OBJECTIVE: To determine and compare haemodynamic responses at maximal arm-crank (ACE) and wheelchair exercise (WCE) in individuals with cervical spinal cord injury and pair-matched able-bodied individuals.
METHODS: Nine male, motor-complete cervical spinal cord injured and 9 able-bodied individuals performed graded, maximal ACE and WCE. Cardiac output, heart rate, and stroke volume were determined at rest and at maximal exercise in cervical spinal cord injured individuals. In able-bodied individuals, measurements were performed at rest and at the maximal workload of the matched cervical spinal cord injured individuals.
RESULTS: In cervical spinal cord injured, maximal cardiac output (ACE 7.4 (standard deviation (SD) 1.6); WCE 7.3 (SD 2.1) l/min) and heart rate (ACE 101 (SD 22); WCE 103 (SD 27) bpm) increased significantly compared with rest (4.6 (SD 1.0) l/min; 65 (SD 12) bpm), while stroke volume (ACE 77 (SD 22); WCE 73 (SD 21) ml) did not differ from rest (73 (SD 20) ml). In able-bodied individuals, cardiac output (rest 4.8 (SD 1.4); ACE 10.7 (SD 1.8); WCE 10.3 (SD 2.2) l/min), heart rate (rest 68 (SD 10); ACE 103 (SD 27); WCE 109 (SD 27) bpm), and stroke volume (rest 70 (SD 10); ACE 105 (SD 20); WCE 96 (SD 17) ml) increased significantly compared with rest. Cardiac output and stroke volume were significantly lower in cervical spinal cord injured compared with able-bodied individuals at the same workloads.
CONCLUSION: Haemodynamic responses to maximal exercise were similar for both exercise modes in individuals with cervical spinal cord injury. The lower cardiac output in individuals with cervical spinal cord injury compared with able-bodied individuals at equivalent workloads reflects the inability of the circulatory system to increase stroke volume.
Key words: cardiopulmonary arm exercise testing; gas exchange; haemodynamics; inert gas re-breathing.
J Rehabil Med 2012; 00: 00–00
Correspondence address: Christina M. Spengler, University and ETH Zurich, Exercise Physiology, Winterthurerstrasse 190, CH-8057 Zurich, Switzerland. E-mail: spengler@ethz.ch
Submitted March 21, 2011; accepted September 26, 2011
Introduction
Cervical spinal cord injury leads to altered cardiovascular regulation during exercise (1–3). Firstly, heart rate during exercise has been reported to be restricted to a maximum of 120–130 bpm in individuals with motor complete cervical spinal cord injury (cSCI) (4–6) resulting from the lack of supraspinal sympathetic nervous outflow directed to the heart (7). Secondly, a combination of low plasma catecholamine spill-over (8, 9) and diminished sympathetic outflow to the vasculature compromise vasomotion. As a result, ineffective blood redistribution (3, 10) and hypotension (11) are likely to occur during exercise in cSCI and these factors have been associated with venous blood pooling in the lower extremities (9). This may, in turn, impair venous blood return to the heart and adversely affect stroke volume (1, 12).
Impaired cardiovascular regulation and skeletal muscle paralysis below the neurological level of injury reduce exercise tolerance and compromise effective cardiovascular training. As a result, deconditioning and a sedentarism increase the risk of cardiovascular disease in cSCI (13). Regular physical exercise is known to improve many cardiovascular risk factors (e.g. blood lipid profile, insulin sensitivity, visceral fat) (2). However, to determine the most efficient cardiovascular training mode, it is important to evaluate cardiac output/stroke volume in response to exercise.
Several studies measured cardiac output in cSCI. However, they only assessed submaximal exercise responses (8, 10, 14–16). They reported elevated cardiac output and unchanged stroke volume in response to submaximal arm exercise training (16) compared with rest or increased cardiac output and stroke volume during leg exercise when using functional electric stimulation (8, 10, 14). However, the magnitude of cardiac output and stroke volume changes in response to maximal arm exercise in a homogeneous group of cSCI is yet unknown.
