Gerold Stucki, MD, MS (President ISPRM)1,2,3, Jan D. Reinhardt, PhD, (Secretary
ISPRM World Health Organization (WHO) Liaison Committee)1,2, Marta Imamura, MD, PhD (President Elect ISPRM)4, Jianan Li, MD (Vice President ISPRM)5 and Joel A. De Lisa, MD, MS (Immediate Past President ISPRM)6
From the 1Department of Health Sciences and Health Policy, University of Lucerne, Lucerne and SPF, Nottwil,
Switzerland, 2Swiss Paraplegic Research (SPF), Nottwil, Switzerland, 3ICF Research Branch, WHO FIC CC in German (DIMDI) at SPF, Nottwil, Switzerland, 4Division of Physical Medicine and Rehabilitation, Department of Orthopaedics and Traumatology, University of São Paulo School of Medicine, São Paulo, Brazil, 5First Affiliated Hospital of Nanjing
Medical University, Nanjing, China and 6Department of Physical Medicine and Rehabilitation, UMDNJ, New Jersey Medical School, Newark, NJ, USA
In 2008 the International Society of Physical and Rehabilitation Medicine (ISPRM) started an initiative to systematically develop its capacity and its internal and external policy agenda. This paper sums up achievements that have been made with this ISPRM initiative as well as pending issues and strategies to address them. The paper treats the following: ISPRM’s policy agenda in collaboration with the World Health Organization (WHO), research capacity in functioning and rehabilitation, ISPRM world conferences, relationships with regional societies of Physical and Rehabilitation Medicine (PRM), and ISPRM’s membership and governance structure.
Key words: rehabilitation; disability; societies; services; non-governmental organizations
J Rehabil Med 2011; 43: 1–7
Correspondence address: Gerold Stucki, Swiss Paraplegic Research (SPF) Guido A. Zäch Str. 4, CH-6207 Nottwil, Switzerland. E-mail: stucki.isprm@paranet.ch
Submitted November 19, 2010; accepted November 24, 2010
INTRODUCTION
At the beginning of the second decade of its existence, the International Society of Physical and Rehabilitation Medicine (ISPRM) is a successfully developing international non-governmental organization (NGO) in official relation with the World Health Organization (WHO). As the global agency for Physical and Rehabilitation Medicine (PRM), ISPRM serves as the international umbrella organization of PRM physicians. It achieves its goals by pursuing its humanitarian, scientific and professional mandate. It aims to “continuously improve PRM practice and facilitate PRM input in international health organizations with the goal to contribute to optimal functioning and quality of life of persons experiencing disability” (1).
To address the challenges typical for an expanding international NGO, in 2008 ISPRM started an initiative to: (i) develop its capacity; and (ii) systematically develop its internal and external policy agenda. The initiative to develop ISPRM has been described in detail in a special issue (1) on “Developing ISPRM” published in ISPRM’s official journal, the Journal of Rehabilitation Medicine. The articles in the special issue are available through open-access and can be downloaded either from the journal’s website (http://jrm.medicaljournals.se/) or from PubMed (http://www.ncbi.nlm.nih.gov/pubmed). The foreword provides a comprehensive overview of the different aspects of the initiative (1). Chapter 2 outlines “ISPRM’s way forward” (2) and chapter 6 provides an overview of ISPRM’s current internal and external policy agenda (3).
To ensure a transparent and democratic process with regard to a range of proposals, all ISPRM members received a copy of chapter 2 “ISPRM’s way forward” (2) on registration at ISPRM’s 2009 Congress, which was held in Istanbul, Turkey. The proposals were discussed during the Board of Governors meeting, which was held during the congress. They were further discussed in ISPRM’s Structural Reorganization Task Force and the relevant Committees. The respective motions were prepared during a retreat of the President’s Cabinet at Sun Moon Lake, Taiwan, in 2010 hosted by the Asia-Oceania Congress of PRM (AOCPRM), the second congress organized by the Asia-Oceania Society of PRM (AOSPRM). During its 2010 mid-term meeting held in the context of the 8th conference of the Mediterranean Forum of PRM in Limassol, the Board of Governors of ISPRM has approved a range of motions including a number of changes in its by-laws, as summarized in Table I. Most importantly, the Board of Governors has transformed itself into an Assembly of Delegates. The Assembly of Delegates is responsible for strategic decisions, by-law changes and the election of ISPRM officials.
