Christophe Luthy, MD1, Christine Cedraschi, PhD1, Patrick Pasquina, RN2, Christophe Uldry, MD3, Noëlle Junod Perron, MD4 and Jean-Paul Janssens, MD2
From the 1Division of General Medical Rehabilitation, 2Division of Pulmonary Diseases, Geneva University Hospitals and University of Geneva, 3Pulmonary Unit, Hospital of Rolle, Nyon and 4Division of Primary Health Care, Geneva University Hospitals, Geneva, Switzerland
OBJECTIVE: To explore the perception of dyspnoea in patients with severe chronic obstructive pulmonary disease.
DESIGN: Cross-sectional study using mixed methods.
METHODS: Thirty-two patients with severe chronic obstructive pulmonary disease were included. Data collected included 3 health-related quality of life questionnaires (SF-36, St George and Maugeri respiratory questionnaires) and the Hospital Anxiety and Depression scale (HADS) to assess the impact of chronic obstructive pulmonary disease on quality of life and psychological functioning. Patients were then asked to draw their body and represent difficulties related to breathing. Drawings were coded and categorized. Patients’ comments were transcribed.
RESULTS: HADS showed scores of depression and anxiety as high as 12.3 ± 2.6 and 9.3 ± 2.2, respectively; SF-36 subscales were severely affected, and the St Georges and Maugeri questionnaires indicated a high impact of chronic obstructive pulmonary disease (79 ± 13 and 60 ± 18, respectively). Drawings illustrated the pervasiveness of dyspnoea; patients’ comments stressed breathlessness. Obstruction and tightening were salient, with a prominent representation of the head and internal structures, e.g. the lungs and the airways.
CONCLUSION: Patients’ drawings capture a global expression of illness experience. They provide insight into the heterogeneity of patients’ perceptions, and allow acknowledgement of patients’ representations and experiences. This may, in turn, help in gaining patients’ participation in rehabilitation programmes or adherence to new medications.
Key words: patients’ drawings; illness representations; chronic obstructive pulmonary disease; mixed methods.
J Rehabil Med 2013; 45: 694–700
Correspondence address: Christophe Luthy, Division of General Medical Rehabilitation, Geneva University Hospitals, CH-1211 Geneva 14, Switzerland. E-mail: christophe.luthy@hcuge.ch
Accepted Mar 6, 2013; Epub ahead of print Jun 24, 2013
INTRODUCTION
Chronic obstructive pulmonary disease (COPD) is a major cause of chronic morbidity and mortality worldwide. It is a slowly progressive disorder, characterized by increasing airflow obstruction, leading to chronic respiratory insufficiency; acute exacerbations occur at variable frequencies and may aggravate the downhill course of the disease; many patients experience marked dyspnoea and severe limitation in everyday life activities (1, 2). Although pulmonary rehabilitation is clearly effective in improving symptoms and quality of life in COPD, patients with advanced disease have a poor quality of life, and the impact of pharmacological treatment is marginal (3, 4).
Representations of patients with COPD regarding their illness and their symptoms have a major impact on their attitude towards treatment (5). Patients’ perceptions are significantly associated with outcomes, such as adherence to treatment, psychological adjustment (6), health-related behaviour and, more specifically, physical role and social functioning, as measured by the Medical Outcomes Study Short Form General Health Survey (MOS) (7). The importance of gaining insight into the patients’ perceptions of their illness has been largely acknowledged (8).
Measurement of patients’ perceptions of illness often relies predominantly on the use of self-administered questionnaires. While questionnaires allow the investigation of predetermined validated items and dimensions, they may not identify idiosyncratic representations that play an essential role in determining health behaviours (9). Various studies have used patients’ drawings as a way to gain insight into their representations of health problems (10–16). Studies have shown that patients’ drawings of their illness allow access to their perceptions about the nature of their illness, as well as disease-related changes (11, 17).
