Jong Youb Lim, MD, Eun Kyoung Kang, MD, PhD and Nam-Jong Paik, MD, PhD
From the Department of Rehabilitation Medicine, Seoul National University College of Medicine, Seoul National
University Bundang Hospital, Seongnam, South Korea
Jong Youb Lim, MD, Eun Kyoung Kang, MD, PhD and Nam-Jong Paik, MD, PhD
From the Department of Rehabilitation Medicine, Seoul National University College of Medicine, Seoul National
University Bundang Hospital, Seongnam, South Korea
OBJECTIVE: To test whether multiple sessions of inhibitory low-frequency repetitive transcranial magnetic stimulation (rTMS) applied to the left parietal area can improve hemispatial neglect after stroke.
DESIGN: An open-label design.
Patients: Seven consecutive patients with hemispatial neglect after right hemispheric stroke were compared with 7 retrospectively recruited control patients.
METHODS: Seven patients received a session of 1 Hz rTMS to the left parietal area immediately prior to occupational therapy for 10 days. Seven control patients received only behavioural therapy.
RESULTS: Baseline values of the line bisection test and the Albert test were comparable in the two groups. The stimulation group showed a greater improvement in the line bisection test than did the control group. However, no differences were found between the two groups according to the Albert test.
CONCLUSION: In this pilot study, low-frequency rTMS application to the non-affected left parietal area was found to be safe and to improve line bisection test, which suggests that non-invasive cortical stimulation has a potential role as an adjuvant strategy during cognitive rehabilitation training in patients with hemispatial neglect. A prospective randomized, sham-controlled study is required to determine the beneficial role of non-invasive cortical stimulation on hemispatial neglect.
Key words: transcranial magnetic stimulation; hemispatial neglect; stroke; brain stimulation.
J Rehabil Med 2010; 42: 447–452
Correspondence address: Nam-Jong Paik, Department of Rehabilitation Medicine, Seoul National University College of Medicine, Seoul National University Bundang Hospital, 166 Gumi-ro, Bundang-gu, Seongnam-si, Gyeonggi-do, 463-707, South Korea. E-mail: njpaik@snu.ac.kr
Submitted June 23, 2009; accepted January 18, 2010
INTRODUCTION
Hemispatial neglect (HN) concerns an impaired ability to explore or react to stimuli presented at contra-lesional sides (1–3) and is generally regarded as a symptom of a right parietal lobe lesion (2). Approximately 40–81% of patients after stroke demonstrate HN, and this symptom is sustained in approximately one-third of these patients (3). Furthermore, HN interferes with the rehabilitative process and is associated with a poor functional outcome (4).
Visual scanning, central cueing, prism adaptation, sensory stimulation, and dopaminergic and noradrenergic drugs are all used to treat HN (3, 5). However, these treatments are inadequate in terms of inducing complete recovery in most stroke patients (2). Therefore, more effective interventions are required to facilitate recovery.
Repetitive transcranial magnetic stimulation (rTMS) has a potential role as a neurorehabilitative adjuvant strategy because it can modulate the excitability of targeted brain areas (6). Furthermore, it has been applied to improve motor (7–9) and language functions (10) in patients after stroke.
rTMS has also been used to improve HN (1, 11, 12), and it has been proposed that activities in contra-lesional homologous regions are increased due to a loss of active inter-hemispheric inhibition due to lesion-containing areas in stroke (6, 13). Nevertheless, it has been suggested in 2 case reports that reducing activity in the left healthy parietal lobe by applying inhibitory low-frequency rTMS can improve HN by reducing abnormally increased inter-hemispheric trans-callosal inhibition from the healthy to the lesioned cortex (11, 12).
In this pilot study, we tested the hypothesis that inhibitory low-frequency rTMS applied to the left parietal area in combination with behavioural therapy (BT) is feasible and can improve HN compared with a retrospectively recruited control group of patients after stroke treated with BT alone.
PATIENTS AND METHODS
Patients
Patients were consecutively recruited from an inpatient rehabilitation unit at our hospital, and the study protocol was approved by the local institutional review board. All study subjects or their legal representatives provided signed, written, informed consent.