| Table I. Motions of the By-Laws Committee passed at the 2010 Board Meeting at a glance |
| Agenda item/strategic goal | Motions | Status of ISPRM activity before BOG 2010 | Type of mandate |
| Enhancement of decision-making 1: BOG becomes Assembly of Delegates | 1. ISPRM change the name of the BOG to the Assembly of Delegates. 2. The Assembly of Delegates will be limited to ISPRM strategic issues such as: a. Approving by-laws b. Selecting sites of world congresses c. Approving strategic plans d. Approving collaborative plans e. Electing members of the Executive and Nominating Committees | Motion passed at BOG (Assembly of Delegates) meeting 2009 Submitted to By-Laws Committee | Professional Scientific Humanitarian |
| Enhancement of decision-making 2: Executive Committee | 1. The Executive Committee will be responsible for all ISPRM operational decisions as delegated to it by the BOG (Assembly of Delegates) with 2 exceptions: a. If a decision has to be made within 30 days b. If the Executive Committee fails to have a valid vote because too few of its members returned their votes | Motion passed at BOG (Assembly of Delegates) meeting 2009 Submitted to By-Laws Committee | Professional Scientific Humanitarian |
| Enhancement of decision-making 3: President’s Cabinet and President | The President’s Cabinet will be responsible for those ISPRM operational decisions the President refers to it, either because the ISPRM must complete a decision within 30 days, or the Executive Committee failed to provide a valid vote. The President may make operational decisions without a formal vote of the President’s Cabinet if the ISPRM must complete these decisions within 15 days or the President’s Cabinet failed to provide a valid vote. In such situations, the President must seek the advice of as many members of the President’s Cabinet as possible before making decisions. If the President must make decisions without a formal vote of the President’s Cabinet or Executive Committee, he/she must prepare a report to these governing bodies outlining the circumstances of the decisions. | Motion passed at BOG (Assembly of Delegates) meeting 2009 Submitted to By-Laws Committee | Professional Scientific Humanitarian |
| Enhancement of decision-making 4: Voting procedures | The ISPRM will adopt the following e-mail or web-based electronic voting procedures for all its governing bodies and committees: BOG (Assembly of Delegates): for a vote to be valid, at least 40% of its members must vote with a majority for acceptance and a 90 day time period for receiving votes. EC: for a vote to be valid, at least 40% of its voting members must vote with a majority for acceptance and 30 day period for receiving votes. The President’s Cabinet: for a vote to be valid, at least 60% of its voting members must vote with a majority for acceptance and a 15 day period for receiving votes. | Motion passed at BOG (Assembly of Delegates) meeting 2009 Submitted to By-Laws Committee | Professional Scientific Humanitarian |
| Increasing relevance of and income generated from ISPRM congresses | ISPRM hold yearly congresses. Applications for World Congresses will be 4 years prior to the projected date. Congresses should rotate among the following regions: Asia-Oceania, America, Africa, Eastern Mediterranean and Europe. | Recommendation of President’s Cabinet Motion passed at retreat in Taipei in May 2010 Submitted to By-Laws Committee | Professional Scientific |
| Enhancement of ISPRM’s institutional memory | Remove the limit on the number of terms that members of the By-Laws Committee can serve. | Recommendation of President’s Cabinet Motion passed at retreat in Taipei in May 2010 Submitted to By-Laws Committee | Professional |
| BOG: Board of Governors; ISPRM: International Society of Physical and Rehabilitation Medicine; EC: Executive Comittee. |
It was decided to maintain the Structural Reorganization Task Force founded at a retreat of the ISPRM’s President’s Cabinet in Nanjing, China (Yellow Mountain) in 2009 until the 2011 ISPRM meeting of the Assembly of Delegates in the context of the congress in Puerto Rico. The Structural Reorganization Task Force has been given the mandate to develop proposals for the following issues: (i) relationship with regional societies; (ii) renewed model for membership; (iii) democratic representation of individual and national members in the Assembly of Delegates and the Executive Committee; (iv) enhanced involvement of ISPRM in its annual world congresses; (v) approval process for discussion and position statements (including, for example, guidelines or curricula in PRM; policy recommendations).