Drawing traditionally belongs to the psychological investigation of children, as a privileged medium of expression of their representations. In adults, drawing may rather have a diagrammatic function, i.e. providing an indication of what the individual considers important. Drawing synthesizes perceptive and representative elements, and combines idiosyncratic and collective aspects. Analysing the meaning of drawing, Wallon et al. (18) notes that graphical production reduces reality to better evoke it; in addition, its verbal equivalent is not just a single word, but at least a statement or even a series of statements.
We conducted an exploratory qualitative study using mixed methods (9). The aim of the study was to investigate how patients with severe COPD perceive their chronic respiratory impairment and their representation of the possible changes in their body related to their breathing difficulties. This open-enquiry approach was associated with a series of questionnaires in order to better characterize the patients, not only in somatic terms, but also in terms of the impact of COPD on various aspects of their quality of life and psychological functioning.
METHODS
Participants included in this cross-sectional study had been diagnosed as having severe (Stage III and IV) COPD according to Global Initiative for Chronic Obstructive Lung Disease (GOLD) criteria (1, 2), and were recruited during a 3-month period. All new patients hospitalized in two subacute wards were eligible if they were admitted for COPD exacerbation, independently of their gender, age, or use of long-term oxygen therapy. The only exclusion criteria were dementia, or insufficient mastery of the French language, which would prevent patients from completing questionnaires and participating in an interview.
Patients were interviewed face-to-face by an independent researcher, trained in interview procedures. They were first invited to complete a series of questionnaires in order to assess the impact of COPD on various aspects of their quality of life and psychological functioning. The questionnaires were selected for their psychometric properties, both in terms of validity and reliability, as well as for their feasibility; as they are widely used, they also allow for comparison with other studies.
Dyspnoea was evaluated by means of the New-York Heart Association (NYHA) dyspnoea scale and Borg scale (19, 20). The NYHA scale is a 4-point scale frequently used for patients with cardiac and/or respiratory disorders (from I = no symptoms and no limitation in ordinary physical activity, to IV = severe limitations; experiences limitations even while at rest). The Borg scale is a category scale (range 0–10) with verbal expressions of severity anchored to specific numbers (from 0 = nothing at all to 10 = maximal). Three health-related quality of life (HRQL) questionnaires were used (1 generic and 2 disease-specific). The 36-question Short Form of the MOS-form survey (SF-36), a generic questionnaire widely used in patients with chronic disorders (21–23), explores 8 domains: Physical Functioning, Role Physical, Bodily Pain, General Health, Vitality, Social Functioning, Role Emotional, and Mental Health. For each scale, item scores are coded, summed, and transformed to a scale ranging from 0 (worst health status) to 100 (best health status). The St George Respiratory Questionnaire (SGRQ) (24, 25) is a disease-specific questionnaire, which explores 3 domains: “Symptoms” (respiratory symptoms, their frequency and severity), “Activity”, (activities limited by breathlessness), “Impacts” (social functioning and psychological disturbances resulting from respiratory disease). Scores are also transformed to a 0–100 scale, but higher scores are related to increased impairment. The Maugeri Respiratory Failure (MRF-28) questionnaire (26, 27) is also a HRQL questionnaire focused on patients with chronic respiratory impairment, exploring: “Daily activity”, “Cognitive function” (memory and concentration), and “Invalidity”. Scores are transformed as for the SGRQ: higher values implicate increased impairment. The fourth questionnaire was the Hospital Anxiety and Depression scale (HAD); the HAD comprises 14 Likert-type items, 7 for anxiety and 7 for depression, each ranging from 0 to 3 for a total score ranging from 0 (no symptoms of anxiety or of depression, respectively) to 21 (severe symptoms of anxiety or of depression). Values between 8 and 10 are considered borderline; scores above 10 are suggestive of an anxiety and/or depressive disorder (28, 29). Results of questionnaires are reported as mean values (standard deviation; SD).
