instruments was used. There was a follow-up only with regard to employability at 3 and 9 months. The description of absolute effect sizes was limited. All treatment mixes appeared effective on most neuropsychological measures, behavioural measures, and measures of productivity. However, there were only minor differences in efficacy between the treatment mixes.
In the second comparative study, Cicerone et al. (21) compared 56 patients with TBI who were allocated either to an experimental integrated comprehensive treatment or to a control treatment that was less intensive and less structured. There was a pre- and post-treatment measurement with a validated instrument (CIQ), but no follow-up. The experimental treatment seemed to result in a higher level of community integration, but allocation bias was a major confounding factor (21).
In the third comparative study, Sarajuuri et al. (22) offered day-treatment to 19 patients who were compared with patients with similar demographic and injury characteristics and who were seen for neuropsychological assessment only. The treatment duration was 7.5 h per day, 5 days per week for 6 weeks. After the training, the patients received neuropsychological support and coaching in work or education. There was no direct post-treatment measurement, only a follow-up measurement at 2 years. This study showed significant improvements in terms of productivity compared with the control group. Only descriptive instruments of work and education were used as outcome measures.
Hashimoto et al. (23) compared the effects of day-treatment with a control intervention in 25 and 12 patients, respectively. All patients were included from the same hospital and at the same time, but the selection procedure was not described. The treatment duration varied per group, from 4 to 16 h per week, for 3–6 months. The mean duration of treatment was 100 h. There were pre- and post-treatment measurements, but no follow-up. Furthermore, the control treatment was not specified. Despite this, the authors reported positive effects on the validated outcome measures (CIQ, Functional Indepence Measure + Functional Assessment Measure (FIM/FAM)) in the intervention group compared with the control group.
Residential community reintegration programmes. As for residential treatment, in the fifth comparative study by Willer et al. (24), 23 patients were compared with a matched sample of 23 patients receiving limited home-based services or outpatient treatment. The residential treatment offered a structured social environment based on neurobehavioural principles in which goal-directed interventions were offered; however, its content was not specified. The duration of the residential treatment was 8 months, but the intensity was not specified. The control group received a variety of home-based or outpatient services of variable intensity and duration. Validated outcome measures were the Modified Health and Activity Limitation Survey (HALS) and the CIQ. The study showed greater improvement in functional abilities and community integration in the group receiving the residential treatment. At one-year follow-up, the functional gains and the level of community integration were maintained.
Neurobehavioral programmes. No comparative study was identified.
Uncontrolled longitudinal cohort studies
Day-treatment programmes. Two original cohort studies have been conducted on the effects of day-treatment programmes (25, 27). Christensen (25) followed 46 patients and showed a significant increase in working hours after treatment, which was maintained at one-year follow-up. However, only descriptive non-validated instruments were used. Teasdale et al. (26) seemed to present the 36 patients with TBI and stroke of the Christensen (25) study with the same results.
Malec (27) followed 96 patients with validated (Portland Adaptability Inventory, Mayo-Portland Adaptability Inventory) and descriptive outcome measures. This study showed positive effects after treatment on employment, diminished care utilization, and independent living. These effects were maintained at one-year follow-up.
Residential community reintegration programmes. Two cohort studies were published that focused on the effectiveness of residential treatment (28, 29) in addition to the comparative study by Willer et al. (24). Gray et al. (28) conducted a historic cohort study using a database of 349 low-functioning patients who did not classify for regular rehabilitation. They used validated instruments (FIM/FAM, Rappaport Disability Rating Scale (RDRS)) and demographic data. They showed significant functional improvements of patients compared with other types of brain injury rehabilitation programmes.
Geurtsen et al. (29) performed a prospective cohort study of 24 patients with behavioural deficits leading to social, emotional, and vocational integration problems. They had a follow-up of one year and used a combination of validated (CIQ, Centre for Epidemiological Studies-Depression, EuroQol group quality of life scale) and descriptive outcome measures. This study showed significant improvements in various domains of community integration (living situation, work) at discharge and at one-year follow-up.
Neurobehavioural programmes. One cohort study was directed at the effects of a neurobehavioural treatment programme (30). The neurobehavioural intervention aimed to restore behavioural and functional skills for semi-independent living in the community. Descriptive measures for living arrangement, employment, and care utilization were used. The study had a variable follow-up period with a minimum of one year and a mean of 2.8 years, and showed a significant treatment effect in terms of improved living arrangements, hours of care required, and employment. These effects were maintained at follow-up (30).