ISPRM Committees and respective Sub-Committees will, in the future, take major responsibility for particular items of ISPRM’s internal and external policy agenda (3). In the following paragraphs, we briefly discuss key developments as outlined in Table VI of chapter 2 “ISPRM’s way forward” (2) as well as the internal and external policy agenda, as summarized in Table III of chapter 6 “The policy agenda of ISPRM” (3). Beyond the activities outlined in this paper, ISPRM is pursuing a range of additional, important activities, including the programmes led by its Educational Committee and its International Exchange Program.
ENHANCING THE ISPRM POLICY PROCESS AND AGENDA IN COLLABORATION WITH THE WHO
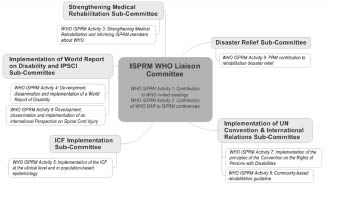
To host the expanding policy agenda in collaboration with the WHO and other rehabilitation organizations in official collaboration with WHO, ISPRM has expanded its WHO Liaison Committee, which now has 5 sub-committees. The sub-committees and their tasks according to the WHO-ISPRM work plan are shown in Fig. 1.
Fig. 1. Structure of International Society of Physical and Rehabilitation Medicine’s (ISPRM’s) World Health Organization (WHO) Liaison Committee/Sub-Committees and their alignment with specific tasks of the ISPRM WHO collaboration plan, as proposed by ISPRM for the period 2011–2013. DAR: Disability and Rehabilitation Team; IPSCI: International Perspectives in Spinal Cord Injury.
International relations and the implementation of the United Nations Convention on the Rights of Persons with Disabilities
The Sub-Committee on International Relations and the implementation of the United Nations (UN) Convention on the Rights of Persons with Disabilities will utilize and take as a model the existing relations of ISPRM with the Disability and Rehabilitation Team (DAR) Professional Organizations Network. This network involves the World Confederation for Physical Therapy (WCPT), the World Federation of Occupational Therapists (WFOT) and the International Society of Prosthetics and Orthotics (ISPO). The ISPRM Sub-Committee will seek to establish relations and work plans with other organizations in official relation with WHO, including Rehabilitation International (RI), in order to facilitate the implementation of the UN Convention on the Rights of Persons with Disabilities.
Implementation of WHO’s World Report on Disability and WHO’s International Perspectives in Spinal Cord Injury
The upcoming publications of the World Report on Disability and Rehabilitation and the subsequent spinal cord injury (SCI)-specific book on International Perspectives in Spinal Cord Injury (IPSCI) in 2011/2012 provides us with the unique opportunity to strengthen PRM and rehabilitation in general. The Sub-Committee on the Implementation of the reports will, in close collaboration with WHO’s DAR team and its Professional Organizations Network (including ISPRM, WCPT, WFOT, ISPO), establish dissemination channels for the reports and develop strategies for their implementation and evaluation (Table II).
