Sharon Hakkennes, BPhty1,2, Keith D. Hill, PhD3,4, Kim Brock, PhD5, Julie Bernhardt, PhD6 and Leonid Churilov, PhD6,7
From the 1School of Physiotherapy, Faculty of Health Sciences, La Trobe University, Melbourne, 2Barwon Health, Geelong, 3School of Physiotherapy, Curtin University, Perth, 4Preventive and Public Health Division, National Ageing Research Institute, Parkville, 5St Vincent’s Hospital, Melbourne, 6National Stroke Research Institute, Florey Neuroscience Institutes, Heidelberg, Victoria and 7Department of Mathematics and Statistics, The University of Melbourne, Victoria, Australia
OBJECTIVES: This study aimed to identify factors that assessors considered important in decision-making regarding suitability for inpatient rehabilitation after acute severe stroke.
DESIGN: Multi-site prospective observational cohort study.
SUBJECTS: Consecutive acute, severe stroke patients and their assessors for inpatient rehabilitation.
METHODS: Rehabilitation assessors completed a questionnaire, rating the importance (10 point visual analogue scale) and direction (positive, negative or neutral) of 15 patient related and 2 organisational items potentially affecting their decision regarding patients’ acceptance to rehabilitation.
RESULTS: Of the 75 patients referred to rehabilitation and included in this study 61 (81.3%) were accepted for inpatient rehabilitation. The items considered to be most important in the decision to accept the patient for rehabilitation were pre-morbid cognition, pre-morbid mobility and pre-morbid communication. For those not accepted the most important items were current mobility, social support and current cognition. Factor analysis revealed 3 underlying factors, interpreted as post-stroke status, pre-morbid status, and social attributes, accounting for 61.8% of the total variance. All were independently associated with acceptance for rehabilitation (p < 0.05).
CONCLUSIONS: This study highlights the importance of pre-morbid function and social factors in addition to post-stroke function in the decision making process for acceptance to rehabilitation following severe stroke. Future models for selection for rehabilitation should consider inclusion of these factors.
Key words: stroke; rehabilitation; patient selection; health services accessibility.
J Rehabil Med 2013; 45: 00–00
Guarantor’s address: Sharon Hakkennes, Faculty of Health Sciences, School of Physiotherapy, La Trobe University, Bundoora VIC 3086, Australia. E-mail: sharonh@barwonhealth.org.au
Submitted January 26, 2012; accepted August 10, 2012
Introduction
Stroke is a leading cause of disability in adults, with an estimated 60,000 stroke events occurring in Australia each year (1). Of the survivors, approximately one third display severe impairments (2–4).
Rehabilitation following stroke aims to support patients to regain independence in daily function and maximise participation in the community (5). Hospital-based rehabilitation following acute stroke improves outcomes (6, 7), with patients with severe stroke appearing to benefit most (5, 6, 8). Canadian best practice recommendations for stroke care recommend that patients should be given an opportunity to participate in inpatient rehabilitation following moderate to severe stroke if they have rehabilitation goals and are rehabilitation ready (9).
Determining who will benefit from inpatient rehabilitation can be difficult. Excluding patients who would have benefited from inpatient rehabilitation may impact on the patient’s functional achievements and ultimate post discharge living situation (10). Conversely, accepting patients who do not benefit from inpatient rehabilitation could be considered a misuse of scarce health care resources.
This difficulty of determining suitability for rehabilitation for severe stroke patients is reflected in the literature, with previous studies demonstrating considerable variation in stroke management, access to stroke rehabilitation and outcome (11, 12), particularly for patients following severe stroke (4). Thus, whilst the evidence supports inpatient rehabilitation following severe stroke there is variation in practice with regards to access.