Patient characteristics
The characteristics of the study populations are described in detail in Table III. The inclusion criteria were sufficiently described in 6 studies (18, 20, 25–27, 29). In the other 7 studies the inclusion criteria were only described globally (19, 21–24, 28, 30). Determining what treatment was directed at which type of patient was impossible due to the limited information provided about baseline cognitive or behavioural functioning. Only 2 studies gave a more extended description of functioning and problems before treatment (29, 30). All studies together included 982 patients, of whom 72.5% had sustained a TBI. Other diagnoses were stroke/subarachnoid haemorrhage (15.3%), anoxia (3.6%), other brain injuries (5.4%), and non-specified brain injuries (2.9%). The comprehensive treatment programmes were directed at severe and complex brain injury patients (Glasgow Coma Score 3–8, coma duration > 6 h or post-traumatic amnesia duration > 24 h; (31)). The exact numbers of mild, moderate or severe TBI patients were specified in a limited number of studies only (18, 21, 23, 27). The mean age of the patient groups varied from 26.6 to 39.4 years. Overall, 72.3% of the included patients were male, 26.5% were female, whereas 1.2% of the cases were unspecified in terms of gender.
Intervention characteristics
The characteristics of the interventions are described in detail in Table IV. In 6 studies the content of the intervention was described only globally (19, 23, 24, 26, 28, 30). The neurobehavioural intervention (30) was directed at restoring behavioural and functional skills for (semi-)independent living in the community for severely behaviourally disturbed patients. The residential community reintegration programmes had all been developed for specific purposes. One programme was directed at patients who were excluded from regular rehabilitation in the chronic phase (24). Another programme was aimed at low-functioning patients (28), and a third programme was directed at the reintegration of chronic patients with social, emotional and vocational integration problems due to behavioural disorders and/or substance abuse (29). Finally, the applied day-treatment programmes were group programmes directed at cognitive training, and improving self-awareness, coping and compensation skills using neuropsychotherapy (18–23, 25–27).
The duration of the applied treatments was often not exactly specified. The neurobehavioural programme lasted 14.3 months (30). The duration of the residential community reintegration programmes was from 28.4 weeks (29) to 51.3 weeks (28). The duration of the day-treatment programmes was the shortest, and varied between 6 weeks (22) and 27.1 weeks (27). The treatment intensity was specified in only 4 studies (18–20, 29). One comparative study specified the treatment intensity only for the experimental group (21). The hours of therapy varied from 36 to 400 in day-treatment (18–21) and 254 (29) in a residential treatment programme, whereas the other studies did not report on intensity.
The members of the rehabilitation team were described in only 10 studies (18, 20–24, 25, 27–29). The neurobehavioural intervention (30) relied on therapy care assistants. It was not specified who coached and trained these assistants. The residential community reintegration programmes were all multidisciplinary (24, 28, 29). The day-treatment programmes varied from therapy by psychologists alone (20) to multidisciplinary interventions (18, 22, 23, 25, 27). Cicerone et al. (18, 21) specified the therapists only for the control treatment. Some studies (19, 26) did not specify the therapists at all. The neurobehavioural programme and residential community reintegration programmes were all inpatient programmes, but Willer et al. (24) used an outpatient group as a control. The day-treatment programmes were given on an outpatient basis, but the patients in the study by Sarajuuri et al. (22) stayed in an inpatient setting during the treatment. Only the day-treatment interventions were described (22).
DISCUSSION
This systematic review of the effectiveness of comprehensive rehabilitation programmes for chronic patients with severe brain injury identified 13 relevant articles that fulfilled pre-established minimal criteria for internal validity. Seven studies used comparative designs, of which only 2 were RCTs. These RCTs (18, 19) were both directed at day-treatment programmes showing positive effects on daily life functioning and community integration. The effectiveness of the day-treatment was substantiated by 4 controlled, comparative studies (20, 21–23) and 3 uncontrolled longitudinal cohort studies (25–27). The positive effects after treatment were maintained in all 4 studies with a follow-up (18, 25–27). Residential treatment also led to changes in daily life functioning and social participation, but this was shown by only one comparative study (24). The effectiveness of residential treatment was substantiated by 2 cohort studies (28, 29) showing positive effects of these treatment programmes on daily life functioning, community integration and employment. The functional gains were maintained at one-year follow-up (24, 29). Only one study (30) investigated a neurobehavioural treatment programme showing improved functioning in several life areas (living accommodation, employment, hours of care needed) that was maintained at follow-up.
The first research question concerning the effectiveness of the comprehensive programmes for treating long-term psychosocial problems in patients with severe acquired brain injury cannot be answered adequately based on the current literature. Generally, it may be stated that daily life functioning and community integration can be enhanced by comprehensive programmes, with the highest level of evidence for the effectiveness of day-treatment programmes. However, for each of the 3 programme types, more qualitatively high-level research needs to be performed. Yet, in severely behaviourally disturbed patients, RCTs are difficult to perform because a control treatment may be unethical or unacceptable to caregivers. In these cases, cohort studies using a waiting period as a control condition may be an alternative to provide more evidence on the effectiveness of comprehensive programmes.
