Joachim Liepert, MD1, Johanna Greiner1 and Christian Dettmers, MD2
From the Departments of Neurorehabilitation, 1Klinken Schmieder, Allensbach and 2Konstanz, Germany
OBJECTIVE: To explore whether stroke patients exhibit increases in motor excitability during action observation, whether differences exist between the affected and non-affected sides, and between pure motor strokes and predominantly sensory strokes.
METHODS: In 18 patients (10 pure motor strokes, 8 predominantly sensory strokes, < 6 months after the stroke) transcranial magnetic stimulation was used to test motor excitability while the patients viewed a video showing a hand performing pinch grips. Transcranial magnetic stimulation pulses were applied at 120% of the individual motor threshold at rest, as obtained from the affected hemisphere. Recordings were taken simultaneously from the first dorsal interosseous muscle of both hands. Motor performance was evaluated with the Box and Block Test.
RESULTS: Transcranial magnetic stimulation-evoked muscle responses obtained from the affected and the unaffected sides were significantly higher during action observation than during rest (p = 0.024 and p = 0.004, respectively). This effect was significantly stronger when measuring the same hand as the one viewed in the video (p = 0.019). No difference was found between motor and sensory strokes. In 11 patients there was an action observation-associated increase in the amplitudes of motor evoked potentials in the affected side. In 15 patients there was an action observation-associated increase in motor evoked potentials amplitudes in the unaffected side.
CONCLUSION: The results are potentially relevant for the use of action observation as a treatment strategy.
Key words: stroke; action observation; transcranial magnetic stimulation; motor excitability.
J Rehabil Med 2014: 46: 00–00
Correspondence address: Joachim Liepert, Department of Neurorehabilitation, Kliniken Schmieder, Zum Tafelholz 8, DE-78476 Allensbach, Germany. E-mail: j.liepert@kliniken-schmieder.de
Accepted Oct 25, 2013; Epub ahead of print Mar 24, 2014
Introduction
The act of observing another person performing a meaningful motor task activates a brain network that mainly involves the inferior parietal lobule, inferior frontal gyrus, and the adjacent ventral premotor cortex (1). This network is known as the mirror neurone network (2). The effects of action observation (AO) on motor excitability have been explored in numerous studies using transcranial magnetic stimulation (TMS). AO enhances corticospinal excitability (e.g. 3–7) and reduces inhibition in the primary motor cortex (3, 5). The muscles involved in the increased motor excitability are the same as those used in the observed action, and their activation is temporally strictly coupled with the dynamics of the observed action (7–9). However, the amount of AO-induced motor facilitation shows large inter-individual variability (10). Increases in excitability are task-related. For example, in observation conditions in which a heavy object was lifted, motor excitability was higher than in conditions in which a light object was lifted (11). Excitability enhancements reflect the observed hand movements rather than the distal goal of the action (9, 12).
Observation of another individual performing simple repetitive thumb movements induced a kinematically specific memory trace of the observed motions in primary motor cortex (13). This memory trace was most pronounced if AO was combined with physical practise in a congruent mode (14).
In contrast to motor imagery, repeated sessions of AO did not further enhance motor excitability (15, 16). During observational learning corticospinal excitability decreased as learning progressed (17). Observational training may increase the muscular strength not only in the observed hand but also in the other hand (18).
Since AO does not require motor performance, but activates motor-associated brain areas, it has been employed in several trials with stroke patients. Most of these studies were performed with chronic stroke patients (19–21). They all report some improvement following the AO therapy. The most recent and most convincing study is a randomized controlled trial with subacute stroke patients demonstrating a superior outcome in the patient group that had AO treatment (22).
The objectives of this study were threefold. First, we wanted to explore whether stroke patients show increased motor excitability during AO. Numerous studies have suggested that motor excitability increases are correlated with the recovery of motor functions after stroke (e.g. 23–25). Secondly, if so, would there be a difference in motor excitability between the affected and the non-affected side? Thirdly, in an earlier study (26) we found that stroke patients with severe sensory deficits had an abnormally low increase in corticospinal excitability during imagination of a tonic pinch grip with the affected hand compared with during imagination of a pinch grip with the unaffected hand, and compared with a patient group with pure motor stroke. A further objective was to determine whether motor excitability changes evoked by AO differ between stroke patients with severe sensory deficits and those with pure motor strokes. If not, treatment with AO might be more reasonable and promising than motor imagery therapy in stroke patients with sensory deficits.