Participants were then asked to draw their body and represent limitations and difficulties related to breathing. They were provided with the following instructions: “We would like you to draw your body as you perceive it”. “We would also like you to draw the limitations and difficulties related to breathing as you experience them. Your drawing abilities are not the focus of this study. Just draw your body and your breathing difficulties as you can. Take your time, there is no time limit.” They were given a blank 297 × 210 mm sheet of paper and a pencil, and they were encouraged to complete the drawing task. These instructions were adapted from other studies investigating patients’ representations of back problems (13), headaches (11) and heart failure (15). We chose to ask the participants to draw their body and not a specific anatomical part (i.e. respiratory system) in order to capture their perception of their breathing impairment and its impact on their body. At the end of task completion, patients were asked to comment on their drawing. These comments, as well as comments made during the drawing task, were tape-recorded and transcribed.
The coding procedure included 3 dimensions. The procedure was derived from qualitative content analysis. The drawings were analysed using a manual data indexing technique to first identify the constitutive elements of the drawings (30). The coding focused on the body parts (e.g. head, mouth) and internal anatomical structures (e.g. lungs, heart). This coding also included the perception of limitations and difficulties (e.g. obstruction, tightening) suggested in the drawings. The patients’ comments were used to clarify their representation (31). As for the second dimension, the drawings were then analysed to identify the configuration of the drawings, i.e. the way the constitutive elements were organized and distributed in the drawings. Three empirical categories characterizing the type of drawing were constructed: (i) a body shape, partial or complete, with no representation of internal anatomical structures; (ii) an anatomical drawing (with no link to a body shape); and (iii) combined elements (a body shape, partial or complete, with anatomical structures). This procedure was performed by two researchers (an internist and a psychologist) who independently coded the constitutive elements of the drawings and the type of drawing. The coding used a constant comparative method (30, 31), which consists of analysing the data by comparing each response with earlier observed responses. This was followed by discussion and comparison of the coding of the data, which were subsequently used to establish the final grids. These grids were then used independently by the two researchers to analyse the drawings in order to maximize theoretical sensitivity and rigor (31). As for the third dimension, in accordance with other studies based on patients’ drawings, the size of the drawings was measured in millimetres from top to bottom and from side to side (11).
Statistical analysis
Values are reported as means (SD), unless specified otherwise. Overall agreement between the two researchers for classification of drawings was quantified by means of the kappa statistic (32). Relationships between characteristics of drawings and HRQL scores or functional parameters were analysed by logistic regression (SPSS 15.0 Command Syntax Reference 2006, SPSS Inc., Chicago, IL, USA).
Patients were interviewed at the hospital and were informed that their responses would not impact on their care. Complete confidentiality was guaranteed and responses were anonymized. The protocol conformed to the Declaration of Helsinki and was approved by the local ethics committee of Geneva University Hospitals; written informed consent was obtained from all participants.
RESULTS
A total of 32 consecutive patients was contacted, all of whom accepted to participate in the study protocol. Only one participant declined the drawing task (declaring he had no drawing ability and that drawing was a children’s task anyway).
Clinical data and pulmonary function tests are shown in Table I. Patients had severe COPD, stage GOLD III for most of them. Twenty-six patients were on long-term oxygen therapy, initiated according to prevailing national guidelines (33). Results of the questionnaires indicated a very strong impact of disease in terms of symptoms, activities of daily life, and invalidity, with very high scores for both SGRQ and MRF-28 (Table II). HAD mean values were clearly suggestive of depression, and borderline for anxiety disorders (Table II). SF-36 values (Table II) were also strongly affected by the respiratory illness. Like all other subscales, “Mental Health” was decreased compared with healthy subjects in the same country (21); this is in agreement with the results of HAD. Values obtained for the items “Role Physical” and “Role Emotional” were very low (zero for the “Role Physical” subscale), resulting from a “floor” effect in this population.