Recently a systematic review investigated factors considered important in decision making when assessing a patient for rehabilitation following acute stroke (13). Three aspects of the decision for acceptance for rehabilitation were investigated: (i) prognostic factors of final functional level, (ii) acute and final discharge disposition, and (iii) rehabilitation selection criteria. Although the methodological quality of the included studies was generally poor, age, cognition, functional level following stroke and continence were found to have an association with outcome across the 3 research areas investigated. In addition stroke severity was also associated with acute discharge disposition, final discharge disposition and functional level. Gender and side of stroke appeared to have no association across the 3 research areas investigated. None of the included studies or reviews assessed the effect of patient factors such as motivation and goals on functional outcome and/or acute and final discharge disposition, nor did they specifically assess the decision-making process surrounding rehabilitation acceptance. More recently, as a part of this study and reported previously (14), we found younger age (odds ratio (OR) = 0.89, 95% confidence interval (CI) = 0.83–0.95, p = 0.001), independent pre-morbid functional status (OR = 14.92, 95% CI = 2.43–91.60, p = 0.004), and higher level of current mobility (OR = 1.31, 95% CI = 1.02–1.66, p < 0.03) to be independently associated with discharge to rehabilitation for patients with acute severe stroke. In addition, in this study 12% of total variability in discharge destination was explained by differences between the hospital units (rho = 0.12, 95% CI = 0.02–0.55, p = 0.048). This indicates that there is variation in practice with regards to access to inpatient rehabilitation for this patient group.
There has been one previous study that has documented clinical and non-clinical factors influencing admission to rehabilitation following stroke for 6 European stroke rehabilitation units (across 4 countries). Medical consultants rated the importance of 25 patient-related and 12 organisational factors in influencing admission to their stroke rehabilitation unit. Factors that were identified as highly important were explored further through semi-structured interviews. Whilst there were many differences across the units, results indicated that, in addition to the presence of social support, pre-morbid function and cognition were important influences, but the severity of functional deficits post-stroke was not. Several organisational factors including insurance status and affiliations between the rehabilitation unit and referring hospital were also identified as being important (11). Whilst this study highlights the complexity of the decision-making process regarding selection for rehabilitation following stroke, the observations were general in nature (rather than related to specific patients) and there was no statistical analysis of the results conducted.
In order to facilitate discussion regarding improving equity of access to rehabilitation following severe stroke, a thorough understanding of not only known prognostic indicators but also the rehabilitation assessors’ decision-making process is required. Therefore, the aim of this study was to identify factors that the assessors considered were important in making the decision regarding suitability of severe stroke patients in the acute hospital for inpatient rehabilitation.
Methods
This was a multi-site prospective observational cohort study of consecutive severe stroke patients admitted to 5 acute hospitals in Victoria, Australia. Participating sites included 4 tertiary referral metropolitan hospitals and 1 large regional hospital, all with access to a specialised stroke service and admitting greater than 300 stroke patients per year.
The participants in this study were clinicians responsible for assessing the suitability of patients for inpatient rehabilitation at the participating hospitals. No restrictions were imposed with regards to qualifications or experience. The clinicians reported the relative importance of items contributing to their decision to accept or not accept individual patients referred for rehabilitation during the study period.
Rehabilitation assessments were included in the study for all patients referred for rehabilitation following an acute, severe (Mobility Scale for Acute Stroke (MSAS) scores ≤ 15), ischaemic or haemorrhagic stroke (4). The MSAS is used to rate ability to perform 6 tasks (bridging, sitting from supine, balanced sitting, sit to stand, standing and gait), and uses a 6-point scale from 1 (unable to perform) to 6 (independent). The MSAS has been shown to be a reliable and valid measure of mobility for use in the first few weeks following acute stroke (15, 16) and can be scored by the physiotherapist while delivering routine assessment and intervention in the acute phase of stroke.
Patients were excluded if they were admitted to the acute hospital from residential care (high level), the onset of stroke was more than 3 days prior to admission, they were in intensive care or for palliative care on day 3 following stroke and/or they were admitted with another primary illness or incident, where stroke was not the main cause of disability.
The trial physiotherapist screened consecutive patients admitted with a primary diagnosis of stroke for inclusion at day 3 (day of stroke was considered to be day 0). Where day 3 fell on a weekend, information was collected at day 4 or 5. At this time the physiotherapist also assessed the patient and completed the physiotherapy data collection form. This included demographic information and information relating to the patient’s pre-morbid status, social status and post-stroke status.
Patient comorbidity was measured using the Charlson Index, which has been demonstrated to be both a reliable and valid method to measure comorbidity (17). Scores were dichotomised according to low comorbidity (0 or 1) and high comorbidity (≥ 2) (18).