| Table II. Pending items of International Society of Physical and Rehabilitation Medicine’s (ISPRM’s) policy agenda |
| Strategic goal | Internal/ external | ISPRM activities | Status of ISPRM activity |
| Enhancement of collaboration with regional PRM societies | Internal | Establishment of mutual recognition and collaboration plans with regional PRM societies (following the model of the WHO DAR/ISPRM collaboration plan) | Discussed in chapter 2 and 6 of JRM Special Issue on Developing ISPRM (1–3); respective motions are currently being prepared by Organizational Structure Task Force and will be discussed and voted upon by the Assembly of Delegates in 2011 (to be submitted to Delegates 90 days before the Assembly) |
| Enhancement of ISPRM congresses | Internal | Enhanced involvement of central offices in ISPRM congresses and of ISPRM officials in scientific committees and programmes | Proposals and draft contract for future congress organizers to be prepared by Congress Committee until mid-2011 (supposed to first apply to the ISPRM world conference with the call to be issued in 2011 and decision upon proposals to be made by the Assembly of Delegates in 2012) |
| Democratization of ISPRM governance structure and election procedures | Internal | Creation of Individual Members Assembly and move from nomination and approval to election of representatives by Assembly of Delegates Election of 3 representatives of individual members (1 per ISPRM area) and 9 representatives of national members (3 per ISPRM area) into Executive Committee by Assembly of Delegates to replace the current ISPRM regional vice-presidents | Discussed in chapter 2, 5 and 6 of JRM Special Issue on Developing ISPRM (2, 4, 3); respective motions are currently being prepared by the Organizational Structure Task Force and will be discussed and voted upon by the Assembly of Delegates in 2011 (to be submitted to Delegates 90 days before the Assembly) |
| Supporting the establishment of rehabilitation services worldwide | External | 1. Discussion paper with working title “ISPRM’s potential roles in fostering the establishment of PRM services in low resourced settings” | 1. Discussion paper currently under technical review by the WHO Liaison Committee |
| 2. New items for WHO DAR/ISPRM collaboration plan have been proposed by ISPRM | 2. Proposed new WHO DAR/ISPRM collaboration plan currently under review by the WHO |
| Developing rapid rehabilitation response to natural and man-made disaster | External | 1. Discussion paper with working title “Possible contributions of ISPRM to PRM disaster relief” | 1. Discussion paper currently under technical review by the WHO Liaison Committee |
| 2. New items on Disaster Relief in WHO DAR/ISPRM collaboration plan proposed by ISPRM | 2. Proposed new WHO DAR/ISPRM collaboration plan currently under review by the WHO |
| Enhancement of research capacity | External | Establishment of Research Task Force mandated to develop work plan | Founded by President’s Cabinet at the 2010 ISPRM retreat in Taiwan, work plan to be submitted to President’s Cabinet mid-2011 |
| |
| Development of ISPRM constituency and membership | External and internal | 1. Facilitation of foundation of PRM societies | 1. PRM societies in low-resource settings: Identification of white spots provided in discussion paper (5); work plan to be developed by Membership Committee and to be submitted to the President’s Cabinet mid-2011 |
| 2. Development of new membership models | 2. Membership models: respective motions are currently being prepared by the Organizational Structure Task Force and will be discussed at the Assembly of Delegates in 2011 |
| General curricula in disability and rehabilitation | External | Discussion paper with working title “General curricula on disability and rehabilitation in medical education” | 1. Draft being prepared by the Education Committee aligned with the WHO Liaison Sub-Committee on Strengthening Medical Rehabilitation; first draft to be submitted to the President’s Cabinet mid-2011 |
| Fighting discrimination | External | Implementation of the UN Convention | 2. Respective Sub-Committee of the WHO Liaison Committee will develop work plan to be submitted to the President’s Cabinet mid-2011 |
| Implementation of the ICF and ICF Core Sets | External and internal | 1. Adoption of ICF as general framework for functioning in PRM and endorsement of the WHO ICF Core Sets | 1. ICF/ICF Core Sets: motion passed in BOG 2009; By-Laws/PP changes to be prepared by By-Laws Committee up until March 2011 (90 days before the Assembly) |
| 2. Review on ICF implementation in rehabilitation hospitals and improvement of ICF implementation | 2. ICF Implementation: work plan to be developed by the WHO Liaison Sub-Committee on ICF Implementation up until mid-2011 |