|
Table I. Summary of clinical data concerning patients studied |
|
|
Mean (SD) |
|
|
Age, years |
64.2 (13.2) |
|
Gender, M/F, n |
19/13 |
|
Smoking history, pack-years, n |
89 (27) |
|
Hospital stays over past 2 years, n |
5.5 (1.9) |
|
FEV1, L |
0.72 (0.23) |
|
FEV1/FVC, % predicted |
37.8 (7.4) |
|
Number of pack years = (packs smoked per day)×(years as a smoker). SD: standard deviation; FEV1: forced expiratory volume in 1 s; FVC: forced vital capacity. |
|
|
Table II. Scores for dyspnoea and health-related quality of life |
|
|
Score |
Mean (SD) |
|
NYHA Dyspnea scale |
2.9 (0.7) |
|
Borg Scale (0–10) |
3.0 (0.7) |
|
St George Respiratory Questionnaire |
|
|
Symptoms |
86 (7) |
|
Activity |
87 (14) |
|
Impact |
72 (17) |
|
Total |
79 (13) |
|
MRF-28 |
|
|
Daily Activity |
66 (22) |
|
Cognitive function |
14 (15) |
|
Invalidity |
69 (21) |
|
Total |
60 (18) |
|
Hospital Anxiety and Depression scale |
|
|
Depression |
12.3 (2.6) |
|
Anxiety |
9.3 (2.2) |
|
SF-36 |
|
|
Physical functioning |
27 (12) |
|
Role physical |
0 (0) |
|
Bodily pain |
58 (15) |
|
General health |
15 (10) |
|
Vitality |
26 (9) |
|
Social functioning |
22 (17) |
|
Role emotional |
2 (12) |
|
Mental health |
51 (6) |
|
For both St George Respiratory Questionnaire and MRF-28 (Maugeri Respiratory Foundation Questionnaire) questionnaires, scores range from 0 to 100; higher values indicate more severe impairment. For Hospital Anxiety and Depression scale, values ranging between 8 and 10 are considered borderline, and scores above 10 suggestive of an anxiety and/or depressive disorder. For the SF-36 (Short Form of the MOS-form survey), scores range from 0 to 100; higher values indicate better health status. SD: standard deviation. |
|
Twelve patients drew a body shape, partial (n = 7) or complete (n = 5); 8 patients drew internal anatomical structures only; 10 drew combined elements (a body shape, partial (n = 4) or complete (n = 6), with anatomical structures); 1 drawing could not be classified. Thus, the majority of drawings included elements of body shape. Among these elements, the head appeared as prominent, including the parts involved in breathing, namely the nose and mouth (Table III). Drawings of internal anatomical structures represented essentially the lungs and the respiratory airways. Between-rater overall agreement was very high (K > 0.90). Fig. 1 presents some examples of drawings.
|
Table III. External and internal body parts indicated in the drawings |
|
|
Components |
n (%) |
|
Head |
20 (65) |
|
Eyes |
11 (35) |
|
Nose |
12 (39) |
|
Mouth |
14 (45) |
|
Upper limbs |
10 (32) |
|
Trunk |
15 (48) |
|
Lower limbs |
13 (42) |
|
Respiratory tubes |
11 (35) |
|
Lungs |
14 (45) |
|
Heart |
2 (6) |
|
Diaphragm |
2 (6) |
|
Sinus |
2 (6) |
Fig. 1. Sample of 8 representative drawings by patients with chronic obstructive pulmonary disease who were asked to draw their body and represent limitations and difficulties related to breathing. See text for details.