The patient’s pre-stroke disability was measured using the modified Rankin Scale (mRS). The mRS rates disability on a 7-point scale between 0, no symptoms and 6, death. The mRs has been shown to be a reliable and valid method of measuring global disability (19). Scores were dichotomised into independent (0–2) and requiring assistance (> 2) (20).
Information relating to the patient’s cognitive and communicative status was collected using the National Institutes of Health Stroke Scale (NIHSS), a reliable and valid measure of post stroke disability (21, 22). Cognition was scored using the level of consciousness, response to questions and response to commands items and communication was scored using the best language and dysarthria items. Scores for each domain were summed. Therefore possible range of scores for cognition was 0–7 and for communication the score range was 0–5, with higher scores indicating a higher level of disability.
Continence was assessed using the bladder and bowel items of the Barthel Index (BI) (23). The reliability of the BI has previously been demonstrated, including its use by physiotherapists (24, 25).
The trial physiotherapist also collected details of the patient’s discharge destination.
A questionnaire was used to measure the factors influencing the rehabilitation assessors’ decision making regarding suitability for rehabilitation, the main outcome of interest. The rehabilitation assessor, immediately following the patient review and decision regarding rehabilitation suitability, completed the questionnaire. In instances where the patient was reviewed more than once before a final decision was made regarding rehabilitation suitability, the questionnaire was completed following the assessment at which the suitability for rehabilitation decision was made. Therefore, only one rehabilitation assessor questionnaire was completed for each patient. The assessor did not have access to the study data collected by the physiotherapist.
Items included in the assessor questionnaire were derived from a comprehensive review of the literature aiming to not only identify important prognostic indicators but also social and organisational factors that may affect rehabilitation admission/outcome (5, 10, 13, 26–29). As this was the first study of its kind, to minimise the risk of missing confounding items the number of probable relevant variables were not restricted (30) and assessors were given the opportunity to identify additional relevant items.
Fifteen patient-related items (age, pre-morbid mobility, pre-morbid cognitive status, pre-morbid communicative status, pre-morbid living situation, current mobility, current cognitive status, current communicative status, current continence status, patient’s mood, patient’s motivation, patient/carer goals, patient’s insight, social support and patient/carer advocating for rehabilitation) and two organisational items (bed availability and funding source) were included in the rehabilitation assessor questionnaire. The questionnaire was paper-based and asked the rehabilitation assessor to rate, in their opinion, the importance on a 10 point visual analogue scale (0, not at all important; 10, very important), how much each item influenced their decision regarding suitability for inpatient rehabilitation, and then indicate if this factor was positive (i.e. increased likelihood of accepting patient), negative (reduced likelihood of accepting patient) or neutral. (A copy of the rehabilitation assessor questionnaire can be obtained from the first author on request.)
In addition, demographic information of the stroke rehabilitation assessors’ qualifications, number of years experience in rehabilitation assessment and approximate number of rehabilitation assessments completed each week was obtained at the time of rehabilitation assessor consent.
Approval was obtained from the ethics committees at La Trobe University and each of the 5 participating sites. Written informed consent was obtained from rehabilitation assessors. As all patient data were collected as a part of routine care, and identifying information was removed from all data collection sheets prior to submission to the research team for data analysis, informed consent from patients was not required.
Analysis
Statistical analysis was conducted using SPSS for Windows version 19.0 and Stata 11. For all analysis, the threshold for statistical significance was set at p = 0.05. Normality of continuous data was assessed both visually and formally using the Shapiro-Wilk Test and, as a result, univariate comparisons for continuous were conducted using the Mann-Whitney U test and the Hodges–Lehmann estimator (with 95% CI) was used to measure effect size. The Fisher’s Exact test and the risk difference (RD) (with 95% CI) was used for univariate comparisons of categorical data.
Descriptive statistics were used to summarise demographic information relating to the rehabilitation assessors and patient profile. To assess for differences between patients accepted and not accepted for rehabilitation, categorical patient demographic and clinical presentation data was compared. Differences in absolute importance of each of the 17 items measured on the rehabilitation questionnaire between participants in the study who were accepted for rehabilitation and those not accepted for rehabilitation were analysed for each item. Item scores were calculated based on the position marked on the visual analogue scale, with a possible score range (to the nearest mm) of 0 to 10.