| Contribution to WHO guidelines and glossary on terminology relevant to disability and rehabilitation | External | Community-based rehabilitation guideline | To be reviewed by the WHO Liaison Sub-Committee on UN Convention upon receipt from WHO |
| Strengthening medical rehabilitation through unifying terminology | External and internal | 1. Position papers on conceptual descriptions of the rehabilitation strategy and PRM | 1. Conceptual descriptions: currently revised by the WHO Liaison Sub-Committee on Strengthening Medical Rehabilitation and to be re-submitted to the President’s Cabinet mid-2011 |
| 2. Discussion paper on rehabilitation services within health services matrix | 2. Rehabilitation Service Matrix: in preparation by the WHO Liaison Sub-Committee on Strengthening Medical Rehabilitation |
| DAR: Disability and Rehabilitation team of the WHO; ICF: International Classification of Functioning, Disability and Health; ISPRM: International Society of Physical and Rehabilitation Medicine; PRM: Physical and Rehabilitation Medicine; WHO: World Health Organization; UN: United Nations. |
International Classification of Functioning, Disability and Health implementation
The International Classification of Functioning, Disability and Health (ICF) Implementation Sub-Committee is currently exploring possibilities for the system-wide implementation of the ICF for the provision of rehabilitation services in cooperation with current initiatives in a number of member societies. The sub-committee is also supporting the work of ISPRM’s President who serves as Chair of the Functioning Topic Advisory Group and member of the Revision Steering Group of the International Classification of Diseases (ICD-11) revision, which is currently in its alpha draft version.
Current tasks include: (i) a review of the current state of the implementation of the ICF in PRM practice, service provision and policy-making; (ii) a concerted ISPRM effort to contribute to the improvement of the ICF through evidence-based proposals in the soon to be opened WHO-ICF update platform; (iii) the development of the ICF Core Set-based scoring systems and measurement instruments; (iv) the development of ICF Core Set manuals for practice and service provision; (v) the development of models on how to use the ICF in the planning of clinical and cohort studies focusing on functioning and disability; (vi) the development of author guidelines on how to use the ICF in the reporting of studies (Table II).
Rehabilitation disaster relief
Based on the experience of ISPRM members in recent earthquake disasters in China in 2008 and Haiti in 2010, ISPRM has established the Sub-Committee on Rehabilitation Disaster Relief within its WHO Liaison Committee. Over the next two years, the Sub-Committee is developing a rapid rehabilitation response plan, which will enable ISPRM to serve as a catalyst of immediate PRM services in case of disasters. The Rehabilitation Disaster Relief Sub-Committee’s mission is effectively to focus the resources of ISPRM and its members to optimize health, functioning and quality of life of persons who sustain injuries or impairments after large-scale natural disasters. In the course of the 2011 ISPRM World Congress in Puerto Rico, a symposium on the issue of rehabilitation after natural disaster is planned, including the publication of a special or integrated supplement in ISPRM’s official journal, the Journal of Rehabilitation Medicine (Table II).
Strengthening medical rehabilitation
The Sub-Committee on Strengthening Medical Rehabilitation is developing a proposal to endorse conceptual, ICF-based descriptions of: (i) rehabilitation, a health strategy; as well as (ii) the medical specialty of PRM. The Sub-Committee can herein build on developments initiated by the Professional Practice Committee of the European Union of Medical Specialists (UEMS) in 2007 (6–8), which led to the approval of revised proposals by the UEMS section as well as the European Society of Physical and Rehabilitation Medicine (ESPRM) in 2010. All members of ISPRM are encouraged to contribute to the discussion towards an international consensus by writing a letter to our official journal, the Journal of Rehabilitation Medicine, or by writing to the chair of the WHO Sub-Committee on Strengthening Medical Rehabilitation (for the address, see ISPRM’s webpage).
The Sub-Committee on Strengthening Medical Rehabilitation is also developing a conceptual framework for rehabilitation services within the broader context of health services provision. Ultimately, this effort should lead to a convergence of our understanding of optimal service provision along the continuum of care, across sectors and over the lifespan (3). The taxonomy will be useful for the development and evaluation of rehabilitation services as well as policy recommendations (Table II).