The primary aim of this study was therefore to determine cardiac output and stroke volume during maximal arm-crank (ACE) and wheelchair exercise (WCE), both of which are common training modalities in cSCI. The evaluation of maximal haemodynamic responses to exercise is necessary to determine the exercise mode with the highest potential to elicit training-induced central cardiovascular adaptations with, for example, high-intensity interval training. We reasoned that differences in metabolic (e.g. oxygen demand) or mechanical (e.g. propulsion technique, breathing pattern) properties between ACE and WCE might affect cardiac output and stroke volume differently.
Furthermore, we aimed to determine the factors that are relevant to exercise tolerance by comparing the respiratory demand, ratings of perceived exertion (RPE), and oxygen uptake between ACE and WCE. We also compared cSCI to pair-matched able-bodied individuals (AB) to determine the type of limitation specifically related to cSCI.
Methods
Participants
Nine men with traumatic spinal cord injury American Spinal Injury Association Impairment Scale (AIS) A or B (2 C5; 3 C6; 4 C7; time since injury 18 (standard deviation (SD) 11) years) and 9 pair-matched AB participated in the study. Participants were matched for age, weight, and physical activity. Subject characteristics are shown in Table I. After detailed information about the study protocol and testing procedures, written informed consent was obtained from each participant. The protocol was approved by the ethics committee of the canton of Lucerne (Switzerland). The study was performed according to the Declaration of Helsinki. Participants were required to refrain from strenuous physical activity for 48 h before the day of testing. Drinking caffeinated or alcoholic beverages on test days was forbidden and no food intake was allowed within the last 2 h before testing.
| Table I. Subject characteristics |
| | Cervical SCI Mean (SD) | Able-bodied Mean (SD) | p-value |
| Age, years | 43 (12) | 42 (12) | 0.825 |
| Height, cm | 178 (7) | 177 (7) | 0.824 |
| Weight, kg | 69 (12) | 73 (10) | 0.400 |
| Activity, h/week | 6.5 (3.0) | 4.6 (0.9) | 0.190 |
| VC, %pred | 85 (11) | 120 (30) | 0.001 |
| TLC, %pred | 90 (13) | 107 (23) | 0.019 |
| RV, %pred | 116 (38) | 95 (36) | 0.085 |
| FEV1, %pred | 83 (12) | 109 (25) | 0.002 |
| PEF, %pred | 77 (18) | 110 (28) | 0.003 |
| SCI: spinal cord injured; VC: vital capacity; TLC: total lung capacity; RV: residual volume, FEV1: forced expiratory volume in 1 s; PEF: peak expiratory flow; SD: standard deviation; %pred: %predicted. |
Study protocol
All individuals reported to the laboratory on 3 separate days. During the initial visit, individuals were familiarized with test procedures and instrumentation. Then, lung function was assessed according to standard procedures using a body plethysmograph (MasterLab, Jaeger, Würzburg, Germany). During the second and third visit, all individuals performed graded ACE or WCE to exhaustion (for details see below). The order of the test modes was randomized and balanced.
General exercise testing procedures
Upon arrival at the laboratory, individuals were asked to empty their bladder, then body weight was measured, and the tyre pressure of the wheelchair was adjusted to 6 bar. Individuals were then fitted with a forehead oxygen saturation sensor (8000R, Nonin Medical, Plymouth, USA) and a facemask (Hans Rudolph, Shawnee, USA), which was connected to the Innocor® system (Innovision, Odense, Denmark). The Innocor® system was used to measure ventilation and gas exchange breath-by-breath, and to determine cardiac output at rest and during exercise. All test protocols included at least 3 practice measurements of cardiac output, and 2 cardiac output measurements at rest, each preceded by 5 min of quiet breathing. During exercise, cardiac output was assessed at maximal exercise (for details see below) and RPE was assessed every minute using a 10-point scale. Numbers were read aloud and the subject nodded when the appropriate number was named. Blood pressure was measured at rest and immediately after exercise using an automated arm cuff (Omron, HEM-907, Omron Healthcare, UK). Capillary blood samples (20 µl) were collected from the earlobe before the start of the exercise test, as well as 2 and 4 min after exercise for the assessment of blood lactate concentration (Super GL, Ruhrtal Labor Technik, Möhnesee, Germany).
