BACKGROUND: Rehabilitation is effective and beneficial for patients with arthritis. The lack of a common structure for describing the content of rehabilitation makes it difficult to compare, transfer and implement research evidence into clinical practice.
OBJECTIVE: To develop a framework comprising domains and elements of importance when describing arthritis rehabilitation.
METHODS: On the basis of a systematic literature search and review, the framework was developed through a 9-step development process, including 5 Delphi consensus rounds within the Scandinavian Team Arthritis Register – European Team Initiative for Care Research (STAR-ETIC) collaboration, a group of clinicians, researchers and patients from northern Europe.
RESULTS: Based on Donabedian’s healthcare model, the International Classification of Function, Disability and Health, and a rehabilitation model by D. T. Wade, 4 domains (context, structure, process and outcome) were defined. Within each domain, the most important and relevant key elements for describing rehabilitation were selected. This framework contains 1 key element under context, 9 under structure, 3 under process, and 9 under outcome.
CONCLUSION: The STAR-ETIC framework can be used to describe arthritis rehabilitation, by emphasizing key elements in 4 main domains. A common framework may facilitate comparisons of rehabilitation programmes across countries and different levels of care, and may improve the implementation of rehabilitation research in clinical practice.
Key words: arthritis; rehabilitation; framework; context; structure; process; outcome.
J Rehabil Med 2012; 00: 00–00
Guarantor/Correspondence address: Mari Klokkerud, National Resource Centre for Rehabilitation in Rheumatology, Diakonhjemmet Hospital, PO Box 23, NO-0319 Oslo, Norway. E-mail: mklokkerud@hotmail.com
Submitted May 9, 2011; accepted December 13, 2011
Introduction
Arthritis comprises over 100 different chronic conditions, both inflammatory and non-inflammatory, causing damage to the joints of the body. With an increasing proportion of elderly people in Western societies, the socioeconomic costs of arthritis are rising continuously. Despite improvements in medical, pharmacological and surgical treatment, special rehabilitation strategies are often required. Rehabilitation for patients with arthritis has a long tradition in Europe (1, 2), yet there is no consensus or recommendations regarding what rehabilitation for patients with arthritis should include (3), and differences are considerable around the world (4).
The World Health Organization (WHO) defines rehabilitation as “a process intended to enable people with disabilities to reach and maintain optimal physical, sensory, intellectual, psychological and/or social function” (5). Rehabilitation interventions are complex and provided by trans-, inter- or multi-disciplinary teams of health professionals. Complex interventions combine a number of components, which may act independently and interdependently (6). The large number of outcomes and degree of flexibility when tailoring interventions also contributes to their complexity (7), helping to explain why rehabilitation has been called “the archetypical complex intervention” (8).
A detailed description of interventions is crucial to enable comparison of effectiveness across studies and replication of interventions in research and clinical practice (7). However, systematic reviews show that such descriptions are often incomplete or lacking in research reports (9, 10). Classification systems (11, 12), and taxonomies (13) do exist, but are too extensive to be feasible for standard reporting of research. Agreement on a common framework1 for describing rehabilitation interventions may improve the quality of rehabilitation studies published. Such a framework should designate the most important domains and elements of what should be described. It should not be too detailed and rigid, but feasible for use in different settings and for different objectives within arthritis rehabilitation.
1A framework is defined as a basic structure underlying a system, concept, or text (14).
The most highly established framework within the field of rehabilitation is the WHO’s International Classification of Function, Disability and Health (ICF), which provides an international and inter-professional scientific basis for understanding and studying health (15). The ICF can serve as a framework for linking rehabilitation goals (16), interventions and outcome measures (17), and to describe and measure health impact and disability (18–20).
A procedure for describing rehabilitation along 3 axes (structure, process and outcome) has been suggested by Wade (8) and Wade & Jong (21). In this suggestion one can recognize terms from Donabedian’s widely used healthcare model. According to Donabedian’s model, structure is the conditions under which care is provided, process comprises the activities that constitute healthcare, and outcome refers to changes (desirable or undesirable) in individuals and populations that can be attributed to healthcare (22).