To enable analysis with relation to the direction in addition to the importance of the items, rehabilitation assessor ratings were transformed based on the direction of their importance. Negative ratings were converted to negative scores, and neutral scores were converted to 0 as, by definition, they neither increased nor decreased the likelihood of acceptance to rehabilitation. Thus scores were converted to represent a continuum of –10 (strong negative influence) to 10 (strong positive influence).
Factor Analysis with Principal Component extraction was used to extract factors from the transformed scores of 15 patient related items, thereby reducing the large number of inter-correlated rehabilitation assessor items. The Kaiser-Meyer-Olkin Measure of Sampling Adequacy was assessed to determine whether use of factor analysis was appropriate (31). Factors with eigenvalues greater than or equal to 1 (confirmed through the scree plot) were retained. Varimax rotation with Kaiser Normalization was used. Items were grouped together in a factor if they loaded higher than 0.4 on that factor and the individual factor scores were calculated using regression approach (32). Percentage of variance explained was reported for each factor individually, and for the overall analysis. Calculated factor scores were subsequently used in a multiple logistic regression analysis to estimate the adjusted odds ratio of acceptance to rehabilitation for each of the factors.
As the analysis was based on the 15 patient-related items, using the 5 subjects-per-item ratio heuristic (33), the minimal adequate sample size for factor analysis was set at 75 patients.
Results
Data collection occurred between June 2010 and September 2011. A total of 117 patients met the study inclusion criteria, 86 (73.5%) were referred for a rehabilitation assessment and 61 (52%) were discharged to rehabilitation. The rehabilitation assessor failed to complete the questionnaire in 11 (12.8%) of these patients. Therefore, a total of 75 patients were included in this study. There was no evidence of systematic selection bias, with no significant differences on any of the demographic or clinical presentation information between those patients included and those patients where the assessor questionnaire was missing.
Fourteen rehabilitation assessors participated in the study. The median number of rehabilitation assessors per site was 3 (range 1–5). Assessors were mostly rehabilitation consultants (43%) or rehabilitation registrars (36%) with the remainder (21%) being geriatricians. The number of years experience in rehabilitation assessment ranged between less than one year to greater than 10 years, with more than one quarter (29%) having less than one year of experience. Over two thirds (69%) of the assessors conducted more than 5 rehabilitation assessments per week.
Of the 75 patients included in the analysis, 61 (81.3%) were accepted for rehabilitation. The median age of the included patients was 76.5 years (interquartile range (IQR) = 66.0–83.0), 38 (50.7%) were male and 59 (78.8%) had an infarct. Those accepted for rehabilitation were significantly younger (difference = –8 years (95% CI –13 to –3), p = 0.004), more likely to be independent in functional activities (difference = –0.21 (95% CI –0.03 to –0.48), p = 0.04), more likely to be living at home with support (p = 0.04) and more likely to be employed (RD = 0.26 (95% CI 0.15 to 0.37), p = 0.03) when compared to those not accepted. In addition, total length of stay was significantly longer for those not accepted for rehabilitation (difference = –13.5 (95% CI –20 to –3), p = 0.005). Table I details demographic and clinical presentation information of the included patients.
