Kate Sansam, MD, MRCP1, Rory J. O’Connor, MD, FRCP1,2, Vera Neumann, MD, FRCP1 and Bipin Bhakta, MD, FRCP1,2
From the 1Academic Department of Rehabilitation Medicine, University of Leeds and 2Leeds Teaching Hospitals NHS Trust, Leeds, UK
OBJECTIVE: Decision making within amputee rehabilitation includes the assessment of whether a patient is suitable for a prosthesis and if so, what components to provide. This study seeks to increase understanding about clinicians’ perspectives on what factors influence these decisions.
Method: One-to-one semi-structured interviews were completed with 23 experienced clinicians at their place of work at 4 UK amputee rehabilitation centres. Thematic analysis using a theoretical, semantic approach was used to identify key themes from the data.
RESULTS: Four key themes were identified: estimating outcome; difficulties predicting outcome; patient choice and barriers to prescribing. There was variation in the importance placed on each theme between individual clinicians and services, with factors such as budget and risk aversion acting as barriers to prescribing. Only one of the 4 centres used formal prescribing guidelines.
CONCLUSION: The results highlight the difficulties clinicians experience in estimating outcome and suggest inequity of prosthetic provision in the UK, with variation in the provision of high cost items. The development of national prescription guidelines is suggested to improve equality of prosthetic provision.
Key words: lower limb amputation; prosthetic; decision making.
J Rehabil Med 2014; 46: 00–00
Guarantor’s address: Dr Kate Sansam, Academic Department of Rehabilitation Medicine, Faculty of Medicine and Health, University of Leeds, Level D, Martin Wing, Leeds General Infirmary, Great George Street, Leeds LS1 3EX, UK. E-mail: katesansam@hotmail.com
Accepted Dec 16, 2013; Epub ahead of print Feb 28, 2014
Introduction
There are two key decisions made during rehabilitation following lower limb amputation. Firstly, whether to prescribe a prosthesis, and secondly, if a prosthesis is to be provided, the type of prosthetic limb selected.
The majority of prosthetic limbs are modular (1) with an endo-skeletal structure and selection of foot and knee components. How components are chosen differs between countries. In the US, the Medicare Functional Classification Level (MFCL) (2), which classifies actual, or potential, ability to mobilise with a prosthesis, is used by Medicare and many third-party health care funders to select components. In other countries, including the UK, the process whereby an individual’s prosthetic prescription is determined is generally influenced by the clinical observations, training and experience of the treating team.
In the UK National Health Service (NHS) most amputee rehabilitation takes place as an outpatient. Most patients will initially see a physiotherapist and, if able, start to mobilise using an early walking aid (EWA). This is an assistive device used within physiotherapy sessions. For transtibial amputees this may be a Pneumatic Post-Amputation Mobility aid (PPAM aid) (3) or Amputee Mobility Aid (AMA) (4). The PPAM aid is also used for transfemoral amputees, as is the Femurett (5). Both the AMA and the Femurett are articulated at the knee level. The Femurett can be used with the articulation locked or free. Rarely, an evaluation prosthesis will be made to decide whether to proceed to a definitive prosthesis, but in the UK these are generally reserved for patients unable to use an EWA, such as after hip disarticulation.
The decision whether to proceed to a definitive prosthesis is usually made by the patient and multidisciplinary team (MDT) at a single assessment appointment at one of 43 NHS amputee rehabilitation centres. The MDT, generally comprising a rehabilitation physician, physiotherapist, prosthetist and specialist nurse, have the relevant background information on the patient including the outcome of initial gait retraining. Other professions, such as occupational therapist and psychologist, may also be involved depending on patient needs and staffing complement of the service.
Traditionally in the UK formulation of the prosthetic prescription was the responsibility of the rehabilitation doctor, with input from other MDT members. However, more recently, independent prosthetic prescribing rights were extended in many services to prosthetists and occasionally other professionals. Different components may be trialled before a final decision is made, but this is not the norm and is more common in subsequent rather than first prostheses. Provision of further prostheses is not time dependent, but is based on clinical need, such as when the first prosthesis no longer meets the patient’s requirements or is beyond economic repair.
There are several national (6, 7) and international guidelines (8, 9) on amputee rehabilitation. Although they all include the need for a patient centred, multidisciplinary assessment to establish each individual’s needs and goals, they do not specify how the decision of whether to provide a prosthesis or what components to choose should be made.
Two research groups have investigated prosthetic prescription. A Dutch group performed a multicentre observational study of lower limb prosthetic prescription (10), interviewed 11 clinicians (11) and conducted a Delphi study to develop prescription guidelines (12). They reported that activity level was an important factor when prescribing a prosthesis, but did not examine how this was established. No clear association between actual or predicted activity levels and components prescribed was found and there was little agreement in component choice between clinicians.