The objective of this study was to develop a framework identifying domains and elements of importance for rehabilitation, based on the ICF and the models of Donabedian and Wade. The final framework should be feasible for basic descriptions of arthritis rehabilitation in different settings and purposes.
Material and methods
Literature search
A systematic literature search was carried out to ascertain whether a framework for describing arthritis rehabilitation care already existed. The databases AMED, MEDLINE, EMBASE, Cinahl, PsychINFO, Cochrane and PEDro were searched from 1 January 1990 to 30 October 2009. Search terms were “Team Care” AND “Arthritis” AND “Rehabilitation”. Only papers in English were selected. Four researchers, working in pairs, carried out the review. Each pair reviewed approximately half of all the abstracts and relevant full-text articles.
To exclude that a potential framework existed, we conducted a systematic literature search with the following inclusion criteria ”articles with the primary aim of describing a model/framework of rehabilitation for patients with rheumatic diseases”.
Delphi procedure
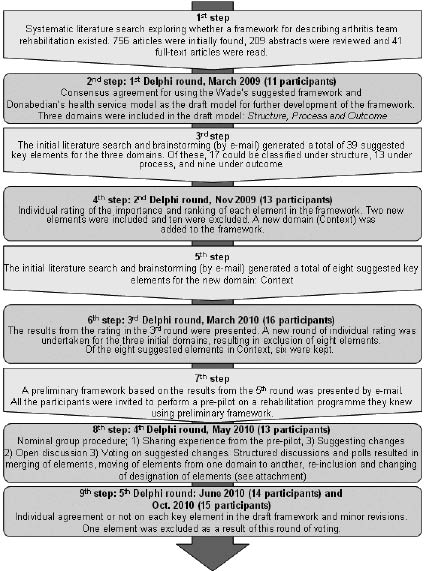
A Delphi consensus procedure is useful when there is little existing evidence. It is a method to obtain relevant intuitive insights from experts and use their informed judgement as systematically as possible (23). The Delphi technique has 4 characteristics that distinguish it from other group decision-making processes: (i) anonymity, (ii) interaction with feedback, (iii) statistical group responses, and (iv) expert input (24). The development process is described in Fig. 1.
Fig. 1. Steps in the development process of the STAR-ETIC Framework including the five Delphi rounds. STAR-ETIC: Scandinavian Team Arthritis Register – European Team Initiative for Care Research
Members of the Scandinavian Team Arthritis Register – European Team Initiative for Care Research (STAR-ETIC) project group participated in the development process. STAR-ETIC is a European initiative among researchers, clinicians and patient representatives from Sweden, Norway, Denmark and the Netherlands. The common goal for the STAR-ETIC collaboration is to create a basis for registration of team care interventions in arthritis and to explore different aspects of the structure, process and outcome of team care in hospitals and rehabilitation units in Europe.
Because of the professional and personal competencies and the different nationalities it encompasses, the STAR-ETIC collaboration was considered an appropriate group of stakeholders for developing this new framework. Interaction within the group was both by e-mail and face-to face contact at regular STAR-ETIC meetings. All participants completed a questionnaire regarding age, sex, professional background and level of education.
In the first Delphi round, a consensus agreement was made to use Wade’s (8, 21), the ICF (25) and Donabedian’s (22) models as the basis for the development process. An initial draft model was developed consisting of 3 domains: structure, process and outcome. The literature gathered through the initial systematic literature search and a group brainstorming session were used to generate a comprehensive list of elements for each domain in the new framework.
The importance of each element was rated in several rounds, using numerical rating scales from 1 to 5 (1 = very important, 5 = not important at all). Each participant also suggested a ranking within each domain, starting from 1 for the most important element to keep in the framework.
A mathematical procedure, based on product (importance × ranking), determined the inclusion or exclusion of elements in the framework throughout the Delphi rounds. Additional domains and elements could be suggested until the final round, but had to be rated as important or very important by at least 75% of the participants in the subsequent round of scoring (26). A consensus threshold of 75% agreement was also used in the final round, where a dichotomous rating of all the remaining elements determined the key elements in the final framework.