|
Table I. Patient demographic and clinical characteristics |
|||||
|
Accepted n = 61 |
Not accepted n = 14 |
Difference (95% CI)a |
p-valueb |
||
|
Age years, median (IQR) |
73.0c (64.5, 82.0) |
83.5 (80.0, 85.0) |
–8 (–13 to –3) |
0.004 |
|
|
Sex, n (%) |
|||||
|
Male |
33 (54.1) |
5 (35.7) |
–0.18 (–0.46 to 0.10) |
0.249 |
|
|
Female |
28 (45.9) |
9 (64.3) |
|||
|
Type of stroke, n (%) |
|||||
|
Infarct |
50 (82.0) |
9 (64.3) |
–0.17 (–0.45 to 0.09) |
0.161 |
|
|
Haemorrhage |
11 (18.6) |
5 (35.7) |
|||
|
Side of hemiparesis, n (%) |
|||||
|
Left |
28 (45.9) |
3 (21.4) |
N/A |
0.067 |
|
|
Right |
33 (54.1) |
10 (71.4) |
|||
|
Bilateral |
0 (0.0) |
1 (7.1) |
|||
|
Charlson Comorbidity Index, n (%) |
|||||
|
0–1 |
47 (77.0) |
9 (64.3) |
–0.13 (–0.40 to 0.14) |
0.326 |
|
|
> 1 |
14 (23.0) |
5 (35.7) |
|||
|
Pre-stroke functional level (mRS), n (%) |
|||||
|
0–2 |
56 (93.3) |
10 (71.4) |
–0.21 (–0.03 to –0.48) |
0.037 |
|
|
> 2 |
4 (6.7) |
4 (28.6) |
|||
|
Pre-stroke living arrangement, n (%) |
|||||
|
Home alone |
8 (13.1) |
4 (28.6) |
N/A |
0.041 |
|
|
Home with others |
51 (83.6) |
8 (57.1) |
|||
|
Supported accommodation |
2 (3.3) |
2 (14.3) |
|||
|
Primary language, n (%) |
|||||
|
English |
39 (63.9) |
10 (71.4) |
–0.75 (–0.34 to 0.19) |
0.759 |
|
|
Other |
22 (36.1) |
4 (28.6) |
|||
|
Employment status, n (%) |
|||||
|
Full-time/Part-time employment |
16 (26.2) |
0 (0.0) |
0.26 (0.15 to 0.37) |
0.032 |
|
|
Not working/retired |
45 (73.8) |
14 (100) |
|||
|
Insurance status, n (%) |
|||||
|
No insurance |
47 (77.0) |
10 (71.4) |
–0.06 (–0.32 to 0.20) |
0.731 |
|
|
Private/Veterans Affairs |
14 (23.0) |
4 (28.6) |
|||
|
Availability of carer on discharge, n (%) |
|||||
|
None |
15 (24.6) |
5 (35.7) |
N/A |
0.487 |
|
|
Supervision |
18 (29.5) |
5 (35.7) |
|||
|
Physical Assist |
28 (45.9) |
4 (28.6) |
|||
|
Cognition, median (IQR) |
2 (0.0, 4.0)d |
2.5 (1.0, 4.0) |
0 (–2 to 1) |
0.465 |
|
|
Communication, median (IQR) |
1 (1.0, 3.0)e |
2 (1.0, 2.0) |
0 (–1 to 1) |
0.220 |
|
|
Continence – bladder, n (%) |
|||||
|
Incontinent/catheter |
33 (54.1) |
11 (78.6) |
N/A |
0.291 |
|
|
Occasional accident |
12 (19.7) |
1 (7.1) |
|||
|
Continent |
16 (26.2) |
2 (14.3) |
|||
|
Continence – bowel, n (%) |
|||||
|
Incontinent/enemas |
28 (46.7) |
8 (57.1) |
N/A |
0.640 |
|
|
Occasional accident |
7 (11.7) |
2 (14.3) |
|||
|
Continent |
25 (41.7) |
4 (28.6) |
|||
|
Total Stroke Mobility Scale Score, median (IQR) |
11.0 (10.0 to13.0) |
9.0 (7.0 to 13.0) |
1 (0 to 3) |
0.135 |
|
|
Days admit to rehabilitation assessment, median (IQR) |
9.0 (5.0 to 14.0) |
10.5 (7.0 to 15.0) |
–2 (–6 to 2) |
0.260 |
|
|
Length of stay (days), median (IQR) |
12.0 (8.0 to16.0) |
27.5 (11.0 to 38.0) |
–13.5 (–20 to –3) |
0.005 |
|
|
aHodges–Lehmann estimator for continuous data and risk difference for categorical data; bContinuous data analysed using Mann-Whitney U-test and categorical data analysed using Fisher’s Exact test; cn = 60; dn = 59; en = 58. CI: confidence interval; IQR: interquartile range; mRS: modified Rankin Scale; N/A: not applicable (unable to be calculated). |
|||||
Of those patients accepted for rehabilitation 100 % were subsequently discharged to rehabilitation. For those patients not accepted, almost half (43%) were discharged to residential care or a transitional program whilst awaiting residential care, just over one third (36%) were discharged to a hospital based geriatric evaluation unit and one fifth (21%) died or were transferred to a palliative care service.
