Andrea Santamato, MD1, Francesco Panza, MD, PhD2, Maurizio Ranieri, MD, PhD3, Maria Teresa Amoruso, MD1, Loredana Amoruso, MD1, Vincenza Frisardi, MD4, Vincenzo Solfrizzi, MD, PhD4 and Pietro Fiore, MD1
From the 1Department of Physical Medicine and Rehabilitation, University of Foggia, 2Geriatric Unit and Gerontology-Geriatrics Research Laboratory, Department of Medical Sciences, IRCCS Casa Sollievo della Sofferenza, San Giovanni Rotondo, Italy, 3Department of Neurological and Psychiatric Sciences, University of Bari and 4Department of Geriatrics, Center for Aging Brain, Memory Unit, University of Bari, Bari, Italy
OBJECTIVE: A few studies have reported the use of botulinum toxin injections after spinal cord injury, as this is the gold standard to treat focal spasticity. We report such a case here.
CASE REPORT: A 38-year-old woman who had become paraplegic and care-dependent secondary to cervico-thoracic intramedullary ependymoma, presented 8 months later with painful lower limb spasticity, which was being treated with oral anti-spastic and benzodiazepine drugs with no therapeutic effect. We treated the patient with intrathecal baclofen to reduce her spasticity and in order to avoid the major side-effects of high dosages of oral baclofen. After motor rehabilitation programmes, which included functional electrical stimulation, the patient was able to wear an advanced reciprocating gait orthosis. However, she experienced painful muscle spasms in her toes of the feet that limited her gait. Therefore, she was also treated with bilateral injections of botulinum toxin type A into the flexor digitorum brevis muscles. The patient reported relief of spasms and pain, enabling her to wear an advanced reciprocating gait orthosis and facilitating rehabilitation programmes.
CONCLUSION: The use of botulinum toxin type A may be an important adjunctive therapy to increase the therapeutic effect of baclofen on spasticity in small muscles, resulting in a more focal effect, and improving the use of orthoses and the effectiveness of rehabilitation programmes in patients after spinal cord injury.
Key words: botulinum toxin type A; intrathecal baclofen; spasticity; spasm; pain; advanced reciprocating gait orthosis; ARGO; spinal cord injury.
J Rehabil Med 2010; 42: 891–894
Correspondence address: Andrea Santamato, Department of Physical Medicine and Rehabilitation, University of Foggia, “OORR”, Viale Pinto, IT-71100 Foggia, Italy. E-mail: a.santamato@unifg.it
Submitted November 26, 2009; accepted June 9, 2010
INTRODUCTION
Spasticity and pain after spinal cord injury (SCI) are major problems that can limit the effectiveness of rehabilitation programmes (1). Severe spasticity is responsible for joint contractures, leading to poor bed posture and impaired motor function. Moreover, pain related to spasticity limits arm mobilization, and may result in the development of pressure sores. A typical clinical picture in complete thoracic SCI is spastic paraplegia and weakness of the lower extremities, the patient being unable to walk or to perform basic activities of daily living.
Current treatments in spasticity after SCI include oral or intrathecal baclofen together with motor rehabilitation programmes (2). However, the intrathecal route of administration is more effective to avoid the side-effects of high dosages of oral drugs, which include hypotonia, nausea, vomiting and lethargy. In fact, intrathecal treatment allows the dosage of baclofen to be reduced to only 1% of the oral dosage, because intrathecal administration results in a more than four-fold increased concentration of the drug in the cerebral spinal fluid compared with oral administration.
A few studies have reported the use of botulinum toxin injections to reduce spasticity after SCI (3, 4). Botulinum toxin is considered the gold standard to treat focal spasticity, and in SCI it can be used together with intrathecal baclofen (5). The most important goals of rehabilitation for patients with SCI are probably to avoid complications and to learn to live with the condition. However, a more difficult objective after SCI is to rehabilitate patients to be able to stand up and walk with the use of walking aids, particularly when the patient has a high neurological level of injury (thoracic or cervical). Many patients with SCI will use a wheelchair for the rest of their lives, but it has been suggested that upright mobility may improve cardiorespiratory function, urological drainage, bowel function, bone density, spasticity and contractures (6).