The study population comprised 14 patients with HN due to unilateral right hemispheric stroke (mean 68.8 years (standard deviation; SD 11.4)); 7 patients who underwent rTMS combined with behavioural therapy (rTMS+BT) (mean 72.0 years (SD 5.3), and 7 control patients who underwent BT alone (mean 65.6 years (SD 15.2)).
The presence of HN was confirmed using the line bisection test (14), and patients were included if they scored a ≥ 15% deviation to the right from the centre (15). Patients with multiple brain lesions, unstable medical or neurological conditions, a foreign metallic body within the brain, a pacemaker, an artificial cochlear implant, severe depression, a history of seizure, and those unable to perform the outcome measure-related behavioural tasks were excluded.
The controls were recruited at the same inpatient rehabilitation unit and were diagnosed using the same criteria used in the rTMS+BT group. The control group was formed by including 7 consecutive patients, treated before the adoption of rTMS, who received normal care (BT) without rTMS (BT group, for more detail see below).
The clinical and demographic details of subjects are shown in Table I, and their imaging data are presented in Fig. 1.
| Table I. Clinical and demographic data of the subjects (n = 7) | ||||||||
| Patients | Sex | Age, years | Type of stroke (brain lesion) | Time after stroke, days | mRS | NIHSS | MMSE | |
| Intervention (rTMS + BT) | ||||||||
| 1 | M | 70 | Infarction (R MCA, BG) | 38 | 5 | 15 | 15 | |
| 2 | F | 76 | Infarction (R MCA) | 23 | 4 | 9 | 18 | |
| 3 | M | 70 | Haemorrhage (R fronto-parietal) | 17 | 4 | 9 | 25 | |
| 4 | F | 80 | Infarction (R thalamus) | 16 | 4 | 4 | 7 | |
| 5 | F | 72 | Haemorrhage (R parietal) | 9 | 5 | 1 | 21 | |
| 6 | F | 73 | Infarction (R MCA) | 17 | 4 | 13 | 15 | |
| 7 | F | 63 | Haemorrhage (R BG) | 313 | 4 | 9 | 16 | |
| Control (BT only) | ||||||||
| 1 | F | 48 | Infarction (R MCA) | 21 | 4 | 10 | 23 | |
| 2 | F | 53 | Haemorrhage (R thalamus) | 20 | 4 | 12 | 27 | |
| 3 | M | 81 | Infarction (R MCA) | 371 | 4 | 14 | 11 | |
| 4 | M | 50 | Haemorrhage (R thalamus, BG) | 15 | 4 | 9 | 24 | |
| 5 | F | 83 | Infarction (R MCA) | 23 | 4 | 13 | 24 | |
| 6 | F | 67 | Infarction (R MCA) | 470 | 5 | 16 | 7 | |
| 7 | F | 77 | Infarction (R parieto-occipital) | 53 | 4 | 13 | 12 | |
| mRS: modified Rankin scale; NIHSS: National Institute of Health Stroke Scale; MMSE: Mini-Mental Status Examination; rTMS: repetitive transcranial magnetic stimulation; BT: behavioural therapy; R: right; MCA: middle cerebral artery; BG: basal ganglia. | ||||||||
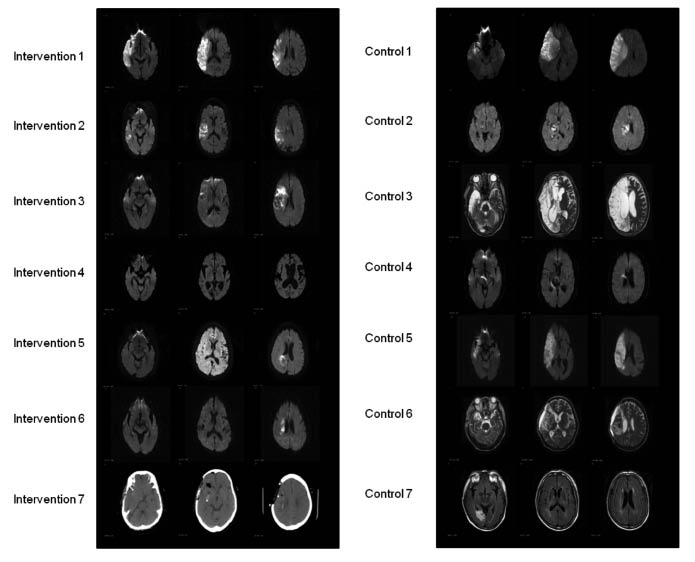
Fig. 1. Subject imaging data.