Analysis of the importance ratings of each of the rehabilitation questionnaire items showed that the 3 most important individual items (highest scores on the untransformed 0–10 visual analogue scale) for patients accepted to rehabilitation were the patients’ pre-morbid cognition (median 8.4, IQR 7.2–8.8), pre-morbid mobility (8.3, 6.8–9.0) and pre-morbid communication (8.0, 6.7–8.8). For those not accepted the most important items were the patients’ current mobility (8.3, 5.4–8.6), social support (8.2, 6.7–8.5) and current cognition (8.2, 7.3–8.5). There were differences in importance between the two groups with relation to (median accepted, not accepted) pre-morbid cognition (8.4, 6.9, p = 0.002), pre-morbid mobility (8.3, 7.1, p = 0.01), pre-morbid communication (8.0, 5.7, p < 0.001), current mobility (5.8, 8.3, p = 0.05) and mood (5.6, 5.1, p = 0.013). After adjusting the p-value for multiplicity (p = 0.002), only the differences in ratings on the pre-morbid cognition and pre-morbid communication items remained significant. Although there was a difference between groups for one of the two organisational items [bed availability, 2.4, 1.0, p = 0.008)], the importance was rated very low in both groups. Fig. 1 illustrates the individual items measured and the importance ratings given for those accepted for rehabilitation and those not accepted.
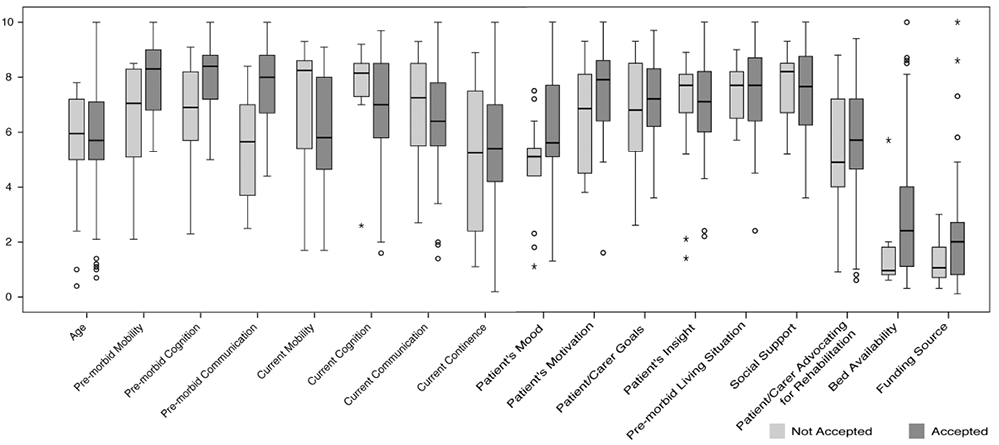
Fig. 1. Box plot showing median (solid bar), interquartile (IQR) range (bar width), whiskers (≤ 1.5 IQR) and outliers of the importance ratings of the 17 rehabilitation assessor questionnaire items by acceptance status.
Additional items identified by the rehabilitation assessors as being important and not on the questionnaire were co-morbidities, allied health team assessment, fatigability, medical stability and rehabilitation potential.
The Kaiser-Meyer-Olkin Measure of Sampling Adequacy was 0.76, indicating that factor analysis was appropriate for this data. Factor analysis of the 15 patient-related items identified 3 factors accounting for 61.8% of the variance between patients. The 3 factors were interpreted as representing post-stroke status, pre-morbid status, and social attributes. The variables loading > 0.4 on any factor are shown in Table II along with the proportion of variance explained by, and the median extracted score for each factor.