CASE REPORT
Case history
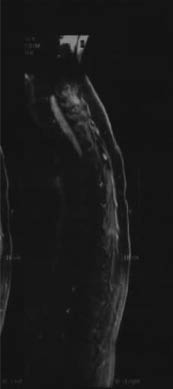
A 38-year-old woman had become paraplegic and care-dependent secondary to cervico-thoracic intramedullary ependymoma (Fig. 1). She reported that her symptoms had begun 3 years previously with weakness of the lower limbs, and balance and urinary disorders. After 4 months, she underwent magnetic resonance imaging (MRI), which showed an intramedullary ependymoma extending from C6 to T5. The neurological function of this patient was evaluated with a modified McCormick classification (7, 8). The patient was McCormick grade 2 in the pre-operative period (mild motor and sensory deficit, independent function and ambulation maintained). Three months later she was underwent surgery to remove the ependymoma. No adjuvant treatments (including radiotherapy and chemotherapy) were used in the post-operative period. Eight months after gross-total tumour resection, her neurological picture had changed, with spastic and painful lower limbs. The patient deteriorated to McCormick grade 4 post-operatively (severe sensorimotor deficit, restricted function, dependent). She did not report any other co-morbid pathologies.
Fig. 1. Magnetic resonance imaging (MRI) sagittal view of the spinal cord of the 38-year-old woman, showing her cervical-dorsal ependymoma.
Baseline clinical assessment
At initial evaluation, the patient was grade B on the American Spinal Injury Association (ASIA) scale (motor score 41) (9, 10) and presented painful spasticity of the lower limbs, which was being treated with oral anti-spastic (baclofen 25 mg 3 times a day; dantrolene 50 mg 3 times a day) and benzodiazepine (lorazepam tablet 2 mg, 1 tablet/day at night) with no therapeutic effect. She used a wheelchair and had a sacral pressure ulcer. She reported nausea and vomiting related to a high dosage of anti-spastic drugs; however, her spasticity was intractable and every attempt to move her lower limbs caused pain that increased the spasticity. The patient was evaluated using a Modified Ashworth Scale (MAS) (11), visual analogue scale (VAS) (12), and Spasm Frequency Score (SFS) (13). The SFS is a clinical scale used to assess the frequency of muscle spasms in hypertonic muscle: the score ranged from 0 (no spasms) to 4 (10 or more spasms per day), or continuous contraction. The MAS was 3/4 in the lower limbs (rigid in flexion position) pain was scored 8/10 on the VAS, and the patient reported a score of 4/4 on the SFS.
Combined treatment and clinical assessment at follow-up
After the initial evaluation, in order to reduce the generalized spasticity of the lower limbs and the side-effects of oral drugs, the patient was given continuous intrathecal baclofen infusion via a subcutaneously implanted pump. In this mode, a high degree of reduction in spasticity was noted, leading to a MAS score of 1/4. With this reduction in spasticity, the patient reported a significant reduction in painful daily spasms. In fact, the scores on both VAS and SFS improved, to 2/10 and 0/4, respectively. Seven days after positioning the baclofen pump, the patient began training with functional electrical stimulation (FES) cycling for 30 min/day, 5 days/week for 4 weeks. The patient also underwent an intensive rehabilitation programme, comprising passive joint extension and flexion, with assistance from physical therapists, and trunk mobilization to increase the torque of the upper limbs. The sacral pressure ulcer began to heal, and was completely healed a few months later. After increasing the torque of the upper limbs, with the aid of a standing device the patient was able to stand up progressively using her upper extremities (Fig. 2). She then began walking with an advanced reciprocating gait orthosis (ARGO). The ARGO comprises a hip-knee-ankle-foot orthosis that controls hip extension while assisting reciprocal hip flexion. The device stabilizes the lower limbs and the trunk in both the sagittal and frontal planes (14, 15). When she walked with the ARGO the patient reported increased painful spasms of toes of the feet, with bilateral rigidity in the flexion position, which compromised her gait. We decided to treat the muscle spasms and pain with botulinum toxin therapy. The patient was treated with botulinum neurotoxin type A (BTX-A) (NT 201 XEOMIN, Merz Pharmaceuticals GmbH, Frankfurt, Germany). Under electromyographic guidance, using a 1 ml syringe and a 26-gauge needle, the flexor digitorum brevis muscles were bilaterally injected in two places with a dose of 80 mouse units (UM) with 1 ml of saline dilution. The procedure was well tolerated and no adverse effects were noted. After BTX-A treatment, the patient was submitted to passive toes of the feet mobilization and stretching. Four days after the injections, the patient reported a regression of painful spasms. We observed that the pain level was significantly lower with BTX-A (VAS score: from 5/10 to 2/10 points after injections). After the painful spasms had reduced, the patient was able to walk more quickly with the ARGO and at the end of the training period (two months) her Walking Index for Spinal Cord Injury (WISCI) (16) level was 3 (Fig. 3). The WISCI was conceived as an instrument that would measure improvements in ambulation following SCI. After this combined treatment, the patient was classified as C grade on the ASIA scale (motor score 61).