Experimental design
Members of the rTMS+BT group received rTMS over the left parietal area at a frequency of 1 Hz and a stimulus intensity of 90% of the resting motor threshold (rMT) using a MagPro® (Medtronic Inc., Minneapolis, MN, USA) for 15 min (900 pulses) immediately prior to 30 min of behavioural therapy. Intervention consisted of 10 daily sessions (5 days per week for 2 weeks). Improvements in HN were assessed using the line bisection test and the Albert test “pre”- and “post”-intervention. Evaluations were performed one day before and one day after intervention.
A figure-of-eight coil was placed tangentially over the P5 location as defined by the international 10/20 system (11). rMT was defined as the minimum stimulus intensity at which motor potentials from the resting right first dorsal interossei (FDI) muscle of larger than 50 µV were evoked during at least 5 of 10 consecutive trials.
BT consisted of a 30-min standardized neglect therapy protocol, which placed emphasis on the top-down approach and included, for example, visual scanning and feedback provision (16).
The control group received BT in exactly the same manner as the rTMS+BT group.
Outcome measures
The line bisection test (14) and the Albert test (17) were used to assess HN. The line bisection test was performed using Schenkenberg’s method (14). Briefly, 20 lines were drawn on A4 white paper parallel to its long axis, and 18 of these lines were organized into 3 sets of 6, such that these sets lay primarily on the left, at the centre, and on the right side of the paper. Each of these 3 set contained lines of length 100, 120, 140, 160, 180 and 200 mm. Two 150-mm lines were placed centrally at the top and bottom of the page. Subjects were asked to mark the centre points of the 18 lines in order. The examiner demonstrated the procedure initially by marking the 2 150 mm lines on the top and bottom of the page. Distances from the left of each line to subjects’ marks and to true line centres were measured. Deviations were measured using the formula:
A percentage deviation of 100% was recorded when a subject crossed the extreme right end of a line (the most severe form of left-sided HN), of 0% when a subject crossed the midpoint, and of –100% when a subject crossed the left end of a line (severe right-sided HN). Improvements after intervention were calculated by subtracting post-intervention values from pre-intervention values.
In the Albert test (17), 40 black lines, each 2.5 cm long were drawn on an A4 sheet of white paper. These lines were arranged in 2 sets of 3 columns of 6 lines/column separated by a central column containing 4 lines. The paper was placed in front of a patient, and the examiner demonstrated the procedure by checking the central column of 4 lines. The patient was then instructed to check all other lines on the paper. The numbers of lines checked in each column were recorded (left 12, centre 12 and right 12), and converted to percentages. Improvements after intervention were calculated and groups were compared.
Statistical analysis was performed using SPSS 17.0 (SPSS, Chicago, IL, USA, 2009). The non-parametric Mann-Whitney test was used to compare continuous variables and the χ2 test to compare nominal variables. p-values of < 0.05 were deemed significant, and all data are presented as means with SD.
RESULTS
Baseline characteristics, namely, age, sex, infarction/haemorrhage percentage, time after stroke onset, and modified Rankin scale (mRS), National Institute of Health Stroke Scale (NIHSS), and Mini-Mental Status Examination (MMSE) scores, were comparable in the rTMS+BT and BT groups (p > 0.05, Table II), as were baseline values of the line bisection test and the Albert test (p > 0.05, Table III).