Results
Participants
A total of 16 persons from the STAR-ETIC collaboration participated in the Delphi process: 12 women and 4 men. The mean age of the participants was 51.3 years (range 35–73 years). Nine participants had studied to PhD level, including 4 professors, 3 participants had a Master’s degree, and 4 had studied to Bachelor’s level. A variety of disciplines were represented: 3 rheumatologists, 7 physiotherapists, 3 occupational therapists and 3 patient representatives. Of the health professionals, 1 worked primarily in clinical practice, 4 worked in both clinical practice and research, and 7 worked primarily in research. One of the professionals did not fit into any of the categories on this question and answered “other”.
Results of the literature search and the Delphi procedure
The literature search identified 209 potential titles/abstracts, of which 41 were retrieved for full-text reading. None of the frameworks, taxonomies and models found had been developed or tested for arthritis rehabilitation care.
The framework development process consisted of a total of 9 steps, including the initial literature search, consensus agreement on the draft model, element generation (brainstorming and literature search) and 5 Delphi rounds with anonymous voting (Fig. 1). During the third and fourth steps, a fourth domain, ”context”, was added to the initial 3 domains: structure, process and outcome. The 6th and 7th Delphi rounds included pre-piloting of the framework. All participants were invited to describe a rehabilitation programme they were very familiar with. A nominal group procedure was then used, as a supplementary method, with an open discussion about the feasibility of the framework. This procedure allows the participants to list ideas for adjustments in a round-robin format, and discuss each idea before voting on the options (26). This discussion was considered crucial to ensure the clinical quality and feasibility of the final framework. In this round, participants were allowed to suggest changes to the framework and re-include previously excluded elements. Problems related to the framework and suggested solutions were summarized and followed up by anonymous rounds of voting on each suggested solution. A total of 15 persons participated in the final consensus round, which was concluded with a dichotomous voting on each element in the final framework. The Delphi process resulted in a framework with 22 elements categorized into the following 4 domains: context, structure, process and outcome.
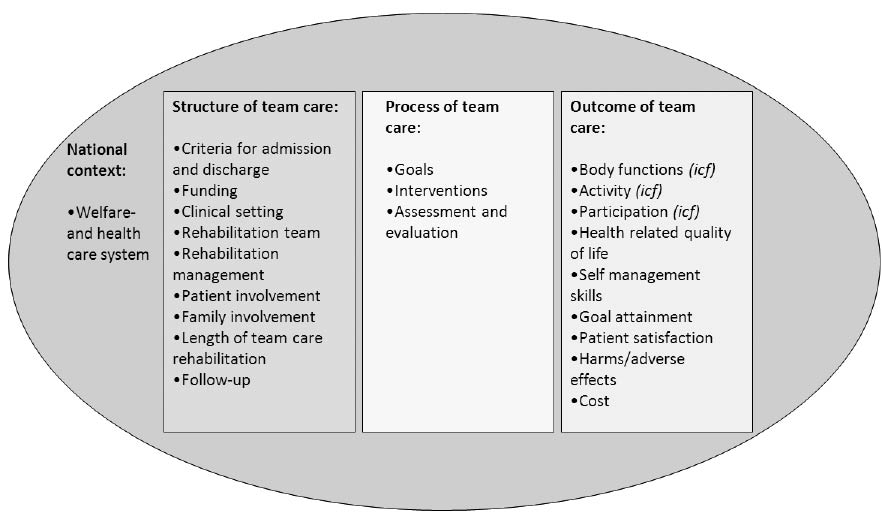
Context describes the national welfare and healthcare system. Structure encompasses the following: criteria for admission and discharge, the funding of the rehabilitation, the clinical setting, the rehabilitation team, the type of rehabilitation management that is guiding the programme, whether there is a structure guiding the length of rehabilitation, how patient involvement and family involvement is addressed, and, finally, whether there is a structure for follow-up. Process comprises a description of rehabilitation goals, interventions, assessment and evaluations. Outcomes should be described as elements according to the ICF categories: body functions, activity and participation. Furthermore, it may be relevant to describe changes in health-related quality of life, self-management skills, goal attainment and patient satisfaction. Finally harms/adverse effects and costs are also considered important. The final STAR-ETIC framework is presented in Fig. 2, and explained in more detail and with definitions in Table I.
