Martin Nuhr, MD1, Veronika Fialka-Moser, MD1, Mohammad Keilani, MD1, Richard Crevenna, MD1 and Michael M. Hirschl, MD2
From the 1Department of Physical and Rehabilitative Medicine, Medical University of Vienna, Vienna and 2Department of Internal Medicine, Landesklinikum Zwettl, Zwettl, Austria
OBJECTIVE: Arterial hypertension is the most frequently observed vascular risk factor. Physical and rehabilitative interventions may affect arterial blood pressure. The frequency of hypertensive patients in an outpatient clinic of physical medicine is unknown.
DESIGN: Prospective data collection.
Patients: Overall, 3,826 patients admitted to the outpatient clinic for physical and rehabilitative interventions were included to assess arterial blood pressure, additional vascular risk factors, history of cardiovascular events and antihypertensive drug treatment.
METHODS: Arterial blood pressure was measured using an oscillometric method on the non-dominant arm. The patients were divided into sufficiently treated (< 140/90 mmHg, drug treatment), insufficiently treated (≥ 140/90 mmHg, drug treatment and history of hypertension) or de novo hypertensive patients (≥ 140/90 mmHg, no history of hypertension).
RESULTS: Arterial hypertension was observed in 48% of all patients (n = 1,840). In 719 (19%) of patients blood pressure above normal values. Due to significant hypertension 189 (5.2%) patients were either not permitted to start treatment or had to interrupt their physical treatment.
CONCLUSION: Insufficiently treated hypertension or previously undiagnosed hypertension is relatively common in a physical medicine clinic. We therefore recommend the implementation of arterial blood pressure measurement into the admission procedures in order to reduce such events.
Key words: arterial hypertension; physical medicine; rehabilitative intervention.
J Rehabil Med 2012; 44: 436–439
Correspondence address: Michael M. Hirschl, Department of Internal Medicine, Landesklinikum Waldviertel Zwettl, Propstei 5, AT-3910 Zwettl, Austria. E-mail: michael.hirschl@zwettl.lknoe.at
Submitted July 5, 2011; accepted January 4, 2012
INTRODUCTION
In Austria, the speciality of physical medicine and rehabilitation offers a wide spectrum of passive physical modalities and active therapeutic approaches, such as physiotherapy, immersion and medical exercise treatment options. Arterial hypertension is the most frequently observed single vascular risk factor in the countries of Western Europe and the USA (1, 2). It is responsible for the development of stroke, acute myocardial infarction, renal insufficiency and peripheral arterial disease (3, 4). Patients admitted to an outpatient clinic of physical medicine and rehabilitation receive multiple and different therapeutic treatments, which may affect arterial blood pressure (5, 6). There are a few reports demonstrating a significant short-term change in arterial blood pressure after physical and rehabilitative interventions (7, 8). Therefore, knowledge of the current blood pressure situation of patients prior to physical and rehabilitative treatment seems to be of clinical relevance. However, no data are available about the percentage of patients with arterial hypertension either treated or untreated admitted to an outpatient clinic of physical medicine and rehabilitation. The aim of this prospectively designed study was to screen patients admitted to an outpatient clinic of physical medicine and rehabilitation for evidence of arterial hypertension either treated or untreated.
METHODS
Study design
In this prospective study 3,826 patients admitted to an outpatient clinic of physical medicine and rehabilitation over an 18-month period were included. Data collection was performed between 1 February 2009 and 31 August 2010. All patients were informed about the anonymous use of their data for scientific reasons and gave their verbal consent prior to data collection. The study was without approval by a research ethics committee, as routine blood pressure measurement is a clinical activity with negligible risk for the participant.
Study setting and population
Patients with musculoskeletal disorders, mainly with a diagnosis of low back pain with or without lumbar or cervical disc surgery, and patients with moderate to severe arthrosis or after knee or hip replacement attended the outpatient clinic to undergo an intensive rehabilitation programme. After admission to the outpatient clinic the medical history of the patient was evaluated by a physician. The following demographic and clinical data were assessed: age, gender, body mass index (BMI), evidence of hypercholesterolaemia, diabetes mellitus, current smoking and history of arterial hypertension. In addition, a medical history of stroke or myocardial infarction was evaluated. After evaluating medical history blood pressure measurement was performed.