| Table II. Subject baseline characteristics | |||
| rTMS+BT (n = 7) | BT (n = 7) | p-value | |
| Age, years, mean (SD) median (range) | 72.0 (5.3) 72 (63–80) | 65.6 (15.2) 67 (48–83) | 0.654 |
| Female, n (%) | 5 (71.4) | 5 (71.4) | 1.000 |
| Infarction, n (%) | 4 (57.1) | 5 (71.4) | 1.000 |
| Days after onset median (range) | 61.9 (111.1) 17 (9–313) | 139.0 (194.8) 23 (15–470) | 0.249 |
| mRS median (range) | 4.3 (0.5) 4 (4–5) | 4.1 (0.4) 4 (4–5) | 0.530 |
| NIHSS median (range) | 8.6 (4.8) 9 (1–15) | 12.4 (2.4) 13 (9–16) | 0.092 |
| MMSE median (range) | 16.7 (5.6) 16 (7–25) | 18.3 (8.1) 23 (7–27) | 0.701 |
| Age, days after onset, mRS, NIHSS, and MMSE were analysed using the Mann-Whitney test. Percentages of women and infarction rates in each group were compared using the χ2 test. mRS: modified Rankin scale; NIHSS: National Institute of Health Stroke Scale; MMSE: Mini-Mental Status Examination; rTMS: repetitive transcranial magnetic stimulation; BT: behavioural therapy. | |||
| Table III. Baseline data of the line bisection and the Albert tests | ||||||
| rTMS + BT (n = 7) | BT (n = 7) | p-value | ||||
| Mean (SD) | Median (range) | Mean (SD) | Median (range) | |||
| Line bisection test | Left | 93.8 (9.5) | 100 (75.5–100) | 92.8 (18.5) | 100 (51.0–100) | 0.602 |
| Centre | 69.9 (30.3) | 76.8 (26.7–100) | 74.6 (28.5) | 83.3 (18.7–100) | 0.798 | |
| Right | 19.2 (46.8) | 27.3 (–29.9–95.2) | 37.0 (32.2) | 35.5 (0.8–100) | 0.406 | |
| Albert test | Left | 29.8 (40.8) | 0 (0–100) | 9.5 (21.8) | 0 (0–58.3) | 0.413 |
| Centre | 56.0 (29.2) | 66.7 (0–83.3) | 21.4 (29.6) | 0 (0–75.0) | 0.076 | |
| Right | 92.9 (15.5) | 100 (58.3–100) | 60.7 (40.7) | 75 (0–100) | 0.076 | |
| Values were analysed using the Mann-Whitney test. rTMS: repetitive transcranial magnetic stimulation; BT: behavioural therapy; SD: standard deviation. | ||||||
All 7 patients in the rTMS+BT group completed the scheduled rTMS sessions without any adverse events.
According to the line bisection test, mean improvements in percentage deviation (= pre–post) of the left-sided line-set were greater in the rTMS+BT group than in the BT group (rTMS+BT group 33.4% (SD 27.5), median 28.5%, vs BT group 13.7% (SD 35.3), median 0.0%; p = 0.053), whereas those of the centred line-set (rTMS+BT group 39.1% (SD 51.0), median 21.4% vs BT group 29.9% (SD 34.1), median 15.7%; p > 0.05) and of the right-sided line-set (rTMS+BT group 14.1% (SD 58.9), median –0.9% vs BT group 19.4% (SD 43.6), median 10.3%; p > 0.05) were not (Fig. 2).
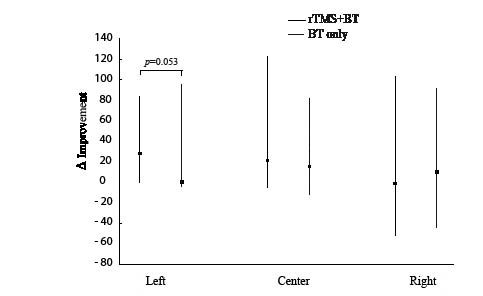
Fig. 2. Improvements in the line bisection test. Improvements in percentage deviations in the line-sets located on left-hand sides were greater for the “rTMS+BT group” (p = 0.053 by the Mann-Whitney test), whereas improvements in the percentage deviations in the line-sets located at centres and on right-hand sides were not (p > 0.05). Dots represent median values and bars represent ranges. rTMS: repetitive transcranial magnetic stimulation; BT: behavioural therapy.
Patients’ raw scores for the line bisection test are presented in Table IV. In the rTMS+BT group, 6 of 7 patients showed an improvement in percentage deviation for the left-sided line-set, whereas in the BT group, only 2 of 7 showed an improvement.