Fig. 2.The STAR-ETIC Framework.
STAR-ETIC: The Scandinavian Team Arthritis Register-European Team Initiative for Care Research. ICF:International Classification of Function, disability and health..
| Table I. The STAR-ETIC Framework. STAR-ETIC: The Scandinavian Team Arthritis Register-European Team Initiative for Care Research |
| Domains and key elements | Definitions |
| Context | |
| Welfare and healthcare system | Welfare: statutory procedure or social effort designed to promote the basic physical and material wellbeing of people in need (27). Healthcare: the organized provision of medical care to individuals or a community (28). |
| Structure | |
| Criteria for admission and discharge | Admission: the process or fact of entering or being allowed to enter a place or organization (29). Discharge: the action of discharging someone from a hospital (30). |
| Funding | Funding: money provided, especially by an organization or government, for a particular purpose (31). |
| Clinical setting | Clinical: of or pertaining to a medical clinic or facility (32). Setting: the place or type of surroundings where something is positioned or where an event takes place (33). |
| Rehabilitation team | Three models of care have been distinguished: 1) a multidisciplinary approach, in which different team members cooperate on a regular basis while staying within their professional boundaries; 2) an interdisciplinary team model, in which the members analyse, synthesize, and harmonize links between disciplines to establish a shared basis of knowledge and common goals in the treatment or rehabilitation of the patient; 3) a trans-disciplinary model where members transcend their traditional boundaries and take on extended roles to be able to meet a patient’s need for more rapid access to care, to provide more time and continuity in care, or to provide a more optimal treatment when funding or human resources are limited (34). |
| Rehabilitation management | Rehabilitation management can be characterized by a problem-solving approach. It enables all professionals involved in patient care to coordinate their actions (20). |
| Patient involvement | Patient involvement is described in the literature as Patient-centred healthcare. There is no globally accepted definition of patient-centred healthcare. The International Alliance of Patients’ Organizations (IAPO) proposes that patient-centred healthcare is a useful concept to ensure that patients’ needs and preferences are at the centre of all aspects of healthcare. Patient-centred healthcare should stress the importance of equality and respect in all relationships in healthcare (35). |
| Family involvement | Family: a group of people affiliated by consanguinity, affinity, or co-residence (36). |
| Length of team care rehabilitation | Period of time from admission to discharge. |
| Follow-up | Follow-up: a continuation or repetition of something that has already been started or done. A piece of work that builds on or exploits the success of earlier work (37). |
| Process | |
| Goals | A goal is the object or aim of an action, usually within a specified time limit (38). |
| Interventions | Rehabilitation interventions can be defined as any intervention that reverses, prevents worsening of or alleviates an impairment and attempts to reduce disability or distress. Two important components of interventions: 1) Quality (who did it? what did they do?); 2) Quantity (how much?) (39). |
| Assessment and evaluations | Assessment is a plan of care that identifies the specific needs of the client and how those needs will be addressed by the facility (40). Evaluation is systematic determination of merit, worth, and significance of something or someone using criteria against a set of standards (41). |
| Outcome | |
| Body functions (ICF) | Body functions are the physiological functions of body systems (including psychological functions) (25). |
| Activity (ICF) | Activity is the execution of a task or action by an individual (25). |
| Participation (ICF) | Participation is involvement in a life situation (25). |
| Health-related quality of life | Although there is no universal definition of health-related quality of life, there is growing consensus that it should be assessed multidimensionally, including physical health, psychological state, and social relationships. Moreover, quality of life and health status are distinct constructs. Quality of life is determined not only by the patient’s health status problems but also by their emotional response to these problems (42). |
| Self-management skills | Self-management is defined as “strategies individuals use to manage symptoms, treatments and life-style changes inherent in their chronic condition, in order to achieve better functional capability, fewer complications and increased psychosocial wellbeing” (43). |