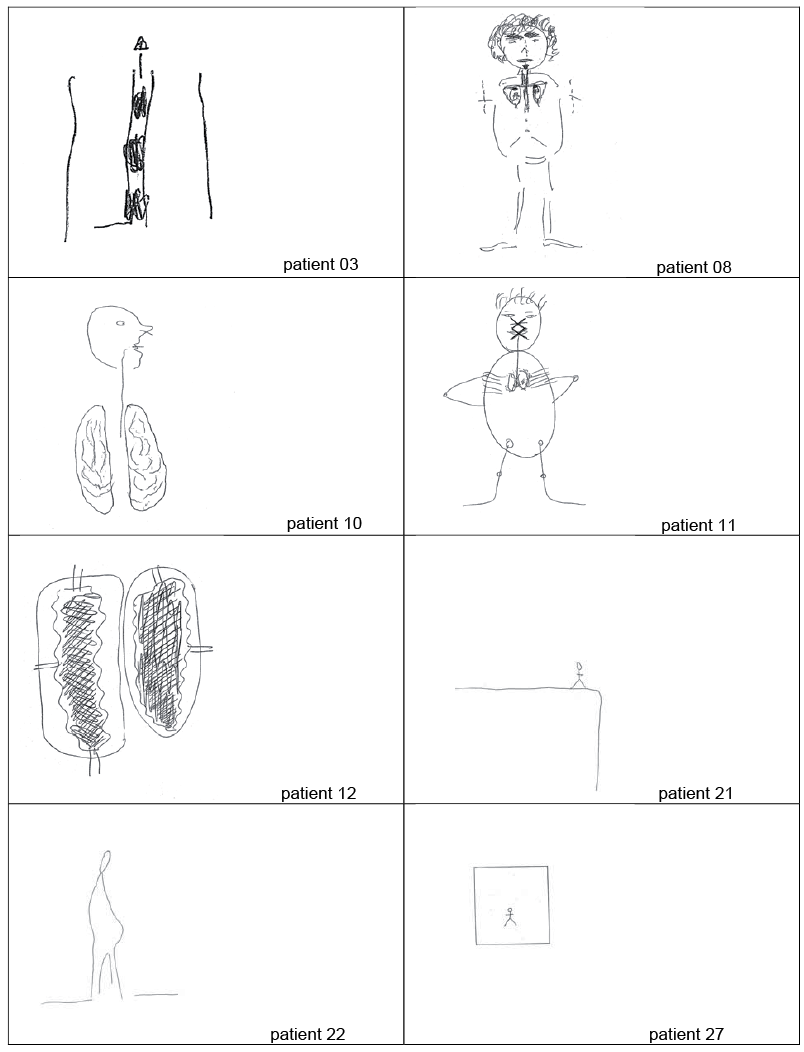
Several types of difficulties in breathing were mentioned.
Obstruction of airflow was presented as occurring at different levels: the mouth, or the lower airways (“There’s only this… plug in the bronchi, it stops me from breathing” [Fig. 1 – patient 03]; “The lungs become small, very small, too small. I can no longer breathe through there, where the air should normally flow. And there you see it should go up to the mouth” [patient 08]).
Restriction (tightening, constriction) of the lungs: (“The lung shrinks and becomes stiff, it cannot breathe any more” [patient 12]). Tightening was also frequently evoked either as a perception of thoracic constriction (“… nothing goes through the nose or the mouth any more. It pulls on the ribs; the muscles are too short. […] we breathe like dogs with the ribs squeezed, there’s no more room to breathe” [patient 11]) or as a more internal constriction (“It’s the lungs… it feels so tight that I’m afraid that it’ll explode the small bubbles and the lungs”).
Dilatation of the lungs (which is what physiologically happens in emphysema) was mentioned by only one patient.
The unclassified drawing was a black spot, further described by the patient as “a black hole, something very dense, something that gets stuck in there and poisons me from the inside…”
Fig. 1 shows examples of how the drawings may illustrate the perception of damages to the respiratory function, but also the pervasive nature of breathlessness. Breathlessness is represented by the darkening of the sick body organs or by closure of the airflow [patient 11]. The emphasis on breathlessness can lead the patients to draw their body as an empty space [patient 22], immobilized because of the damages to the respiratory function (“That’s the ground and the body is like this, with the legs on the ground. I don’t move, I just try to catch my breath. It’s not very nice to look at… It makes me look a bit sad… with my belly pushing forward and also preventing me to breathe”). The body can even be presented as dismembered [patient 10] or reduced to its damaged parts [patient 03 and patient 12]. Breathlessness can also be presented as permeating every level of body perception [patient 21 (“… This is me and to be out of breath, it’s like this, it’s to be at the end of the end. I don’t want to die but I can feel I’m at the end”) and patient 27 (“I take your ruler to draw the box first, that’s it, it’s a box. No way to escape the disease or to escape to myself. Breathlessness and locking up, it’s how I see it”)].