However, improvements in percentage deviation for the left-sided line-set in Fig. 2 were not found to correlate with patient ages, times after onset, or NIHSS scores (p > 0.05 by Pearson’s and Spearman’s correlation analysis).
| Table IV. Patient raw percentage deviation data obtained using the line bisection test | |||||||||||
| Patient number | Type of stroke (brain lesion) | Time after stroke (days) | Left | Centre | Right | ||||||
| Pre- | Post- | Improvement (pre-post) | Pre- | Post- | Improvement (pre–post) | Pre | Post | Improvement (pre–post) | |||
| Intervention | |||||||||||
| 1 | Infarction (R MCA, BG) | 38 | 100 | 59 | 41 | 100 | –23 | 123 | 50 | –30 | 80 |
| 2 | Infarction (R MCA) | 23 | 95 | 74 | 21 | 77 | 33 | 44 | 95 | –9 | 104 |
| 3 | Haemorrhage (R fronto-parietal) | 17 | 86 | 38 | 48 | 27 | 5 | 21 | –24 | –23 | –1 |
| 4 | Infarction (R thalamus) | 16 | 100 | 100 | 0 | 90 | 94 | –5 | 38 | 67 | –29 |
| 5 | Haemorrhage (R parietal) | 9 | 100 | 17 | 83 | 95 | 1 | 94 | 27 | 2 | 25 |
| 6 | Infarction (R MCA) | 17 | 100 | 72 | 28 | 72 | 76 | –4 | –23 | 29 | –51 |
| 7 | Haemorrhage (R BG) | 313 | 75 | 63 | 12 | 29 | 29 | 0 | –30 | 0 | –29 |
| Controls | |||||||||||
| 1 | Infarction (R MCA) | 21 | 100 | 91 | 9 | 93 | 48 | 44 | 30 | –2 | 32 |
| 2 | Haemorrhage (R thalamus) | 20 | 100 | 7 | 93 | 19 | 3 | 16 | 1 | 14 | –13 |
| 3 | Infarction (R MCA) | 371 | 100 | 100 | 0 | 83 | 80 | 4 | 35 | 25 | 10 |
| 4 | Haemorrhage (R thalamus, BG) | 15 | 99 | 100 | –1 | 80 | 15 | 65 | 8 | 0 | 8 |
| 5 | Infarction (R MCA) | 23 | 100 | 100 | 0 | 92 | 100 | –8 | 45 | 89 | –44 |
| 6 | Infarction (R MCA) | 470 | 100 | 100 | 0 | 100 | 93 | 7 | 100 | 47 | 53 |
| 7 | Infarction (R parieto-occipital) | 53 | 51 | 56 | –5 | 56 | –26 | 82 | 39 | –49 | 89 |
| R: right; MCA: middle cerebral artery; BG: basal ganglia. | |||||||||||
In terms of the Albert test, group improvements (mean improvements of percentage of the numbers of lines checked = post–pre) for the 2 left columns (rTMS+BT group 45.2% (SD 44.3), median 50.0% vs BT group 41.7% (SD 52.0), median 0.0%; p > 0.05) and centre columns (rTMS+BT group 29.8% (SD 30.8), median 33.3% vs BT group 36.9% (SD 37.2), median 25.0%; p > 0.05) were not significantly different. However, right-sided columns improved more in the BT group than in the rTMS+BT group (rTMS+BT group –8.3% (SD 19.8), median 0.0% vs BT group 28.6% (SD 34.3), 25.0%; p = 0.038) (Fig. 3).
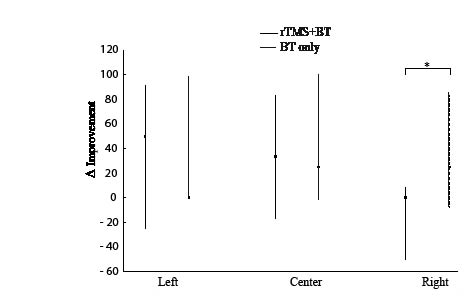
Fig. 3. Improvements in the Albert test. No significant inter-group improvement differences were observed for left-sided and centred columns. However, improvements in right-sided columns were observed in the “BT group” after treatment. *p < 0.05 by the Mann-Whitney test. Dots represent median values and bars represent ranges. rTMS: repetitive transcranial magnetic stimulation; BT: behavioural therapy.