Methods
Patients
A total of 18 stroke patients were included in the study after having given consent to participate. They were recruited during inpatient neurological rehabilitation therapy. Treatments focused on upper extremity function and were similar for all patients regarding amount and duration of therapy. The study protocol was approved by the ethics committee of the University of Constance, Konstanz, Germany. Inclusion criteria included occurrence of a first-ever stroke less than 6 months prior to the study, sufficient strength in the affected hand to grasp and release an object, and the ability to evoke responses in a hand muscle by transcranial magnetic stimulation. Contra-indications included a history of epileptic seizures, inability to understand the instructions, intake of drugs known to affect brain excitability, pregnancy, metallic implants in the brain, and heart pace-makers.
Patient group 1 (PG1) comprised 8 stroke patients (mean age 63 years (standard deviation; SD 10)), 2 women, affected hemisphere, 3 × left, 5 × right) with severe somatosensory deficits. These patients had impairments of the sense of vibration, light touch and stereognosis. Seven of the patients in PG1 had also participated in a motor imagery experiment (26).
Patient group 2 (PG2) comprised 10 stroke patients with a pure motor stroke (mean age 66.6 years (SD 13), 2 women, affected hemisphere, 4 × left, 6 × right). Sense of vibration, light touch and stereognosis were normal. Seven of the patients in PG2 had also participated in a motor imagery experiment (26).
Further details are shown in Table I.
|
Table I. Clinical characteristics of the 2 patient groups. Patients 1–8 belong to patient group 1. Patients 9–18 belong to patient group 2 |
|||||||
|
Patient |
Age, years |
Sex |
Duration, weeks |
Affected side |
Sensory Functions |
Median nerve SSEP |
Lesion location |
|
1 |
49 |
M |
10 |
Left |
Loss of stereognosis, vibration, light touch |
– |
Right thalamus |
|
2 |
57 |
M |
6 |
Left |
Loss of stereognosis, vibration, light touch |
– |
Right thalamus |
|
3 |
74 |
F |
9 |
Right |
Loss of stereognosis, vibration, light touch |
– |
Left brain stem |
|
4 |
49 |
M |
15 |
Left |
Vibration 3/8, stereognosis and light touch reduced |
– |
Right thalamus |
|
5 |
70 |
M |
11 |
Left |
Vibration 5/8, stereognosis and light touch reduced |
(+) |
Basal ganglia including thalamocortical fibres on the right |
|
6 |
69 |
F |
5 |
Right |
Loss of stereognosis, vibration, light touch |
– |
Basal ganglia left hemisphere |
|
7 |
59 |
M |
13 |
Right |
Vibration 6/8, stereognosis and light touch reduced |
– |
Left parietal cortex |
|
8 |
77 |
M |
17 |
Left |
Vibration 5/8, stereognosis strongly, light touch slightly reduced |
(+) |
Right parietal cortex |
|
9 |
79 |
M |
8 |
Left |
Normal |
+ |
Right pons |
|
10 |
31 |
M |
8 |
Left |
Normal |
+ |
Left pons |
|
11 |
83 |
M |
7 |
Right |
Normal |
+ |
Left internal capsule |
|
12 |
62 |
M |
16 |
Right |
Normal |
+ |
Left semioval centre |
|
13 |
65 |
F |
5 |
Left |
Normal |
+ |
Right pons |
|
14 |
77 |
M |
6 |
Left |
Normal |
Not done |
Right pons |
|
15 |
66 |
M |
4 |
Left |
Normal |
Not done |
Right primary motor cortex |
|
16 |
67 |
M |
10 |
Right |
Normal |
+ |
Left pons |
|
17 |
73 |
M |
6 |
Left |
Normal |
+ |
Right semioval centre |
|
18 |
67 |
F |
8 |
Right |
Normal |
+ |
Left internal capsule |
|
M: male; F: female; duration: time interval between stroke and study; median nerve SSEP: somatosensory evoked potential produced by stimulation of the median nerve; –: absent cortical SSEP response; +: normal cortical SSEP response; (+): abnormal cortical SSEP response, either amplitude reduction or prolongation of latency. |
|||||||
Box and Block Test (BBT). To test motor functions, the BBT was administered. This test is frequently used as a measure of dexterity and has been shown to be valid and reliable (27–30). It has a standardized size, is well-known and widespread, is easy to administer and includes the most important aspects of upper extremity motor functions (grasping, moving and releasing an object).