Blood pressure measurement
The measurement was performed in a quiet room with a constant room temperature (22ºC). The patient was told to rest for 15 min in a sitting position prior to blood pressure measurement. The measurement was taken by a trained nurse using an oscillometric method on the non-dominant arm of the patient (Fa. OMRON, MIT-Elite Plus, LR Hoofddorp, The Netherlands). Three measurements were performed every 5 min. The values of the 2nd and 3rd measurement were added and a mean value was calculated. The measurements were repeated on the 2nd and 3rd day after admission. The mean of the values assessed on 3 consecutive days was used for further classification. Patients with a blood pressure below 140/90 mmHg were either classified as normotensive individuals (no antihypertensive drug treatment and no history of arterial hypertension) or sufficiently treated hypertensive individuals (current antihypertensive treatment). In the case of blood pressure values above 140/90 mmHg, the measurement of blood pressure was repeated on the subsequent 2 days. If the mean value of blood pressure remained above 140/90 mmHg patients were classified as de novo hypertensives, if no history of arterial hypertension and lack of antihypertensive treatment were evident. Insufficiently or non-treated hypertensives were defined as patients with a history of arterial hypertension with or without antihypertensive drug treatment. Patients with an initial blood pressure > 180/100 mmHg were not permitted to start physical treatment. Insufficiently treated hypertensive or de novo hypertensive patients with an initial systolic blood pressure between 141 mmHg and 180 mmHg and/or diastolic blood pressure between 81 and 100 mmHg were allowed to start treatment. In these patients blood pressure was measured after physical treatments, which are potentially associated with an increase in blood pressure (water immersion, physiotherapy). If blood pressure was increased above 180/90 mmHg after these interventions discontinuation of treatment was recommended.
End-points
The primary parameter was the prevalence of patients with arterial hypertension in a population of an outpatient clinic of physical medicine and rehabilitation. Secondary parameters included the number of hypertensive patients who were insufficiently treated or previously undiagnosed. Further parameters were the absolute blood pressure values in each group, the frequency of concomitant risk factors and the number of patients with severe arterial hypertension who were not permitted to start therapy and those interrupting their physical treatment due to severe blood pressure elevation during or after treatment.
Data collection and analysis
The patients were divided into 4 groups: normotensives, sufficiently treated hypertensives, insufficiently treated hypertensives and de novo hypertensives. The patient characteristics and the blood pressure values were compared using χ2 statistics for categorical variables and the Mann-Whitney U test for continuous variables. Analysis was performed using the Statistical Package for Social Sciences, version 13.0 (SPSS, Chicago, IL, USA). The level of significance was determined as p < 0.05.
RESULTS
General characteristics
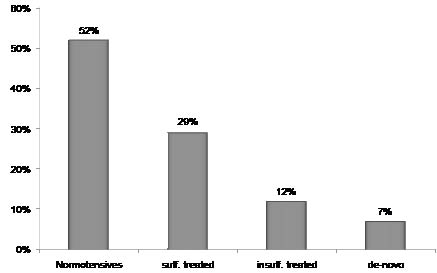
A total of 3,826 patients (1986 females, mean age 61 (standard deviation; SD 15) years) were consecutively screened for the evidence of arterial hypertension. Fig. 1 shows the distribution of patients according to the 4 predefined groups. Forty-eight percent of all patients were defined as hypertensive patients. Out of these 1,840 patients blood pressure values were above normal values in 719 patients. A total of 264 patients had no knowledge of the evidence of arterial hypertension.
Fig. 1. Percentage of patients in each group (normotensive, sufficiently treated hypertensives, insufficiently treated hypertensives and de novo hypertensives) according to blood pressure measurement.
General characteristics and concomitant risk factors
Table I illustrates the characteristics of the 4 predefined groups. Patients with arterial hypertension were significantly older independent of the efficacy of antihypertensive treatment and exhibited a higher BMI compared with normotensive people. The frequency of diabetes mellitus was two-fold higher than in normotensives (p < 0.0001). Patients with newly detected hypertension differed from normotensive patients with regard to the percentage of males (58% vs 46%). In addition, these patients were older (62 years (SD 13) vs 55 years (SD 14)) and exhibited a higher BMI (28.6 (SD 4.8) vs 26.5 (SD 4.3)).