ENHANCING ISPRM CONGRESSES
At its 2010 meeting, the Board of Governors approved the motion to move to yearly ISPRM congresses as well as a systematic rotation of the congress location in the 3 ISPRM Areas (in alphabetical order: 1 – Americas; 2 – Asia-Oceania; 3 – Europe, Eastern-Mediterranean, Africa) (2) from 2013 onwards. Accordingly, ISPRM will hold its congresses in Asia-Oceania (2013: Beijing; 2016: voting 2012); the Americas (2014: electronic voting at the beginning of 2011; 2017: voting 2013); and Europe, Eastern-Mediterranean, Africa (2015: Berlin; 2018: voting 2014). The ISPRM Board of Governors also approved a standard congress structure and a congress topic list for future ISPRM world congresses.
Until the 2011 ISPRM meeting in Puerto Rico, the ISPRM Organizational Structure Task Force develops, with involvement of the Congress Committee, a new contract for future ISPRM congresses that includes these standards as well as suggestions for an enhanced involvement of the Central Office. It will also develop a model for cooperation of ISPRM and national hosts with suitable regional societies including the Asia Oceania Society of PRM (AOSPRM), the ESPRM and the Asociación Médica Latinoamericana de Rehabilitación (AMLAR) as well as the Mediterranean Forum, which has an integrative role involving Europe, Eastern-Mediterranean and North-Africa (Table II).
STRENGTHENING FUNCTIONING AND REHABILITATION RESEARCH
The Board of Governors approved the motion to adopt the Journal of Rehabilitation Medicine as ISPRM’s only official journal. It also approved the concept of an international web of journals. The web of journals under the auspices of the Publication Committee provides PRM journals worldwide with the opportunity to be published in association with ISPRM or to be endorsed by ISPRM according to defined criteria (2). It is also intended to enhance the author guidelines of PRM through the inclusion of the ICF as standard for the reporting of persons’ functioning in studies.
A most important initiative is currently being developed by the Education Committee. It is the proposal to offer national societies the possibility to enrol trainees for the São Paulo/Harvard Clinical Effectiveness Program. The Principles and Practice of Clinical Research is an international collaborative distance-learning clinical research training programme offered by the Department of Continuing Education of Harvard Medical School. The course is designed for individuals who wish to gain basic advanced training in clinical trials before moving into the field, and for those who have experience in this area and aim to broaden their role in the design, management, analysis, and reporting of clinical trials (9).
To facilitate ISPRM’s role in strengthening functioning and rehabilitation research through collaborative research and the development of suitable research methodology, ISPRM has appointed a Task Force on Research. This Task Force is currently developing a plan towards the establishment of an ISPRM Research Committee (Table II).
ESTABLISHING COLLABORATIONS WITH REGIONAL SOCIETIES
Since the publication of the special issue on “Developing ISPRM” (1, 2), there has been an extensive discussion about the best model for cooperation between ISPRM and regional societies. The ISPRM Structural Development Task Force is addressing this issue and will present a proposal at the 2011 ISPRM Assembly of Delegates in Puerto Rico.
A concept that seems to gain momentum is the so-called “mutual recognition” and the appointment of reciprocal liaison officers with observer status at the ISPRM Assembly of Delegates and respective regional society assemblies. Most importantly, it is intended to develop 2–4 yearly collaboration plans with goals and milestones. In this respect, the WHO DAR/ISPRM Collaboration Plan may serve as a model (http://www.isprm.org/?CategoryID=353&ArticleID=170).
It also now seems clear that the model of regional vice-presidents, independent from the nominating and appointment process, may cause irritations within regional societies. Therefore, a model with elected regional representatives for national societies and individual members, as discussed in the next paragraph, seems to be an attractive alternative (Table II).