Maximal exercise test protocol
Maximal ACE and WCE protocols started at 3 W with increments of 3 (SD 0) W/min for ACE and 3 (SD 1) W/min for WCE until volitional exhaustion was reached. The initial treadmill speed for WCE was set at 1 km/h at an inclination of 1%. Treadmill speed was increased by 0.5 km/h for the 2 subsequent increments, followed by a 0.5% rise in slope. Alternate changes in speed and slope were continued until volitional exhaustion. The measurement of maximal cardiac output was initiated 30 s before individuals reached exhaustion. Since we expected AB to attain higher maximal workloads, incremental tests in cSCI were scheduled before those of AB, so that an additional cardiac output measurement could be performed in AB at the workload identical to the maximal workload achieved by the matched cSCI (isomax).
Arm-crank and wheelchair exercise equipment and settings
ACE tests were conducted with an electromagnetically braked, synchronous arm-crank ergometer (Ergoline, Höchberg, Germany). The centre of the crank shaft was set at the height of the subject’s shoulder joint. The elbow remained slightly bent when the arm was outstretched. Elastic straps were used to fix the hands to the handles of the ergometer. Assist to get up to speed was provided by the experimenters if required.
WCE tests were conducted on a motor-driven treadmill (Treadmill Giant, Bonte Technology, Groningen, The Netherlands) with a moving rail to prevent falls from the treadmill. A separate drag-test to determine the treadmill workload was performed before WCE started. Details of the drag-test can be found elsewhere (17). cSCI performed all tests in their own wheelchair. Chest straps or gloves were used if needed. AB performed all tests in the same standard wheelchair and were instructed to use mainly the heel of the hand for propulsion, similar to cSCI, and to relax the chest wall and leg muscles.
Cardiac output assessment
The technology of the Innocor® system to assess cardiac output is based on inert gas re-breathing using nitrous oxide and sulphur hexafluoride. The theoretical basis for this non-invasive technique, its application, and validity for exercise testing have been described previously (18–20). Briefly, prior to the cardiac output measurement, a re-breathing bag was filled with a specific gas mixture consisting of 28% oxygen, 0.5% nitrous oxide and 0.1% sulphur hexafluoride in nitrogen from atmospheric air. The filling volume was set at 40% of the individuals’ predicted vital capacity. If this was not achieved by the cSCI, then the filling volume was set at 44% of the effective vital capacity. Cardiac output measurements were performed at a breathing frequency of 18–22 breaths per min over a maximum of 20 s. Heart rate was measured by pulse oximetry and stroke volume was derived from cardiac output and heart rate.
Data analysis
Resting cardiac output measurements were averaged. Breath-by-breath data of physiological variables were averaged over 30-s intervals. The maximal workload was determined as the highest workload that was sustained for at least 30 s. The Wilcoxon sign-rank test was used for pairwise comparisons of haemodynamic data assessed at rest and during exercise. Between-group comparisons were performed using the Mann-Whitney U test. Analyses were performed using SPSS 17.0 (SPSS Inc., Chicago, USA) and statistical significance was accepted for p < 0.05. Data is given as mean (SD) if not otherwise stated.
Results
In AB, 3 maximal cardiac output measurements had to be excluded due to technical problems. Therefore, within-group comparisons of maximal haemodynamics in AB are reported for n = 6. All other within- and between-group comparisons are given for n = 9.
Maximal haemodynamics in cervical spinal cord injured compared with able-bodied individuals at identical workloads
Fig. 1 shows that maximal haemodynamic responses to exercise were not different between ACE and WCE in cSCI. While at maximal exercise, cardiac output and heart rate were significantly increased compared with rest, stroke volume and blood pressure (Table II) did not differ from resting values (blood pressure: systolic 103 (SD 15), diastolic 60 (SD 11) mmHg). Maximal heart rate of cSCI did not differ from heart rate at identical workloads in AB, while cardiac output and stroke volume were significantly lower in cSCI compared with AB.