The mean height of the drawings was 115.1 mm (SD 55.5) and the mean width was 84.0 mm (SD 45.1). There was no association between the type of drawing (body shape, partial or complete, internal anatomical structures, or combined elements) and their size. There was no association between the type or size of the drawings and the scores of the questionnaires, whether generic (SF-36 and HAD) or disease-specific (SGRQ and MRF-28), or the clinical variables.
DISCUSSION
This is, to our knowledge, the first study to analyse drawings as a transcription of patients’ perception of illness in severe COPD. These representations are very distant from the biomedical view of the body and respiratory function. Patients’ representations of their body and breathing difficulties ranged from the drawing of an isolated body part to the drawing of a body shape, sometimes even presented in a broader context. The drawings emphasized the patients’ sensation of breathlessness and body areas related to their handicap.
Participants had severe COPD with a major impact on HRQL, as shown by both generic and disease-specific HRQL questionnaires (26, 27, 34–36).Values obtained for the SF-36, the SGRQ sub-scores and the MRF-28 are in agreement with those published for severe COPD (27, 34, 35, 37). The “floor effect” observed for the “Role Physical” and the “Role Emotional” sub-scales of the SF-36 reflect the experience of major limitations in these patients with severe COPD. A similar “floor effect” for these two sub-scales were reported in 20% of patients in a validation study of the SF-36 (38). Very low values for these two scores are occasionally reported. In the manual for the SF-36, normal values for the US population include 10.3% and 9.6% of the normal population having a “0” score for the “Role Physical” and the “Role Emotional” sub-scales, respectively (23).
Impact of COPD on HRQL was in agreement with the pervasiveness of dyspnoea illustrated in the drawings. Drawing offered to the complaint of breathlessness an expression that goes beyond the possibilities of verbal expression. The graphic expression of the patients’ subjective experience of breathlessness suggested either “obstruction” or “tightness”, “dilatation” and “distension”, or both. This complaint was sketched in various ways, e.g. through occlusions, darkening, contextualization, which modulated its intensity. Suffering related to COPD was expressed beyond the anatomical body, and extended from the feeling of being out of breath to the fear of being unable to breathe, reaching “the end of the end” and to the feeling that there is “no way to escape from the disease or to escape from myself. Breathlessness and being locked up”. Patients’ representations were far from the biomedical view in their description of breathlessness. In particular, many drawings emphasized the perception of a contraction, or tightness of the chest, which is opposite to the hyperinflation of the lungs that occurs in emphysema. Indeed, while all the patients had emphysema, and thus various degrees of hyperinflation, a number of them drew their lungs as small organs in relation to their sensations of being out of breath and of chest tightness.
Drawings thus provide an indication of how the illustrators explain to themselves and to others how they perceive their health problem. As an evocation, rather than a recognition task, drawing does not necessarily indicate the whole body of knowledge of the illustrator, but rather the elements he/she considers most relevant, compared with the internal or external model (18). Drawings capture a specific expression of the illness experience, i.e. a syncretic representation, including both sensitive and affective elements, such as the sensations related to hyperinflation or to sarcopenia and the physical and psychological fatigue, or even the exhaustion, as well as the distress associated to these consequences of the disease. This representation of the disease may render the perception of exercising more of a dangerous, and sometimes even life-threatening, challenge. Furthermore, while rehabilitation programmes emphasize peripheral muscular reinforcement or exercise in general, drawings showed body shapes often lacking upper limbs and/or presenting thread-like lower limbs. This representation may also act as a barrier to the acquisition of new skills and self-confidence (39).