Fig. 2. Following therapy with intrathecal baclofen, the patient was able to stand up.
Fig. 3. Following combined therapy with intrathecal baclofen and botulinum toxin type A, bilateral spasms in the flexor digitorum brevis muscles were reduced and the patient could walk faster with the advanced reciprocating gait orthosis (ARGO).
DISCUSSION
This case report describes the effect on locomotor function of a combined treatment of intrathecal baclofen, BTX-A, and a rehabilitation programme in a woman who became paraplegic and care-dependent secondary to cervico-thoracic intramedullary ependymoma. Ependymomas are the most common intramedullary tumour in adults, accounting for 60% of intramedullary spinal cord tumours (17, 18). Intramedullary ependymomas are observed most commonly in the cervical region, and almost all spinal cord ependymomas are histologically benign (7). Maximal resection of the tumour while protecting neurological function is the golden rule in surgical treatment of spinal ependymomas (7, 19, 20).
Many patients with SCI will use a wheelchair for the rest of their lives. An important objective of rehabilitation programmes in these patients is the recovery of gait. This objective is very difficult to obtain because it depends on the level and type of lesion. Spasticity is a major problem in SCI, and the use of intrathecal baclofen may be a useful therapy for patients in whom high dosages of oral anti-spastic agents are not effective or produce intolerable side-effect. Intrathecal administration of baclofen represents the best therapy to manage intractable and generalized spasticity. The use of botulinum toxin together with baclofen can be justified in the case of persistent focal spasms. In the present case, when the patient was able to stand up, she experienced painful dystonic movement and spasms bilaterally in her toes of the feet that interfered with her gait.
A few studies have reported combined treatment of spasticity with botulinum toxin injection and intrathecal baclofen (5, 21, 22). In fact, it is often sufficient to use intrathecal baclofen alone to reduce spasticity and to avoid the major side-effects of high dosages of oral baclofen. In our patient, BTX-A was added to increase the anti-spastic effect of intrathecal baclofen. We used a dosage of baclofen that did not completely eliminate spasticity, in order that the patient could stand up with the ARGO, since complete elimination of hypertonicity would not allow this. It is probable that by reducing the dosage of baclofen, the effect on spasticity was incomplete (spasticity was greater in the proximal muscles of the lower limbs than in the distal muscles) and after changing the position of the patient’s trunk, an increase in hypertonicity was noted, in particular bilaterally in the flexor digitorum brevis muscles.
Several studies have reported the effect of position change on spasticity, and the stretch reflex activity has been shown to play a role in the changed goniogram after position change. Increased spindle sensitivity might contribute as a direct result of muscle elongation or in combination with increased stiffness of the spastic muscles. A change in the biomechanical properties of other soft tissues in different positions is also a likely factor (23). Our patient did not exhibit this problem when she was FES cycling. In fact, our findings were similar to those of a study in which no reduction in spastic muscle tone was found after a 30-min passive cycling training in patients with SCI (24). The spasticity-reducing influence of FES has been demonstrated previously (25–27). Moreover, other studies have found that the combination of walking orthosis and FES can increase the effectiveness of ARGO more than traditional long leg braces (28). The use of botulinum toxin injections to the flexor digitorum brevis muscles, reducing the painful spasms of toes of the feet, enabled the patient to walk more easily and for a longer time. A few studies have reported the combined use of intrathecal administration of baclofen and botulinum toxin injections (15, 16). This combined treatment might improve the effect of baclofen on spasticity in small muscles or may enable a more focal effect. The present case report demonstrates the importance of a multidisciplinary approach in order to ease care and prevent complications in SCI. In this patient, combined treatment with intrathecal baclofen and botulinum toxin injections appeared to be safe and effective. The use of BTX-A may be an important adjunctive therapy to increase the effect of baclofen on spasticity in small muscles, obtaining a more focal effect, and improving the use of orthoses and the effectiveness of rehabilitation programmes in patients after SCI. Nonetheless, other case reports or small clinical series with BTX-A treatment and intrathecal administration of baclofen are needed to confirm these promising findings.
ACKNOWLEDGEMENT
The authors would like to thank Dr Sheila Abrusci for her help in editing the manuscript.
REFERENCES