An Irish group held patient focus groups and interviews with clinicians to identify important outcomes of prosthetic provision (13, 14). They found that clinicians viewed successful outcome as achieving the level of mobility predicted by them during initial clinic visits and that this prediction influenced prescription. Although they did not describe how this potential was established, they identified patient attributes considered predictive, such as age and comorbidities, most of which have been described in previous studies (15). This group also used the Delphi technique to create consensus on the most important outcomes, predictors and facilitators of prosthetic prescription and use (16). There was agreement on the importance of 19 predictive factors: 12 physical, such as decline due to age and illness, and 7 psychosocial, such as motivation.
Both groups considered new and established prosthetic users together and did not examine the initial decision of whether a limb should be provided.
This study aims to deepen understanding of how clinicians decide whether a prosthesis is suitable and what components to choose for the first prosthesis. Detailed consideration of the merits of specific components, however, is beyond the scope of this study.
Methods
This was a qualitative study with ethical approval granted by Leeds (East) Research Ethics Committee. Local collaborators at 4 NHS amputee rehabilitation centres identified suitable doctors, prosthetists and physiotherapists with expertise in amputee rehabilitation. Using a stratified sampling matrix clinicians were invited to participate via email or letter. A purposive sampling strategy ensured all 3 professions were represented at each centre to enable comparison of different services and professional groups. Centres were selected to be broadly representative of the range of UK services covering sufficiently large populations (all seeing more than 90 new patients a year) to ensure a number of health professionals, from which potential participants could be drawn, worked at each centre.
Only one clinician who was approached declined to participate due to insufficient time. Participants completed a questionnaire regarding their experience in amputee rehabilitation prior to the semi-structured interview that was conducted on a one-to-one basis at their place of work by a single interviewer (KS) to ensure consistency. Interview content was led by a topic guide (Table I) with new topics introduced by participants discussed as and when they arose.
|
Table I. Interview topic guide |
|
• How do you decide what to do with someone after a lower limb amputation? • What do you define as success after prosthetic rehabilitation? • What factors are important to predict successful use of a lower limb prosthesis? • What factors are considered when deciding whether to mobilise someone with an early walking aid, which aids are used and how are they used? • What factors are considered when assessing a patient for suitability for a first prosthesis after lower limb amputation? • How is the decision made regarding what prosthetic components are used? • Under what circumstances is free-knee use unsafe or clinically inappropriate after above knee amputation? • How would you assess learning ability in relation to prosthetic rehabilitation? |
Interviews lasted between 20 and 70 min and were audio-recorded with the participants’ consent and transcribed verbatim. Transcripts were verified for accuracy by the interviewer prior to analysis which occurred concurrent with data collection. Thematic analysis using a theoretical, semantic approach (17) was used to analyse the data (Fig. 1).
Coding and data organisation was assisted by NVIVO version 8 software. All transcripts were coded by the interviewer and the first 3 transcripts were coded separately by a second researcher (ROC). Potential themes and thematic structure were discussed with the whole research team to resolve discrepancies and ensure reliability. As well as analysing the whole data set, transcripts were also examined in subgroups to compare and contrast responses from different services and professional groups.
Recruitment to the study continued until data saturation (18, 19) was achieved. This was defined as the point at which new interviews were only confirming existing categories and no new themes were being identified.
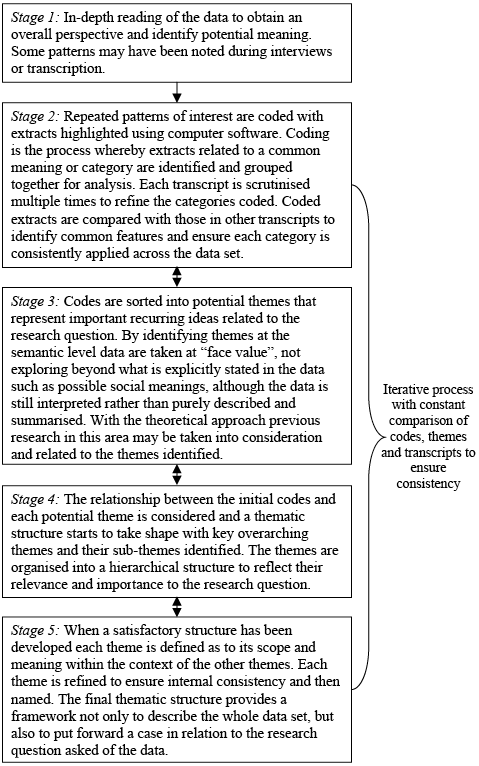
Fig. 1. Stages of analysis.