|
Table II. Loading of the 15 patient-related rehabilitation assessor questionnaire items on the 3 identified factors |
|||
|
Variables |
Factor 1 Post-stroke status |
Factor 2 Pre-morbid status |
Factor 3 Social attributes |
|
Age |
0.41 |
||
|
Current mobility |
0.64 |
||
|
Current cognition |
0.82 |
||
|
Current communication |
0.73 |
||
|
Current continence |
0.68 |
||
|
Mood |
0.66 |
||
|
Motivation |
0.75 |
||
|
Insight |
0.82 |
||
|
Pre-morbid mobility |
0.81 |
||
|
Pre-morbid cognition |
0.87 |
||
|
Pre-morbid communication |
0.86 |
||
|
Pre-morbid living situation |
0.63 |
0.55 |
|
|
Patient/carer goals |
0.68 |
||
|
Social support |
0.69 |
||
|
Patient/carer advocating for rehabilitation |
0.78 |
||
|
Total variance |
28.4% |
19.4% |
14.0% |
|
Factor score, median (IQR) [range] |
0.15 (–0.71 to 0.81) [–2.26 to 1.63] |
0.21 (–0.24 to 0.51) [–4.13 to 1.25 |
–0.26 (–0.78 to 0.78) [–3.44 to 1.74] |
|
All loading on factors < 0.4 are not shown. |
|||
Multiple logistic regression analysis demonstrated statistically significant association between the assessor ratings of each of the 3 identified factors and the outcome of being accepted for inpatient rehabilitation (Table III). An increase by 1 unit on the scale of the factor representing post-stroke status increased the odds of being discharged to rehabilitation by 7.3, 2.7 for the factor representing pre-morbid status and 4.4 for the factor representing social attributes. The 2 organisational factors did not contribute significantly when added to the regression model, and all 3 identified factors remained significant.
|
Table III. Logistic regression for acceptance to inpatient rehabilitation using factor scores identified in factor analysis |
||||
|
Factor |
OR |
95% CI for OR |
p-value |
|
|
Lower |
Upper |
|||
|
Post-stroke status |
7.314 |
1.993 |
26.840 |
0.003 |
|
Pre-morbid status |
2.677 |
1.277 |
5.614 |
0.009 |
|
Social attributes |
4.402 |
1.436 |
13.494 |
0.010 |
|
OR: odds ratio; CI: confidence interval. |
||||
Discussion
Best practice guidelines recommend that all patients following acute stroke receive care in a specialised stroke unit. In Australia, 81% of acute stroke patients are managed in hospitals with a stroke unit (33). The evidence also supports provision of specialised inpatient stroke rehabilitation, especially in relation to severe stroke patients (5, 8, 34). However, there is significant variation in practice with regards to access (4, 12) and a paucity of evidence relating to the rehabilitation selection process (13). This study is the first to examine the factors that influence decision-making regarding selection for rehabilitation following severe stroke.
For patients accepted to rehabilitation, items relating to pre-morbid status were the most important factors. Conversely, items relating to post-stroke status and social support were the most important factors for those patients not accepted for rehabilitation. This is reflected in part by the patient characteristics where those patients who were discharged to rehabilitation tended to have a higher functional level pre-stroke and were less likely to live alone. In addition, there was a non-significant trend for patients not accepted to display lower levels of current mobility. Whilst the value of pre-morbid and post-stroke function have been established as predictors of acute discharge disposition following stroke, social attributes such as patient/family goals have not (13). The results of this study suggest that for some patients, in addition to known prognostic indicators, social attributes are also important in the rehabilitation decision-making process, particularly with regards to the decision not to accept.
Age and continence following stroke have been documented extensively as being important prognostic indicators for functional level and discharge disposition (both acute and final) following stroke (13). In addition, in this study, there was a significant difference between the two groups with respect to age. However both of these items were among the lower ranked items in terms of importance ((age: accepted median 5.7 (IQR 5.0–7.1), not accepted median 6.0 (IQR 5.0–7.2); continence: accepted median 5.4 (IQR 4.2–7.0), not accepted median 5.3 (IQR 2.4–7.5)). These results further support the notion that acceptance for rehabilitation for severe stroke patients is not based on known prognostic indicators alone.
Comparing the results with our previously reported study of variables associated with discharge to rehabilitation after acute severe stroke (14) reveals some interesting findings. Whilst the patient’s age was found to be independently associated with discharge to rehabilitation, age was one of the lower ranked items in terms of importance in the rehabilitation assessor decision-making process. One possible explanation for this is the correlation of age with other variables (for example, a person of older age was more likely to display lower levels of cognition and was more likely to be incontinent) rather than purely being a predictor of recovery. This indicates that the rehabilitation assessors, in assessing the clinical presentation of the patient, were focusing on each variable individually rather than focusing on a single variable that has demonstrated correlations to other variables. In contrast to these findings pre-stroke disability (as measured by the modified Rankin Scale) and current mobility (as measured by the Mobility Scale for Acute Stroke) were independently associated with discharge for rehabilitation and were also found to be important variables in the decision-making process with regards to suitability for rehabilitation. Those patients with higher levels of pre-stroke disability and lower levels of current mobility were less likely to be discharged to rehabilitation. However, in the rehabilitation assessor’s decision-making process pre-morbid status was more important when the decision was to accept the patient for rehabilitation, and current mobility was more important in the decision not to accept the patient for rehabilitation. In addition, in this study, the rehabilitation assessors did not consider organisational variables as being important in their decision, whilst in the prognostic analysis of the data the hospital unit was a significant factor. Therefore, whilst organisational factors may affect access to rehabilitation this does not appear to be as a result of the rehabilitation assessors’ intentions.