| Table II. Peak responses to incremental arm-crank and wheelchair exercise in individuals with cervical spinal cord injury (SCI) (n = 9) |
| | Arm-crank Mean (SD) | Wheelchair Mean (SD) | p-value |
| Workload, W | 42 (17) | 31 (13) | 0.015 |
| Push rate, rpm | 60 (3) | 65 (13) | 0.441 |
| Oxygen uptake, ml/kg/min | 15 (7) | 14 (5) | 0.383 |
| Oxgen saturation, % | 98 (1) | 98 (2) | 0.489 |
| Lactate, mmol/l | 3.1 (1.8) | 3.3 (1.8) | 0.767 |
| Systolic blood pressure, mmHg | 96 (18) | 95 (38) | 0.953 |
| Diastolic blood pressure, mmHg | 54 (19) | 47 (15) | 0.176 |
| SD: standard deviation. |
Fig. 1. Haemodynamic responses to arm exercise. Values are means (standard deviations). SCI: spinal cord injured; max: maximal workload in SCI; isomax: workload in able-bodied identical to max; CO: cardiac output; SV: stroke volume; HR: heart rate. *p < 0.05 significant difference between rest and exercise.
Exercise responses in cervical spinal cord injury compared with able-bodied individuals at identical workloads
Table II shows maximal ACE and WCE data of cSCI. Eight out of 9 cSCI achieved higher workloads during ACE compared with WCE. Otherwise, no differences were found in maximal responses between ACE and WCE.
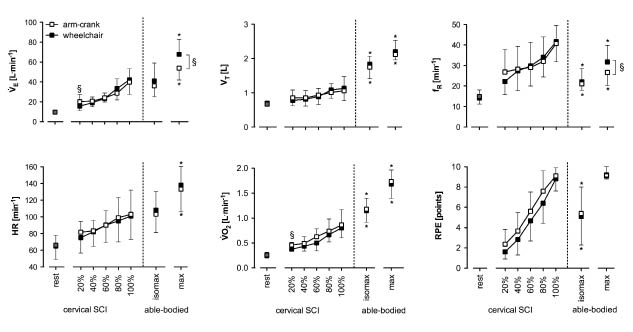
End-tidal carbon dioxide pressure during maximal exercise was significantly lower compared with rest (rest 38 (SD 3), exercise 32 (SD 5) mmHg) and compared with AB at isomax (rest 37 (SD 2), exercise 38 (SD 2) mmHg). The ventilatory equivalent for oxygen was significantly higher at maximal exercise for cSCI compared with AB at isomax (cSCI 50 (SD 9), AB 33 (SD 4)).
Fig. 2 shows that all exercise responses were elevated compared with rest, and continued to increase with exercise intensity. For cSCI, the increase in tidal volume from rest to maximal exercise was only 0.4 (SD 0.1) l and absolute tidal volume did not exceed 1.1 (SD 0.4) l (in percent of vital capacity: ACE 26 (SD 9), WCE 28 (SD 8)%). Accordingly, increases in minute ventilation were predominantly achieved through increases in breathing frequency. Conversely, oxygen uptake and tidal volume were higher in AB and breathing frequency was lower compared with cSCI at the same minute ventilation.
Fig. 2. Physiological responses and ratings of perceived exertion during graded arm exercise. Values are means (standard deviations). §p < 0.05 significant difference between arm-crank and wheelchair exercise. *p < 0.05 significantly different from 100% of SCI. SCI: spinal cord injured; max: maximal workload; isomax: workload in able-bodied identical to 100% cervical SCI; 20–80%, workload in % of the maximal workload (100%); V.E: minute ventilation; VT: tidal volume; fR: breathing frequency, HR: heart rate; V.O2: oxygen uptake; RPE: ratings of perceived exertion.
Maximal exercise responses in able-bodied individuals
Table III shows haemodynamic responses to maximal ACE and WCE for the 6 AB. Maximal workload (n = 9) for ACE (73 (SD 14)W) was significantly higher compared with WCE (53 (SD 11)W). Maximal heart rate, oxygen uptake, blood lactate concentration (ACE 4.4 (SD 1.7), WCE 5.1 (SD 1.4) mmol/l), and tidal volume relative to vital capacity (ACE 38 (SD 9), WCE 39 (SD 6) %) were similar for ACE and WCE, and were significantly higher compared with cSCI. Maximal minute ventilation and breathing frequency were lower for ACE compared with WCE (Fig. 2).