| Goal attainment | The extent to which the intended goals are achieved (44). |
| Patient satisfaction | Measures of patient satisfaction with rehabilitation should include items regarding progress and degree of return to independent living (45). Wade et al. (46) suggest the phrase Customer satisfaction and says that this has two angles. One is an independent variable consisting of ”compliance, service utilization and efficacy of intervention”. The other is a dependent variable concerning ”the patient’s previous experiences with services, attitudes towards life, self-esteem, and illness behaviour”. |
| Harms/adverse effects | Several types of adverse effects exist. Societal adverse effects arise when resources are used that deliver less benefit than an alternative use of the same resource. Patient adverse effects may be transient or permanent, and may be inevitable, or arise by change, or arise predictably in a proportion of people (47). |
| Cost | Cost of illness could be described by direct costs and indirect costs. Direct costs are defined as those costs for which actual payments are made (e.g. treatment costs, hospital costs and medication, transport costs to the health provider and specialist aids etc.). Indirect costs are costs for which resources are lost, but no direct payment is actually made (e.g. productivity losses) (48). |
Discussion
Based on research evidence and clinicians’ and patients’ expertise, a framework for describing arthritis rehabilitation has been developed. The framework designates domains and elements of essential importance when describing an arthritis rehabilitation programme. The overall aim is that the framework may serve as a starting point for a process towards a more rigorous and congruent description of arthritis rehabilitation in studies. The framework was based on 3 existing models that are well recognized within the field of rehabilitation: Wade’s rehabilitation model (8, 21), ICF (25), and Donabedian’s healthcare model (22). The process has adopted a systematic and transparent approach, synthesizing evidence from 3 key sources: research evidence, clinical expertise and patient values (49). Table II provides an example of how the STAR-ETIC framework can be used.
| Table II. An example of how to use the The STAR-ETIC Framework.for describing a rehabilitation programme. STAR-ETIC: The Scandinavian Team Arthritis Register-European Team Initiative for Care Research |
| Domains and key elements | Description |
| Context | |
| Welfare and healthcare system | The country has a Nordic welfare model with universal healthcare, subsidized higher education, and a comprehensive social security system. |
| Structure | |
| Criteria for admittance and discharge | Only patients with an inflammatory disease that is confirmed by a rheumatologist are included in the programme. Rehabilitation in primary care should be considered not sufficient according to the rehabilitation needs. There are no specified criteria for discharge. |
| Funding | The rehabilitation programme is funded by the welfare system. |
| Clinical setting | Day care in a rheumatology hospital. |
| Rehabilitation team | Patient, rheumatologist (R), physiotherapist (PT), occupational therapist (OT), social worker (SW), psychologist (P) and nurse (N). |
| Rehabilitation management | At admittance, in cooperation with the team, each patient develop an individual plan for the rehabilitation period comprising goals, suggested interventions and cooperative agreements with the different team members. This provides the overall plan for the rehabilitation stay, and it is adjusted and evaluated by the patient and 1 of the team members, once a week. Team meetings (including the patient) are conducted at admittance and discharge. |
| Patient involvement | Patients are considered as the most important member of the rehabilitation team, and involved in the development, adjustment and evaluation of the rehabilitation plan. |
| Family involvement | Family members or essential others are invited to meet with relevant members of the team together with the patient. |
| Length of team care rehabilitation | 20 days over a 4-week period. The programme starts 09.00 h and ends at 15.00 h every day Monday to Friday. |
| Follow-up | All patients are invited to a follow-up meeting with the team 6 months after discharge. Other potential follow-up after discharge are individual and based on the individual goals of the rehabilitation plan. |
| Process | |
| Goals | Goals are individually developed according to each patient’s rehabilitation needs |