| Table I. General characteristics and concomitant risk factors in the 4 groups of patients (n = 3,826) |
| | Normotensive | Sufficiently treated | Insufficiently treated | De novo |
| Total, n | 1,986 (52) | 1,121 (29) | 455 (12) | 264 (7) |
| Age, year, mean (SD) | 55 (14) | 68 (11) | 68 (11) | 62 (13) |
| BMI, mean (SD) | 26.5 (4.3) | 29.3 (4.6)** | 30.4 (5.2)** | 28.6 (4.8) |
| Males, n (%) | 922 (46) | 552 (49) | 229 (50) | 155 (59)* |
| Diabetes mellitus, n (%) | 44 (2) | 124 (11)** | 63 (14)** | 9 (4) |
| Hyperlipidaemia | 222 (11) | 141 (12) | 56 (12) | 25 (9) |
| Current smoker | 343 (17) | 105 (9)*** | 37 (8)*** | 39 (15) |
| *p = 0.0017 (normotensives vs de novo hypertensives). **p < 0.0001 (normotensives vs sufficiently or insufficiently treated hypertensives). ***p < 0.001 (normotensives vs sufficiently or insufficiently treated hypertensives). BMI: body mass index; SD: standard deviation. |
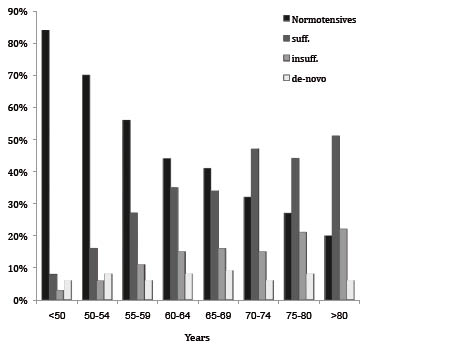
Analysing the distribution of patients in each age group, the percentage of patients with known arterial hypertension increased with age. In the group of patients with de novo hypertension no such correlation was noted (Fig. 2). The BMI was significantly higher in all groups of hypertensive patients compared with normotensive individuals.
Fig. 2. Percentage of patients of each group with regard to age.
Blood pressure values
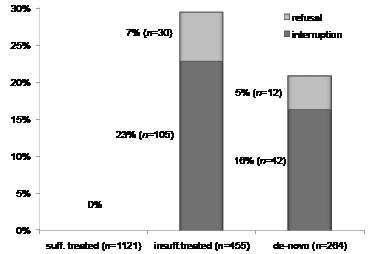
Table II summarizes the mean systolic and diastolic blood pressure values according to the 4 groups. Blood pressure was significantly more elevated in patients with insufficiently treated hypertension or in patients with unknown hypertension compared with normotensives or patients with sufficiently treated arterial hypertension. Forty-two out of 1840 (2.3%) hypertensive patients were not permitted to start physical treatment. The treatment had to be interrupted in 147 (8.2%) patients due to severe blood pressure elevation mainly after the physical treatment. All of these patients belonged to the group of insufficiently treated or de novo hypertensive patients. Fig. 3 illustrates the percentage of these patients with regard to their initial blood pressure.
| Table II. Blood pressure values (systolic and diastolic) in patients admitted to an outpatient clinic of physical medicine and rehabilitation (n = 3,826) |
| | Normotensive | Sufficiently treated | Insufficiently treated | De novo |
| Total, n | 1,986 | 1,121 | 455 | 264 |
| Systolic BP, mmHg, mean (SD) | 122 (10) | 128 (8) *** | 155 (13)*, ** | 153 (12)*, ** |
| Diastolic BD, mmHg, mean (SD) | 77 (7) | 79 (6) *** | 89 (10)*, ** | 93 (15)*, ** |
| *p < 0.0001 (normotensives vs insufficiently treated hypertensives or de novo hypertensives). **p < 0.0001 (sufficiently treated hypertensives vs insufficiently treated hypertensives or de novo hypertensives). *** p < 0.001 (normotensives vs sufficiently treated hypertensives). BP: blood pressure; SD: standard deviation. |
Fig. 3. Percentage of patients who had to be refused therapy or had to interrupt treatment due to their initial blood pressure.