Drawings performed in this setting also provided an indication of what patients considered relevant in the context in which the query was made, which referred to scientific knowledge (healthcare setting). The weight given to anatomical structures, represented alone or included in a body shape, in their drawings further emphasized the importance for the patients of a biomedical representation of the disease. Anthropologists have suggested that anatomy and physiopathology operate a clear dissociation between the person and the body, as a requisite for the construction of scientific knowledge (40). To better understand it, scientific knowledge thus depersonalizes the disease, which is seen as the defect or the failing of an organ or of a function. Conversely, lay knowledge tends to personalize the illness, by including the individual’s suffering and even contextualizing it, for example, the two patients who drew a person on the edge of a cliff and a coffin, respectively (patients 21 and 27, Fig. 1). The drawings would thus stress the role of the clinician in bridging the gap between these two forms of knowledge by re-contextualizing, i.e. individualizing, the diagnosis and the treatment, be it medication or exercise programmes.
As in other studies, our results point to the drawings as eliciting the patients’ representations of their illness, but also the patients’ distress regarding their experience of their illness (11, 13–17). In contrast to studies in patients with heart disease (10, 15) or lung disease (16), in our study the characteristics of the drawings were not associated with clinical variables. This may be related to the fact that the drawings are more an indicator of the patient’s global distress than of the specificity of the disease. It may also be related to the fact that our sample of patients was highly homogenous in terms of the severity of the disease and of its consequences, as shown by the generic and disease-specific questionnaires.
The limitations of this study should be acknowledged. Results obtained provide an insight into the perception of a specific group of patients with severe COPD, most of whom were on long-term oxygen therapy. In this population, impact of respiratory impairment on HRQL scores was particularly important. Observations related to the drawings analysed in this study cannot be generalized to less severe COPD or to patients with other advanced respiratory disorders. In addition, physiological correlates or phenotypes of COPD may be related to the manner in which breathlessness is expressed; for example, distension is typical of hyperinflation, as in severe emphysema, which may also lead to chest tightness. Previous studies have tried to establish a relationship between a list of descriptors used by patients for their dyspnoea and specific mechanisms and/or respiratory pathologies (41, 42). In these studies, COPD was associated with a sensation of “air hunger” and “increased work of breathing”. Plethysmographic measurements were not available for our patients, and we could thus not explore the possible relationship between physiological parameters and patients’ perception and representation of dyspnoea. This study also has strengths, in particular the use of mixed methods, with the drawings enabling a better understanding of how severe chronic respiratory impairment impact on activities of daily living, symptoms, invalidity, anxiety and depression, as assessed in generic and disease-specific questionnaires.
This study has various implications for the clinicians. The graphic representations provided by the patients emphasize the distressing impact of dyspnoea. This impact involves both the physical component, including the associated handicap, and the psychological issue, including the emotional distress. In some drawings, the sensation of dyspnoea even appeared to elude the perception of self and/or of other parts of the body. These results suggest the importance of addressing this issue in the therapeutic encounter. The drawings also illustrate the gap between patients’ views of the illness and health professionals’ knowledge about the disease and treatment. Patients and health professionals refer to a biomedical model of the body, sometimes even using the same terms. However, these terms may not convey the same meaning or cover the same reality. Hence, there may be an increased risk of misunderstandings between patients and therapists, related to the term itself, but also due to the belief that they have understood each other because the same term has been used. This study stresses the necessity for the clinician to ensure the use of a common language. The drawings provide further insight into the heterogeneity of the patients’ perceptions, and thus allow acknowledgement of the patients’ individual experiences. These subjective perceptions and experiences are of major importance in situations such as trying to gain the patients’ active participation in a rehabilitation programme or adherence to a new medication to help alleviate symptoms. Indeed, considering the patients’ views about breathlessness in terms of causes and consequences may help in constructing a shared workspace. This workspace may, in turn, allow for the establishment of a common understanding of treatment goals and expected outcomes. This may be particularly important in discussing physical reconditioning in patients with dyspnoea as well as related fear of movement and distress.
ACKNOWLEDGEMENTS
This study benefited from an unrestricted grant from Astra Zeneca.
The authors report no conflicts of interest.
REFERENCES