| Interventions | Each day begins with 45 min training in hot water supervised by a PT for all patients. According to the individual rehabilitation plan patients have individual appointments with PT, OT, SW, R, P or N before and after lunch. Three days a week from 14.00 h to 15.00 h patients can participate in a group exercise programme ending with 20 min of relaxation. |
| Assessment and evaluations (for clinical assessment) | All patients fill out Goal Attainment Scale (GAS) at arrival, discharge, and at the follow-up meeting 6 months later. R: General health status in an anamnesis including joint assessment. PT: Time Stands test, minor submax test, Shoulder arm function (Bostrom), Index of muscle function. OT: Gripit and Measure for activity performance of the hand (MAP). Canadian Occupational Performance Meassure (COPM). All assessments are made at inclusion and the R and the PT assessment are also repeated at discharge. N, SW and P get to know the patient by semi-structured clinical interviews at arrival. |
| Outcome (for research documentation) | |
| Body functions (International Classification of Function, Disability and Health (ICF)) | Numeric rating scale of pain, fatigue and disease activity. |
| Activity (ICF) | COPM, Modified Health Assessment Questionnire (Bath Ankylosing Spondylitis Functional Index for patients with Bekhterew). |
| Participation (ICF) | COPM |
| Health-related quality of life | Patient Global of Impression Scale and Short Form-36 |
| Self-management skills | The Brief Approach/Avoidance Questionnaire, Rheumatic Disease Illness Perception Questionnaire |
| Goal attainment | GAS |
| Patient satisfaction | Rehabilitation Patient Experience Questionnaire |
| Harms/adverse effects | Will be documented. |
| Cost | Will be documented. |
The framework was developed by a North European expert group, and with a North European rehabilitation practice as frame of reference. The selected domains and elements are very much in line with the detailed recommendations for rehabilitation that were published recently by the WHO and the World Bank in 2011 in the World Report on Disability (50). For example, similar to the STAR-ETIC framework, this report states that rehabilitation involves identification of a person’s problems and needs, relating the problems to relevant factors of the person and the environment, defining rehabilitation goals, planning and implementing the measures, and assessing the effects (50). The similarities between the STAR-ETIC framework and the WHO report strengthen the external validity of our proposed framework. The use of a standardized framework can help to describe cultural, geographical and socio-economic differences in arthritis rehabilitation across countries. In addition, the feasibility of the framework needs to be explored in developing countries with less resources and health infrastructures.
The initial literature search did not identify any frameworks for describing arthritis rehabilitation care. However, a framework for reporting on health service models for managing rheumatoid arthritis was published by a Canadian research group shortly after we finished the literature search (51). This framework was designed to cover all kinds of healthcare models, from inpatient care to telehealth. The Canadian research group proposed 6 underlying dimensions in their framework, all formulated as questions: (i) Why was it founded? (ii) Who was involved? (iii) What were the roles of those participating? (iv) When were the services provided? (v) Where were the services provided/received? (vi) How was the service/intervention assessed and implemented, how did the individuals involved communicate, and how was the model supported/sustained? (51). All these dimensions are covered in our framework; however, our framework provides a more detailed structure, as it was tailored for describing the content of complex rehabilitation interventions and highlights elements that are of particular importance in rehabilitation. Nevertheless, this does not undermine its potential as a useful framework for other groups of patients or programmes.
For health service research in general, there are some existing extensive classification frameworks, such as the System of Health Accounts (SHA) developed by the Organisation for Economic Co-operation and Development (OECD) (52), the Australian Classification of Health Interventions (ACHI) (12) and the WHO International Classification of Health Interventions (ICHI), which are in progress (11). These are all comprehensive tools for reporting and analysing the distribution and evolution of health interventions, and aim to cover a wide range of health-related care services. These tools are, however, generic for all types of healthcare and thus too extensive for brief descriptions in a clinical setting or for reporting of research results in journal formats.