All treatment programmes included relatively young and predominantly male brain injury patients, most of whom had severe TBI, which is in accordance with TBI population rates. In general, the inclusion criteria for the treatment programmes were only marginally described: baseline cognitive and behavioural functioning were specified in only 2 studies (29, 30), while other patient characteristics were not described at all. As a consequence, it must be concluded that the specific patient characteristics for the different comprehensive treatment programmes are not known. In order to accumulate evidence in this field, researchers must elaborate carefully on the patient characteristics in future work. With this information we will be able to identify prognostic personal factors for positive outcomes. This, in turn, may contribute significantly to improvements in treatment efficiency.
There appeared to be a large heterogeneity in the intervention characteristics between different (types of) programmes. The neurobehavioural and residential treatments were inpatient programmes for subjects with severe behavioural difficulties and functional disabilities, respectively. Whereas the neurobehavioural programmes aimed to restructure psychosocial behaviour, the residential community reintegration interventions were directed specifically at improving functional abilities. The day-treatment programmes offered neuropsychotherapy in group programmes to patients in whom behavioural problems might be present, but only mild. The duration of treatment was different in the 3 types of programmes. The neurobehavioural programme lasted more than one year, the residential community reintegration programmes lasted between 6 months and one year, whereas the day-treatment programmes varied in length from 1.5 months to 6.2 months. These differences partly answer our third research question concerning the essential intervention characteristics of the various programmes. More specific characteristics cannot be given due to the limited description of the content, intensity and duration of the programmes.
The conclusions of this review are generally in agreement with those of Cicerone et al. (8, 9) and Turner-Stokes (10). The additional value of this review is, however, the clear distinction between types of comprehensive treatment programmes and the focus on patient and intervention characteristics. It underscores the necessity to provide more detailed information about these characteristics in future studies in order to be able to compare them adequately. Furthermore, compared with previous work (8–10), it integrates a larger number of studies concerning comprehensive rehabilitation in the chronic phase of severe acquired brain injury. However, the results of this review do not justify straightforward recommendations for clinical practice due to the limited methodological quality of the included studies and the heterogeneity of the interventions. The review does, however, reflect the present situation and clearly highlights the shortcomings and gaps in the present literature and knowledge of comprehensive treatment programmes for severe chronic brain injury.
Implications for future research
Given the present lack of high-quality studies, well-designed controlled studies (preferably RCTs) are necessary to further enhance the field of comprehensive treatment programmes for patients with severe acquired brain injury. Although performing an RCT in this area is notoriously difficult, this review shows that, at least in the field of day-treatment programmes, RCTs are possible. When treating patients with severe behavioural disorders in the chronic phase, other ways to control bias appear to be justified, such as using a waiting period before enrolment in the treatment arm. In all types of controlled studies, researchers are strongly encouraged to work according to the CONSORT Statement checklist, describing the general principles of a RCT (12–16) even when using a non-randomized design. In the same way as for pharmacological trials, the treatment characteristics should be described in detail, including dosage, duration and means of administration (32). The same is true for patient inclusion and exclusion criteria, in order to be able reliably to compare different studies. Editors and reviewers should be very strict in requiring that all studies provide this descriptive information.
Outcomes should always be presented as absolute scores and effect sizes with parameters of central tendency and variation. Effectiveness must be measured with responsive instruments validated in patients with brain injury in the chronic phase. For instance, the CIQ that was used in 5 of the 13 studies in this review is reliable and responsive (33) and is recommended to assess community integration objectively (34). And the World Health Organization Quality Of Life Assessment Abbreviated (35) is a well-validated and responsive instrument for brain injury patients (35). The Centre for Epidemiologic Studies-Depression Scale is a valid instrument to measure mood in this population (36) and the McMaster Family Assessment Device is a reliable and valid tool to measure family functioning (37). In addition, more individually tailored instruments, such as Goal Attainment Scaling, can be used (38).
When sound evidence of the effectiveness of different comprehensive treatment programmes is available, the next steps should entail the comparison of treatment mixes and testing differences in treatment duration and intensity to determine cost-effectiveness. Lastly, better theoretical underpinning of the interventions seems essential and possible using models from neuropsychology and cognitive psychology as well as knowledge from neurobiological research on severe brain injury, for instance about the impact of diffuse axonal injury (39) on the clinical course of cognitive impairments after severe brain injury. The hypotheses based on these models and neuroscientific information can then be tested to improve the results of comprehensive rehabilitation programmes (40).
ACKNOWLEDGEMENT
This study was funded by Johanna Child Fund and BIO Children Rehabilitation Fund.
REFERENCES