Patients’ raw scores for the Albert test are presented in Table V. In the rTMS+BT group, 5 of 7 showed improvements in percentage of the numbers of lines checked for the left-sided line-set, where as in the BT group, 3 of 7 improved. However, neither improvements for the left-sided line-set nor for the right-sided line-set correlated with patient ages, times after onset, or NIHSS scores by Pearson’s and Spearman’s correlation analysis (p > 0.05).
| Table V. Patient raw data of percentage of the numbers of lines checked using the Albert test | |||||||||||
| Patient Number | Type of stroke (brain lesion) | Time after stroke (days) | Left | Centre | Right | ||||||
| Pre- | Post- | Improvement (post–pre) | Pre- | Post- | Improvement (post–pre) | Pre | Post | Improvement (post–pre) | |||
| Intervention | |||||||||||
| 1 | Infarction (R MCA, BG) | 38 | 0 | 92 | 92 | 0 | 83 | 83 | 92 | 100 | 8 |
| 2 | Infarction (R MCA) | 23 | 0 | 92 | 92 | 67 | 100 | 33 | 100 | 100 | 0 |
| 3 | Haemorrhage (R fronto-parietal) | 17 | 42 | 83 | 42 | 67 | 100 | 33 | 100 | 100 | 0 |
| 4 | Infarction (R thalamus) | 16 | 0 | 67 | 67 | 33 | 75 | 42 | 58 | 42 | –17 |
| 5 | Haemorrhage (R parietal) | 9 | 0 | 50 | 50 | 67 | 50 | –17 | 100 | 50 | –50 |
| 6 | Infarction (R MCA) | 17 | 100 | 100 | 0 | 75 | 100 | 25 | 100 | 100 | 0 |
| 7 | Haemorrhage (R BG) | 313 | 67 | 42 | –25 | 83 | 92 | 8 | 100 | 100 | 0 |
| Control | |||||||||||
| 1 | Infarction (R MCA) | 21 | 0 | 100 | 100 | 0 | 100 | 100 | 75 | 100 | 25 |
| 2 | Haemorrhage (R thalamus) | 20 | 0 | 100 | 100 | 75 | 100 | 25 | 100 | 100 | 0 |
| 3 | Infarction (R MCA) | 371 | 0 | 0 | 0 | 0 | 0 | 0 | 92 | 100 | 8 |
| 4 | Haemorrhage (R thalamus, BG) | 15 | 58 | 58 | 0 | 42 | 92 | 50 | 100 | 92 | –8 |
| 5 | Infarction (R MCA) | 23 | 0 | 0 | 0 | 0 | 0 | 0 | 25 | 50 | 25 |
| 6 | Infarction (R MCA) | 470 | 0 | 0 | 0 | 0 | 17 | 17 | 0 | 83 | 83 |
| 7 | Infarction (R parieto-occipital) | 53 | 8 | 100 | 92 | 33 | 100 | 67 | 33 | 100 | 67 |
| R: right; MCA: middle cerebral artery; BG: basal ganglia. | |||||||||||
DISCUSSION
The main finding of this comparative open-label pilot study was that rTMS applied over the left parietal area provides a safe and feasible means of treatment, and that rTMS before BT improved line bisection test results in patients with post-stroke HN compared with behavioural therapy alone.
HN is a common problem after stroke (5), and the results of uncontrolled trials suggest that rTMS is an effective therapy (1, 11, 12). The present study examined the effect of rTMS on HN using a retrospectively recruited control group.
HN is known to be a symptom of lesions in the parietal lobe (2). The supra-marginal gyrus of the right inferior parietal lobule is believed to be a critical involved area in cases of neglect, and therefore, right hemispheric lesions usually lead to more severe HN (2). However, right-side HN is also common after stroke (18), and it is likely that right-side HN is under-detected due to concomitant aphasia.
It has been proposed that the down-regulation of activity in healthy contra-lesional homologous areas could paradoxically facilitate motor (7–9) and language functions (10) after stroke, perhaps by reducing abnormally increased inter-hemispheric trans-callosal inhibition from the contra-lesional side to the ipsi-lesional cortex (19). Our results support the currently proposed mechanism of HN; that is, HN is caused by the relative hyperactivity of trans-callosal inhibition from the healthy hemisphere to the lesioned hemisphere (2). Previous neuroimaging studies have also demonstrated increased activation of the left healthy parietal lobe in HN (20).
| Percent deviation (%) = | Marked left side distance − True half length | × 100 |
| True half length |
In particular, we investigated the hypothesis that rTMS delivered over the left parietal area improves HN in patients after stroke. We found that the application of rTMS before behavioural therapy improved left-side HN in patients after stroke, which is consistent with the findings of previous case series (11, 12).