DISCUSSION
This is the first study to investigate the frequency of arterial hypertension in patients admitted to an outpatient clinic of physical medicine and rehabilitation. The number of patients with unknown hypertension or insufficiently treated arterial hypertension is of clinical relevance, as 19% of all patients belonged to these groups. Our knowledge of the short-term effect of physical and rehabilitative treatment modalities on arterial blood pressure is limited. Some data are available about the effect of water immersion on blood pressure and cardiac output (9, 10). Whereas hot water immersion leads to a decrease in blood pressure, cold water immersion causes a significant increase in blood pressure due to peripheral vasoconstriction (11). A previous publication demonstrated that even immersion at 33ºC induced a small, but significant, increase in noradrenaline (12). Another study confirmed this finding by demonstrating significant increase in noradrenaline due to moderate to cold water temperatures (5). Arterial hypertension is based on increased peripheral vasoconstriction mediated by noradrenaline. It is therefore very likely that physical interventions associated with an increase in noradrenaline in healthy subjects may have negative effects in hypertensive patients. Considering our data it may be assumed that the risk for insufficiently treated hypertensive patients to develop severe hypertension may increase after physical interventions, for example, water immersion with cold to normal temperature levels.
Early detection of elevated blood pressure may lead to an intensified antihypertensive drug treatment to achieve sufficient blood pressure control prior to the start of rehabilitative interventions. After a sufficient control of blood pressure the risk of interrupting treatment is negligible, as none of the patients with sufficiently controlled blood pressure had any complications during or after treatment. Despite these immediate favourable effects on the rehabilitative programme the public health aspect of measuring blood pressure has to be emphasized. A considerable number of patients, i.e. 7% of the overall study population, were identified as hypertensive patients. The detection of arterial hypertension at this stage and consequent early start with medical interventions may prevent the development of serious complications, such as myocardial infarction and stroke.
We are aware that measurement of blood pressure on admission has not been usually performed routinely in the outpatient clinic of physical and rehabilitative medicine. Therefore it may be reasonable to search for easily available markers, which may help to identify these patients on admission to the outpatient clinic. In general, the frequency of arterial hypertension increased with age. This finding is in line with epidemiological data demonstrating a correlation between increasing age and occurrence of arterial hypertension (13). However, the use of an age-related cut-off to identify patients with a higher risk for arterial hypertension cannot be justified by our data, as especially patients with unknown or de novo hypertension are equally distributed over the different age classes. A considerable percentage of these patients would not be detected if only those patients over a predefined cut-off undergo blood pressure measurement (Fig. 2). The other obvious distinction between normotensive individuals and hypertensive patients is the mean BMI, which was significantly higher in hypertensive patients. Increased BMI is an independent risk factor for the development of arterial hypertension (14). The probability of detection of arterial hypertension will increase with higher BMI. However, patients with unknown hypertension, in particular, showed wide variability with regard to the BMI.
In summary, arterial blood pressure measurement should be requested as an unconditional procedure prior to the start of a rehabilitation programme. Early detection of hypertensive patients prior to physical and rehabilitative interventions may prevent the interruption of treatment and of cardiovascular complications due to blood pressure elevation. Moreover, arterial blood pressure measurement meets the criteria of a preventive procedure, as antihypertensive treatment of insufficiently treated hypertensive patients can be successfully modified and de novo hypertensive patients can be referred to further diagnostic and therapeutic procedures.
Study limitations
One limitation of this study is the use of office blood pressure measurements, as occasional blood pressure measurements are higher than the “true” blood pressure level in approximately 20% of all patients. Using 3 measurements within 15 min on 3 consecutive days should minimize the risk of incorrect classification of individuals according to their blood pressure. In addition, most of the studies dealing with the effect of antihypertensive drug treatment have used a similar procedure to assess blood pressure. The possible increase in blood pressure during various physical and rehabilitative interventions remains speculative, as continuous blood pressure measurement during such interventions has not been carried out. However, according to previously published data the probability of blood pressure increase during physical interventions is high, as the release of noradrenaline, which is a potent vasoconstrictor, has been determined. Our data demonstrate that a considerable percentage of patients exhibit severe blood pressure elevation after specific physical treatment, leading to discontinuation of treatment. In addition, blood pressure measurement on admission to a physical and rehabilitative outpatient clinic must be seen as an important preventive strategy, as patients with insufficiently treated or de novo hypertension can easily be identified.
ACKNOWLEDGEMENT
This study was supported by an unrestricted grant of Takeda Pharma Austria.
REFERENCES