ISPRM GOVERNANCE AND MEMBERSHIP
Two important tasks of the ISPRM Structural Development Task Force are the development of a revised membership model addressing the issue of national, individual and combined membership, as well as a revised model for the representation of national societies and individual members in the Executive Committee and Assembly of Delegates.
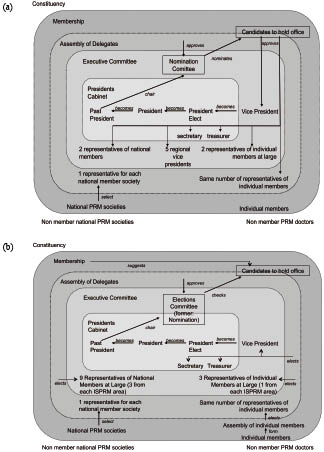
Fig. 2 shows the current governance model (Fig. 2a) and the model to be discussed (Fig. 2b), based on the considerations published in chapter 5 of the Special Issue on developing ISPRM (4).
Fig. 2. (a) Current governance model of the International Society of Physical and Rehabilitation Medicine (ISPRM). (b) Envisioned governance model of the ISPRM for discussion. PRM: Physical and Rehabilitation Medicine.
Model (b) has a number of advantages. These include bottom-up processes for the election of national societies and individual member representatives in the ISPRM Executive Committee by the new Assembly of Delegates. They also include the election of individual member representatives for the Assembly of Delegates through an Individual Members-Assembly to be created in the future.
Another model for national representatives in the Executive Committee that is to be discussed includes the suggestion to elect 3 representatives of national societies and 1 representative for the individual members for each of the 3 ISPRM Areas (2). Having 3 representatives from the national societies for each ISPRM Area seems to be advantageous across areas. In the ISPRM Area of the Americas, this would allow southern, middle and northern America to be represented. In the ISPRM Area of Europe, Eastern Mediterranean and Africa, a respective representation of each of those regions would be possible. Finally, in the ISPRM Area Asia-Oceania, a representation of the UN region Western Pacific would be assured by representatives of Asia-Western Pacific and Oceania-Western Pacific. In addition, there would also be a representative for South-East Asia (2). With respect to individual members, it is being discussed whether, in future, the representation of individual members should be balanced against a much larger representation of national societies, with many of them including a combined national and individual membership model. Therefore, it has been suggested that the ISPRM Assembly elects one representative of the individual members for each ISPRM Area to the Executive Committee (Table II).
The leadership of ISPRM is looking forward to develop our society in close collaboration with our national and individual membership, our colleagues from regional societies, our partners at the WHO and their Professional Organizations Network, as well as their Network of People with Disability Organizations. Together we can ensure that PRM physicians worldwide can provide effective, adequate and efficient services for patients along the continuum of care and over the lifespan.
ACKNOWLEDGEMENTS
The authors would like to thank the members of ISPRM’s Executive Committee (Maria Amparo Martinez Assucena, Maher Saad Benjadid, Alessandro Guistini, Juan Manuel Guzman, Marco Francheschini, Walter Frontera, Deog Young Kim, Jorge Lains, Leonard Li, John Olver, Nachum Soroker, Simon Tang, Mark Young, Chang-il Park, Linamara Battistella, Veronica Rodriguez de la Cruz, Christoph Gutenbrunner, as well as Werner Van Cleemputte), the chairs and Sub-Committee chairs of ISPRM Committees (John Olver, John Melvin, Guy Vanderstraeten, Andrew Cole, Bryan O’Young, Leonard Li, Walter Frontera, Nachum Soroker, Franco Franchignoni, Jorge Lains, Christoph Gutenbrunner, Martin Grabois, Alessandro Giustini, Marcelo Riberto) as well as the committee members and contributing national societies and individual members for their ongoing support of the development of ISPRM in its second decade. We would also like to thank Gunnar Grimby, the Editor, and the Editorial Office of ISPRM’s official journal, the Journal of Rehabilitation Medicine, for ongoing support of ISPRM’s development and good collaboration. Finally, we would like to thank Annette Frischmann for her support with the preparation of this special report.
REFERENCES