| Table III. Haemodynamic responses to maximal arm-crank and wheelchair exercise in able-bodied individuals (n = 6) |
| | Arm-crank Mean (SD) | Wheelchair Mean (SD) | p-value |
| Cardiac output, l/min | 12.1 (2.4) | 13.1 (2.3) | 0.345 |
| Stroke volume, ml | 83 (14) | 91 (21) | 0.345 |
| Heart rate, bpm | 146 (24) | 144 (16) | 0.344 |
| Systolic blood pressure, mmHg | 160 (30) | 165 (33) | 0.465 |
| Diastolic blood pressure, mmHg | 72 (8) | 78 (9) | 0.223 |
| SD: standard deviation. |
Discussion
There are two main findings in this study. Firstly, we demonstrate that haemodynamic and respiratory responses to maximal ACE and WCE did not differ between ACE and WCE in cSCI. Secondly, we show that the increase in cardiac output was achieved by an increase in heart rate only, while stroke volume remained near pre-exercise levels even at maximal exercise in cSCI.
These findings have both physiological and practical relevance. From the physiological view, it appears that the limits to increase cardiac output are governed by a restriction to increase stroke volume and by a low maximal heart rate, which are most likely a consequence of the disturbed sympathetic nervous system in cSCI. The fact that stroke volume increased at isomax in AB confirms that this intensity of upper body exercise has, in general, the potential to increase stroke volume. In practice, these findings support the view that conventional ACE and WCE exercise might not provide an adequate training stimulus to elicit central training adaptations in cSCI (1, 3).
Exercise tolerance in cervical spinal cord injury
Peak oxygen uptake in cSCI was within the mean range for this population (21). In addition, a substantial contribution of anaerobic energy supply to maximal exercise performance was present, shown by increased blood lactate concentration, increased ventilatory equivalent for oxygen, and low end-tidal carbon dioxide pressure at maximal exercise.
Low active muscle mass and high muscle fatigability are commonly presumed to be the major limiting factors for exercise performance in cSCI (1, 3, 22, 23). However, since stroke volume did not increase above resting values during arm exercise in our set-up, oxygen transport to the exercising muscles might have been restricted by the inability of the cardiovascular system to further increase cardiac output. Based on the present findings, improvements in maximal ACE and WCE performance could probably only be expected from enhanced oxygen extraction or by an increase of non-oxidative muscle mass. Interestingly, Schantz et al. (24) showed that trained cSCI displayed a higher proportion of oxidative type I fibres in the deltoid muscle compared with AB, which might be a compensatory mechanism of the periphery in response to the central limitations.
Maximal arm-crank vs wheelchair exercise
The higher workload achieved with ACE is probably related to the higher mechanical efficiency during ACE compared with WCE (25, 26). During ACE, force can be applied continuously, while during WCE, force is applied at only 20–40% of the 360º cycle (27). Differences in force production, movement pattern and trunk stabilization between ACE and WCE result in a similar metabolic cost, e.g. similar oxygen consumption and blood lactate concentration, at maximal exercise despite the higher workload achieved with ACE. Therefore, ACE might be preferential for outdoor activities involving inclines or to cover long distances.
However, with respect to training, which is generally performed at submaximal workloads, both modes are similar, as no substantial differences in physiological responses or RPE were found, at identical percentages of maximal workload. Accordingly, it could be concluded that ACE and WCE do not differ in their suitability to train the cardiorespiratory system. Nonetheless, the submaximal exercise mode, which can be sustained for a longer duration, might be more beneficial for the improvement of cardiovascular health (2, 5).
Exercise ventilation
Interestingly, tidal volume remained low in cSCI, while minute ventilation and breathing frequency increased with exercise intensity. Also, compared with AB, cSCI breathed at a lower percentage of their vital capacity, possibly because the diaphragm also acts as a postural muscle in cSCI (28). Therefore, the smaller tidal volume might reflect a compromise between respiratory needs and maintaining upper body balance. In addition, the small tidal volume might also result from the limited ability to expire actively.