However, Oliveri et al. (1) reported that a single session of 25 Hz-facilitatory rTMS applied over the unaffected parietal area resulted in better improvement in ipsilateral HN than sham stimulation, which contradicts our hypothesis. Accordingly, the mechanism underlying the improvements induced by rTMS requires further study.
Furthermore, we found inconsistent associated changes between the line bisection test and the Albert test for neglect in the present study. One possible explanation for this dissociation is that different forms of HN respond in different ways to neglect tests (21). However, the present study does not have sufficient statistical strength to warrant a large-scale randomized controlled study. It has been demonstrated that tests vary in terms of their sensitivities to detect HN, and HN may be detected by one test, but not by another. Therefore, a patient with HN is usually operationally defined as one with a score below a certain cut-off value for the sum of a number of tests (22–24).
In the present study, the selection of right-sided columns was not improved in the rTMS+BT group based on Albert test results, whereas it was improved in the BT group. We postulate that this non-improvement in rTMS+BT was caused by a “ceiling effect” of the Albert test in this group. It is noteworthy that 6 of the 7 patients showed almost normal findings in right-sided columns.
According to individual patient analysis, patient 4 in the rTMS+BT group (female, 80 years old, 16 days after onset with a right thalamic infarction) did not show any improvement according to the line bisection test. We postulate that, in this patient, concomitant dementia, demonstrated by her MRI (which showed hydrocephalus), and a low MMSE score (7 points), caused rTMS to have a negative effect on HN. In the control group, patient 2 (female, 53 years old, 20 days after onset with a right thalamic haemorrhage) showed a marked improvement by the line bisection test, whereas the other 6 patients in this group did not. We suppose that spontaneous recovery occurred in this patient.
The present study has some limitations. The main limitation is that we did not randomize the patients, but rather adopted a retrospectively recruited control, which could have induced bias, because the examiner was not totally unaware of the type of intervention. Another limitation was that we did not apply sham rTMS stimulation to the BT group. The present study was a small, pilot study, and thus, the beneficial effect of rTMS on HN should be confirmed by a prospective, randomized, parallel group study, in which different patient groups receive different forms of stimulation (real rTMS or sham).
Furthermore, the recruitment of patients with the same aetiology, acuteness, and severity of HN would have been preferable. Days lapsed after onset tended to be longer and NIHSS to be poorer in the BT group, although this difference was not statistically significant, which does at least exclude the possibility that our positive result originated from a group difference in the acuteness or the severity of stroke. Furthermore, correlational analysis of the relations between HN improvements and times after onset and NIHSS scores failed to reveal any significant correlation.
It is likely that spontaneous recovery occurs after a subacute stroke. Our finding that HN did not improve among patients in the control group (patient 4 at 15 days after onset and patient 5 at 23 days after onset) during the subacute stage suggests that our positive intervention effect was not totally due to a group difference in lesion acuteness.
In future studies, greater emphasis should be placed on selecting patient populations to determine whether treatment response depends on age, lesion acuteness, or stroke severity. Similarly, it is important that the parameters which best optimize the beneficial effects of rTMS on HN be identified and that their long-term effects are determined.
In conclusion, this comparative open-label pilot study demonstrates that inhibitory low-frequency rTMS is a safe treatment modality, and that rTMS applied over the healthy left parietal area before BT improved line bisection test results compared with behavioural therapy alone. This finding suggests that rTMS has a potential role in terms of facilitating recovery from HN after stroke, and thus our findings support the merits of non-invasive cortical interventions as adjuvant strategies during cognitive rehabilitation training in patients with HN. Further research is required to determine the beneficial effects of rTMS on HN in the framework of a prospective, randomized, sham-controlled, parallel group design.
ACKNOWLEDGEMENTS
We thank our occupational therapy team for performing the hemispatial neglect assessments.
This research was supported by a grant from Seoul National University College of Medicine to Paik N-J (Grant No. 800-20060236)
REFERENCES
*Presented as a moderated E-poster at the International Stroke vConference held in San Diego, CA, USA on 18–20 February 2009.