Factor analysis of the rehabilitation assessor items identified 3 distinct factors, interpreted as post-stroke status, pre-morbid status and social attributes. Each factor was significantly associated with the decision regarding rehabilitation acceptance. The identification of these factors may assist in simplifying future studies of rehabilitation acceptance.
The importance of organisational factors in selection for rehabilitation following stroke such as insurance status and affiliations between hospitals has been previously reported (11), however, this was not demonstrated by the present study. This may be reflective of differences in the health care systems and services across different countries. In addition, the findings of this study do not support the hypothesis that organisational factors may be potential contributors to variations in practice with regards to selection for rehabilitation following stroke (4).
Whilst rate of acceptance for those patients referred to rehabilitation in this study was higher (81.3%) than we had anticipated, less than 75% of all eligible patients were referred for a rehabilitation assessment. The overall rate of discharge to rehabilitation for the 117 severe stroke patients meeting the inclusion/exclusion criteria was 52%. This indicates that the selection for rehabilitation process begins with the acute hospital team and their decisions as to which patients are referred for a rehabilitation assessment. Current consensus within the literature is that assessment for ongoing rehabilitation should be conducted by a specialist rehabilitation team (5, 8). Further investigation is warranted into the screening processes of the acute health team with regards to the decision making process for referral for rehabilitation assessment.
In this study descriptive information about the rehabilitation assessors’ experience in conducting rehabilitation assessments was collected. The experience of the rehabilitation assessors ranged from less than 1 year to greater than 10 years with more than one quarter (29%) of the assessors participating in this study having less than one year of experience in rehabilitation assessment. Future studies aimed at determining the impact of experience in rehabilitation assessment on decisions made would help inform discussion with regards to the amount and type of training required to perform rehabilitation assessments for patients after stroke.
Measurement of the assessors’ ratings of the items was conducted using a visual analogue scale. Although the reliability of the scale was not formally tested, the use of visual analogue scales have been reported to be a reliable method to measure subjective responses (35). In addition, the scale was designed based on the results of previous research to maximize reliability, including the length of the scale and restriction to a unipolar scale with the separate ratings (positive, negative and neutral) to indicate the direction (35).
As this was the first study of the rehabilitation assessor decision making processes we were unable to formally assess the validity of the scale used. To determine items for inclusion in the rehabilitation assessor questionnaire an extensive literature review was undertaken (13). However, as the results indicated that the most important factors were not always known prognostic indicators, it is possible that other important items may have been excluded from the questionnaire. To assist in the identification of these items rehabilitation assessors were given the opportunity to list additional items when completing the questionnaire. The additional items identified by assessors were co-morbidities, allied health team assessment, fatigability, medical stability and rehabilitation potential. These items warrant consideration in the planning of future studies.
Finally, although this was a multi-centre study, sites were limited to a single state (Victoria) in Australia. Inpatient rehabilitation in Victoria is generally provided in a separate sub-acute facility which, although funded by a casemix based funding system (36), have no external selection based criteria imposed. As the models for the provision of rehabilitation vary widely (7), caution should be used when generalising the results of this study to other countries.
In conclusion, this study has highlighted the importance of the patient’s pre-morbid, post-stroke and social status in the rehabilitation decision-making process following severe stroke. Factors regarding patient’s pre-morbid status appear to be the most important in the decision to accept, whilst the most important factors when the decision is made not to accept are related to the patients’ post-stroke and social status. The identification of these factors and the differences in importance between the two groups provides valuable information that could be used in the development of a model to improve equity of access to rehabilitation following severe stroke.
Acknowledgements
The authors would like to thank the stroke unit physiotherapy staff at the participating hospitals for agreeing to take part in, and collect data for, this study.
References