Furthermore, reduced active respiratory muscle mass increases the overall demand on the diaphragm and its susceptibility to fatigue (29). In AB, exercise-induced diaphragmatic fatigue has been proposed to attenuate blood flow to locomotor muscles as a result of sympathetically mediated vasoconstriction due to the competition for blood flow between respiratory and locomotor muscles (30). It cannot be ruled out that competition for blood flow between respiratory and arm muscles occurred in the present study, thereby affecting exercise performance. However, since sympathetic vasoconstrictor activity cannot be activated from the cardiovascular centres in cSCI (7), it is unlikely that this mechanism affected exercise performance in this population.
Despite the high demand on the respiratory system in cSCI, evidence that the respiratory system does not limit exercise performance is provided by Taylor et al. (23), who did not observe exercise-induced diaphragmatic fatigue after intensive constant-load arm crank exercise in highly trained cSCI. These authors propose that their findings can be extended to less fit cSCI, since these individuals will be even less able to reach the limits of their breathing capacity.
Technical considerations
A first consideration is that the inert gas re-breathing system (Innocor®) used to assess cardiac output in the present study was not specifically validated in SCI individuals by comparison with a gold-standard. We infer the validity of our measurements from published literature in cardiac and intensive care patients that found good agreement between cardiac output assessed by inert gas re-breathing and gold-standard thermodilution (18, 31) at rest and during exercise. Also, cardiac output measurements of Innocor® and the non-invasive gold standard, cardiac magnetic resonance imaging, were shown to agree well (32) and the validity of inert gas re-breathing (Innocor®) is similar to that of, for example, carbon dioxide re-breathing (33), the latter being used many times to assess cardiac function in individuals with SCI at rest and during exercise (15, 34–36). Furthermore, a chronically altered pulmonary system could theoretically compromise the assessment of cardiac output by re-breathing. However, Saur et al. (37) showed, for example, good agreement of inert gas re-breathing with non-invasive gold standard measurements in individuals with obstruction, restriction and compromised lung diffusion capacity. Finally, reproducibility of cardiac output measurements by use of Innocor® system is in the range of gold standard (coefficient of variation 5–10%) at rest and during exercise (20, 38) also in cSCI (39).
Secondly, our sample size was small, but the inclusion criteria restricted the available number of active and otherwise healthy cSCI. To partly overcome this issue, we included pair-matched AB for comparisons. A sample size of n = 9 is capable of detecting between condition cardiac output differences of 15% of maximal exercise in cSCI with 80% power and 5% alpha error based on the standard deviation of repeated cardiac output measurements on different days.
Thirdly, motor- and sensory-complete cSCI (AIS A) might differ from motor-complete and sensory-incomplete cSCI (AIS B) concerning sympathetic activity. However, individual data did not reveal any signs of elevated sympathetic activity (e.g. exercise heart rate above 130 bpm, stroke volume above resting values) related to the type of classification.
Finally, blood pressure was measured immediately after stopping, rather than during maximal exercise to avoid interference with cardiac output measurements. Blood pressure assessed immediately after exercise may not necessarily reflect blood pressure at peak exercise. However, the present blood pressure data (rest: 106/60 mmHg; post-exercise: 96/54 mmHg) in individuals with cSCI compares well with that published previously (Claydon et al. (40) rest: 96/61 mmHg; post-exercise: 81/54 mmHg).
In conclusion, we could show that maximal ACE and WCE are equivalent with respect to cardiorespiratory stress, but even maximal load seems to be insufficient to elicit adequate volume loading of the heart to maximally stress central haemodynamic mechanisms (3). Therefore, increases in maximal cardiac output and stroke volume are most likely not to be expected even when including maximal bouts of ACE and WCE in high-intensity interval training. Thus, more effective exercise modes, e.g. functional electric cycling or exercise in different body positions, should be considered in order to train the cardiovascular system in cSCI.
AcknowledgEments
The authors would like to thank all volunteers for their time and effort dedicated to this study and Dr. Ruth Briggs for proofreading the manuscript. The study was supported by the Swiss National Science Foundation (SNSF, grant no. 32-116777). The SNSF was not involved in study design, collection, analysis and interpretation of data, writing of the report or the decision to submit the paper for publication.
The authors have no conflicts of interest to disclose.
References