The BBT apparatus consists of a box of specified dimensions divided into two sections. The test involves grasping and moving one-inch (2.54 cm) square wooden blocks from one side of an 8-inch (20.32 cm) square box to the other by passing them over a wooden partition 5 inches (12.7 cm) high using one hand. In our experiment, subjects had to move 15 blocks. The time needed to complete the task is taken as the result.
Procedure
Patients were seated in a comfortable chair and were asked to watch a video attentively. They did not have the task of imagining or imitating the movements seen in the video. Hardwick et al. (31) have shown that observing an action with the aim of imitating it leads to less facilitation than attending to the observation of actions.
Two versions of the video were shown. The patients either saw a right hand or a left hand that grasped a clothes-peg with a pinch grip, held it for 2 s and then attached it to a wooden rod. As soon as the clothes-peg was held between the thumb and index finger the TMS pulse was given. Each trial lasted 5 s. For each hand, 8 trials were performed. As control condition, the subjects watched a video of either a right hand or a left hand that did not move. In each video the subject saw the hand from a first-person perspective. TMS pulses were given at intervals of 5 s. Altogether, 4 videos were shown. The sequence of the videos was randomized. The intervals between the videos amounted to 60 s.
Transcranial magnetic stimulation. Recordings with surface electrodes (belly-tendon montage) were taken simultaneously from the first dorsal interosseus muscle (FDI) on both sides, in order to study motor excitability in both hemispheres simultaneously.
TMS was performed with a circular coil (outer diameter 14 cm) (The Magstim Comp., Dyfed, UK) connected to a magnetic stimulator (Magstim 200 HP). The optimal coil position where motor-evoked potentials (MEPs) could be evoked with the lowest stimulus intensity from both FDI was marked with ink on the scalp to ensure an exact repositioning of the coil throughout the experiment. At this coil position the motor threshold (MT) was determined. MT was defined as the stimulus intensity needed to produce MEPs with a magnitude of 50–100 µV in 5 out of 10 consecutive trials during complete muscle relaxation (32). The MT for the affected side was higher than for the healthy side. We therefore applied TMS single pulses with an intensity of 120% of the MT of the affected side at rest.
Auditory feedback via a loudspeaker ensured that no muscle contraction occurred. Recording of each trial started 30 ms prior to the TMS pulse and finished after 200 ms. Trials with electromyogram contamination produced by involuntary muscle activity were excluded from further analysis. As a control, 24 TMS pulses were applied during rest. The sequence (video showing a right hand and video showing a left hand) was randomized.
Recordings were stored on a Viking IV (Nicolet, Kleinostheim, Germany) and analysed off-line. Upper and lower filters were set to 2000 Hz and 20 Hz, respectively. The sampling frequency was 4000 Hz. MEP amplitudes were measured peak-to-peak. For one part of the analysis, amplitudes of MEPs during AO were expressed as a percentage of the mean MEP amplitude obtained during the rest condition.
If MEP amplitudes recorded from the same hand shown in the video were higher than MEP amplitudes recorded from the other hand, this is termed “congruency”. In contrast, “incongruency” means that recordings were made from the hand not shown in the video.
For further analysis, a laterality index (MEP amplitude of the FDI ipsilateral to the observed pinch grip/MEP amplitude of the FDI contralateral to the observed pinch grip) was calculated. The higher the value, the more the increase in excitability is directed towards the hand shown in the video. This analysis was introduced in order to compare the results obtained in this study more directly with results published earlier (26).
Statistical analysis
To explore whether AO induced an increase in motor excitability, MEP amplitudes (in mV), were used. We calculated differences between control condition and AO with Student t-tests. Due to substantial differences in MEP amplitudes and the large variance produced by direct comparisons between the affected and unaffected sides, each side was tested separately. All other analyses, described below, were performed with amplitudes expressed as a percentage of the mean MEP amplitude obtained during the rest condition.
A 3-factorial analysis of variance (ANOVA) with the factors GROUP (2 levels; pure motor strokes and predominantly sensory strokes), AFFECTED SIDE (2 levels: recordings taken from the affected side and recordings taken from the unaffected side) and CONGRUENCY (2 levels: hand observed in video is the hand from which recordings are taken, and recordings are taken from the hand not observed in the video) was conducted.
ANOVA tests were also used to compare laterality indices between the patient groups. For each patient group, 2 laterality indices exist (MEP size affected side/MEP size unaffected side for AO of the affected side and MEP size unaffected side/MEP size affected side for AO of the non-affected side. A 2-factorial ANOVA with GROUP (2 levels) and LATERALITY (2 levels) was run.
In case of significant differences in the ANOVA, post-hoc t-tests were calculated.