Strengths and limitations
A major strength of this study is the development process of the framework, which was undertaken within a broad international group with representatives of clinicians, researchers, and patients. Although the Delphi rounds were carried out at the regular STAR-ETIC meetings, the reconciliations were still anonymous and open discussions were not arranged until the shift in the procedure in the eight step of the process. Anonymity is regarded as advantageous because it encourages opinions that are not influenced by peer pressure or other extrinsic factors (24). Furthermore, anonymous voting is important to diminish influence of a potential hierarchical structure between the participants, thereby ensuring that everyone has the same influence on the final framework regardless of their education, profession or professional reputation. A downside of anonymity is that it may also lead to a lack of accountability. However, this can be minimized if individuals are recruited because of their expertise, as was the case in the current process (53). In the final phase of the development process, a change from an anonymous Delphi procedure to a more open Nominal group technique was introduced. This shift was essential to allow the participants to see the framework as a whole and reach a final consensus. The pre-piloting of the framework before the Nominal group discussions and final consensus votes was also very useful to ensure that the final framework was valid and feasible.
The decision to base the framework on a draft model, based on Wade’s rehabilitation model (8, 21), ICF (25) and Donabedian’s structure, process and outcome model (54), helped us to maintain a logical structure for categorizing important elements under the 3 domains (structure, process and outcome). Other authors have argued that descriptions of context are crucial, not only when designing interventions, but also to be able to assess to what degree an intervention that was effective in one setting may work in another setting (7, 55). The introduction of context as a fourth domain was debated, and unanimously agreed upon in the group. It can be argued that our definition of context is superficial and could have been more specific in order to distinguish the context of health systems from the setting of care provisions. One way to do this could have been to use the triad of macro (policy and financing), meso (healthcare organization and community) and micro (patient and family) levels of the healthcare system, which is outlined in the WHO Innovative Care for Chronic Conditions Framework (56). On the other hand, it can be argued that this distinction of macro, meso and micro levels are already covered within our framework. The “macro” level very much overlaps with our “context” domain, the “meso” with our “structure”, and the “micro” with our “process” domains, respectively. Future studies could explore this topic further.
The number of elements included in the 4 domains in the framework was not predetermined, and the initial brainstorming process and the search for elements in the reviewed literature did not bring forward many new elements. The predefined mathematical procedure for including or excluding elements after the 2nd and 3rd Delphi round forced participants to exclude elements that a majority had initially ranked as important or very important. It was necessary to reduce the number in this way to ensure feasibility in terms of a framework with a manageable number of elements.
Two limitations of our study are that nurses, psychologists and social workers are not represented in the STAR-ETIC group, and that the panel only included members from the northern part of Europe. Including experts from other professions and other parts of the world might have affected the outcome. Concerning the second limitation, the huge differences in healthcare systems and rehabilitation traditions would, however, probably have made it more difficult to reach consensus. To ensure external validity, the new framework should be tested in different cultural settings, and in teams encompassing many different professions.
One important lesson learned in the process was the importance of ensuring that the different health professionals and patient representatives have the same understanding of the concepts used to describe potential dimensions and elements in the framework. The process might have been easier and less time-consuming if all the concepts and elements proposed had been defined in the initial phase.
An important next step is to validate the framework by using it in different rehabilitation settings in different countries, and thereafter develop evidence-based quality criteria related to each element in the framework. Development of quality criteria can further serve as a basis for developing clinical guidelines, which is recognized as an important action to reduce barriers to rehabilitation worldwide (50).
In conclusion, the STAR-ETIC framework designates the most important domains and elements for describing arthritis rehabilitation. The framework is designed to be used both in clinical practice and in research. A common framework may enhance comparisons of rehabilitation programmes across countries and national levels of care.
Acknowledgements
The STAR-ETIC project is financially supported by the European League Against Rheumatism (EULAR).
The authors would like to thank Ingegerd Wickström, Britta Strömbeck, Sofia Hagel, Birgitta Smedeby, Elisabeth Lindquist, Inger Henriette Stovgaard, Susanne Jürgensen, Connie Ziegler, Jorit J. Meesters, and Gerd Jenny Aanerud for contributing in the Delphi process, and librarian Hilde Iren Flaatten at Diakonhjemmet Hospital for performing the literature search.
References