We also calculated correlations between AO-induced motor excitability increases and other parameters (patient age, time since stroke onset, affected side, motor performance, size of somatosensory evoked potential amplitudes, allocation to PG1 or PG2).
The level of significance was assumed at 5%.
Results
MEP amplitudes obtained during AO were significantly higher for the affected (p = 0.024) and for the unaffected side (p = 0.004). On the affected side, the mean MEP amplitude increased from a mean of 0.5 mV (SD 0.054; control condition) to 0.84 mV (SD 0.83; AO condition). On the unaffected side, the MEP amplitude increased from 1.41 mV (SD 1.25) to 2.4 mV (SD 2.1). The ANOVA indicated a significant difference for the factor CONGRUENCY (F = 5.86; p = 0.019). The factors GROUP (F = 0.554; p = 0.46) and AFFECTED SIDE (F = 2.71; p = 0.102) did not show significant differences. There was no significant interaction between the factors.
Motor excitability was significantly more strongly increased when recorded from the same hand that was shown in the video (Fig. 1).
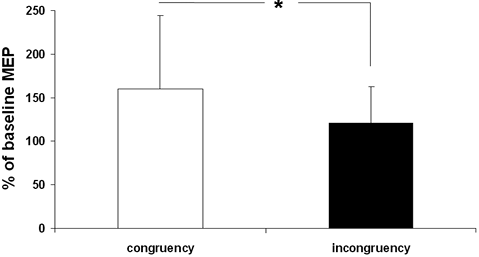
Fig. 1. The bars show motor-evoked potential (MEP) amplitudes expressed as percentage of the MEP sizes obtained in the control condition. “Congruency” means that MEPs were recorded from the same side as was shown in the video. For example, while the patient watched a right-hand MEPs were recorded from the right first dorsal interosseous muscle. “Incongruency” indicates that MEPs were recorded from the hand contralateral to the one viewed in the video. Error bars show standard deviations. *p < 0.05.
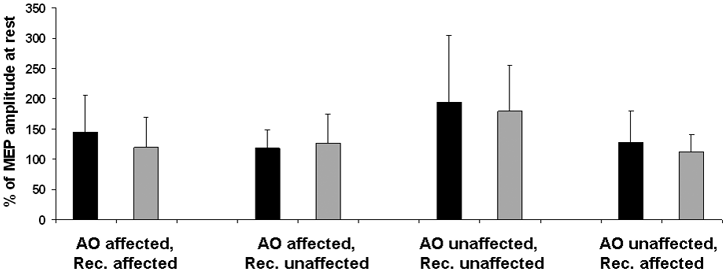
Table II shows the clinical and electrophysiological results. Patients with pure motor strokes needed less time to complete the BBT. However, this difference was not significant (p = 0.11). Patients with pure motor strokes showed congruency for both the affected and the unaffected hand, whereas patients with predominantly sensory strokes showed congruency only for the unaffected hand (Fig. 2). In both groups of patients AO induced an increase in MEP size compared with the control condition.
Analysis of laterality indices indicated no difference for the factor GROUP (F(1;17) = 0.297, p = 0.59), but a trend for the factor LATERALITY (F(1;17) = 4.13, p = 0.051). There was no interaction between the 2 factors (F(1;17) = 0.154, p = 0.697) (Table II).
|
Table II. Results of the Box and Block Test and transcranial magnetic stimulation |
||
|
Pure motor stroke Mean (SD) |
Predominantly sensory stroke Mean (SD) |
|
|
Box and Block Test, s |
41.1 (36.8) |
66.0 (21.4) |
|
Laterality index, AO affected |
1.26 (0.43) |
1.03 (0.49) |
|
Laterality index, AO unaffected |
1.66 (1.0) |
1.63 (0.62) |
|
The laterality index was calculated using the formula “MEP amplitude of the FDI ipsilateral to the observed pinch grip/MEP amplitude of the FDI contralateral to the observed pinch grip”. For interpretation, see methods section. SD: standard deviation; AO: action observation; MEP: motor-evoked potential; FDI: first dorsal interosseus muscle. |
||
Analysis of the condition “congruency” in individual patients showed that, in PG1, 4 patients developed an increase in excitability during AO on the affected side and 6 of these patients showed increased excitability in the non-affected side. In PG2, 7 subjects showed an increase in AO-associated excitability in the affected side and 9 subjects had an increase in excitability in the non-affected side.
We correlated the amount of excitability changes during AO with other parameters. No correlations were found for “time since stroke onset”, “affected side” (right or left), “patient age”, “size of somatosensory evoked potential amplitudes” and “patient group” (PG1 or PG2). The correlation with motor performance (time needed to complete the BBT) showed a trend (r = –0.441; p = 0.067).
Discussion
There were 3 notable results of this study. First, observing another person performing pinch grips increased motor excitability in our patient group. This enhancement was found for the affected as well as for the unaffected hand. It suggests that AO produces basically similar effects in patients and in healthy subjects (3–8). Secondly, the increase in motor excitability of muscles of the hand was significantly stronger for the hand that was viewed in the video. This suggests some specific or focal effect of AO. It corresponds to results obtained with functional magnetic resonance imaging in healthy subjects. In that study, the first-person perspective elicited parietal activation in the hemisphere contralateral to the performing hand as if the modelled action was mimicked with the same anatomical hand (33). Both results are in agreement with the motor-simulation theory of Jeannerod (34), which proposed that perceiving actions involves neural simulation of the same action by the observer. Watching the hand in the first-person perspective (as was the case in our study) induces stronger MEP facilitation than an opposite hand orientation (4). However, our result has an additional implication. Since the excitability increase was not restricted to the hand visible in the video it suggests that, in addition to the congruency-associated effect, there is also a less specific effect that produces an enhanced excitability in both hemispheres. Bilateral increases in MEP amplitudes as an indicator of this bihemispheric excitability change have also been found in a study by Borroni & Baldissera (8). In addition, Porro et al. (18) reported that observation of right-sided finger movements increased muscular strength for both hands to a similar degree. Data analysis of laterality indices indicated a trend towards a greater increase in excitability when watching the hand that corresponded to the unaffected hand in the patients. This tendency was found in both patient groups and might suggest that the unaffected hand has a stronger representation in motor-related brain areas. We tried to identify parameters that correlate with the degree of motor excitability changes during AO. The only factor that approached significance was the negative correlation between motor performance and the amount of MEP size increases. It indicates the trend that AO-associated motor excitability changes are more pronounced in patients with superior dexterity. However, it remains speculative whether a higher motor function is the consequence or the prerequisite for the modulation of AO-associated motor excitability.
Thirdly, patients with pure motor strokes and those with predominantly sensory impairment showed no difference in their AO-induced motor excitability changes. This indicates that the presence or absence of sensory deficits is irrelevant for effects of AO on brain excitability. The result is in contrast to our preceding study in which motor excitability during imagination of a tonic pinch grip was particularly impaired in the patient group with severe sensory deficits. This difference between AO and motor imagery becomes even more robust and obvious when considering the substantial overlap of patients who had participated in both studies. In the patient group with sensory deficits, 7 out of 8 patients had also entered the motor imagery study. In the group with pure motor function impairment, 7 out of 10 patients had participated in both studies.
Considering the results of the current and the preceding study (26), we hypothesize that, in particular, patients with a severe sensory deficit might benefit more from AO training than from motor imagery exercises. Of course, such a hypothesis needs to be tested in a clinical trial with randomized allocation of these patients to one or the other treatment group.
A limitation of this study is the number of subjects. Therefore, we propose to categorize our results as a proof-of-principle which should be replicated in a larger group of patients. Another limitation is the lack of a healthy control group. Results obtained in such a control group are necessary for interpretation of the magnitude of AO-induced MEP facilitation in stroke patients. A third limitation consists of our control condition, which only showed a static hand. In order to identify the relevance of the kinematic aspect, another control condition could be to show moving lines with identical kinematics of the pinch grip movements.
The only other study employing TMS in an AO experiment with stroke patients addressed a different issue. In that study, TMS was used to test (i) whether AO and physical exercise induced a longer lasting motor memory formation than physical exercise alone; and (ii) whether corticospinal excitability changes (20). The authors reported that excitability changes occurred after AO and exercise in favour of the agonist muscle.
In conclusion, this study indicates that AO enhances motor excitability in stroke patients. One might conclude that a relevant prerequisite for an effective AO training for improvement of motor functions is fulfilled. Since the excitability increase was stronger for the hand that was observed in the video, this aspect of congruency might be a relevant detail when employing AO as a treatment strategy. However, analysis of individual patients indicated that some of them did not develop a motor excitability increase during AO. Therefore, further studies are needed to determine the correlation between AO-induced motor excitability changes and the clinical effectiveness of AO. It would be of particular interest to determine whether patients with and without motor excitability increases during AO differ in their ability to benefit from AO.
References