Results
Twenty-three experienced clinicians were interviewed between April 2008 and January 2010. Participants had worked in amputee rehabilitation for a mean of 18 years (range 2–36 years) and worked a mean of 26.9 h a week in the field (range 5–50 h). The distribution of professions by centre is shown in Table II.
|
Table II. Participant recruitment at each site |
||||
|
Profession |
Centre |
|||
|
01 |
02 |
03 |
04 |
|
|
Physiotherapists |
2 |
1 |
1 |
3 |
|
Prosthetists |
2 |
2 |
3 |
4 |
|
Doctors |
2 |
1 |
1 |
1 |
At the time of the study, centres 01 and 03 used the traditional model of prosthetic prescribing by the consultant rehabilitation physician, whereas in the other two centres, the prosthetists had also adopted a prescriber role.
Four key themes were identified (Fig. 2), each having several subthemes as shown in Table III.
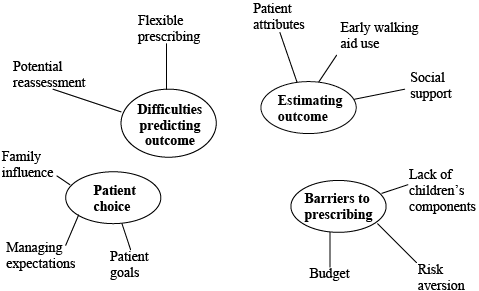
Fig. 2. Key themes identified in analysis.
|
Table III. Key themes identified in analysis with illustrative quotes |
|
|
Theme |
Subthemes and illustrative quotes |
|
Estimating outcome |
Patient attributes “People who are, sort of, well motivated and can cope with things happening in their life, even before amputation, they will use those qualities to get through losing a leg and their rehab” |
|
Early walking aid use “if they can’t stand and walk in a Femurett then they’re not going to stand and get a benefit functionally from a prosthesis” |
|
|
Social support “if they didn’t have all that support at home and they were borderline they may be less likely to have a prosthesis” |
|
|
Difficulties predicting outcome |
Potential reassessment “by the time they [patients] actually leave hospital, have a bit of proper food and start to get their diabetes under better control you might... see a different picture rather than what you saw at a very early stage” |
|
Flexible prescribing “Sometimes what we do is when there’s a doubtful case we’ll provide people with a free-knee with the optional lock… so they have an option of to use it free, and in certain situations where they feel that they might not be able to manage… they can lock it” |
|
|
Patient choice |
Family influence “If their parents express frustration or dissatisfaction with the limb the child is likely to pick that up… They may be less prepared to wear the leg, or maybe much more conscious of it“ |
|
Managing expectations “They’ve read newspaper articles, they’ve looked on the internet and their expectations are way up here. And I feel guilty because sometimes that first visit to me is ‘Well hang on… this is what’s possible now, this may be possible in the future’” |
|
|
Patient goals “We have to make sure that we do sit down and try and discuss goals with patients and not lead them… And not try and push people into limb wearing just because ‘you can do it, it’s great!’” |
|
|
Barriers to prescribing |
Budget “I guess as a prosthetist I don’t really want to care about the budget if I’m honest, but as a realist we are spending tax payers’ money so we can’t just go giving out stuff willy nilly.” |
|
Risk aversion “if someone is not able to understand how to put the prosthesis on and off and we think they’re a risk to themselves, or to others, then they wouldn’t get a limb.” |
|
|
Lack of children’s components “the variety available for children is a lot less than what’s available for adults and I think that is because they don’t put the research into it” |
|
Estimating outcome
In all centres, new patients were assessed by several MDT members, either simultaneously, or more commonly, sequentially. In order to decide if a patient would benefit from prosthetic rehabilitation and what components to prescribe, participants described respectively estimating their potential to learn to use a prosthesis and the level of mobility they were likely to achieve.
Estimated mobility outcome was used to select components and was usually based on matching clinicians’ previous experience of components to the needs of the patient. Centre 04 had a more formal approach using locally agreed prescription guidelines. These were devised by the MDT by evaluating available components and choosing the most cost effective ones for given predicted mobility levels and needs.
Three subthemes were identified as influencing participants’ estimation of outcome: patient attributes, early walking aid use and social support.
Patient attributes. The majority of participants described assessing patients using the traditional history taking and examination skills. The patient attributes they considered when predicting mobility outcome are presented in Fig. 3 in a structure based on the International Classification of Functioning, Disability and Health (ICF) (20). No participants explicitly discussed using the ICF in their approach to patient assessment, but several emphasised the importance of considering participation, not just mobility. Although formal outcome assessment tools such as the Amputee Mobility Predictor (21) exist, none of the participants used these, preferring to rely on their own clinical judgement.
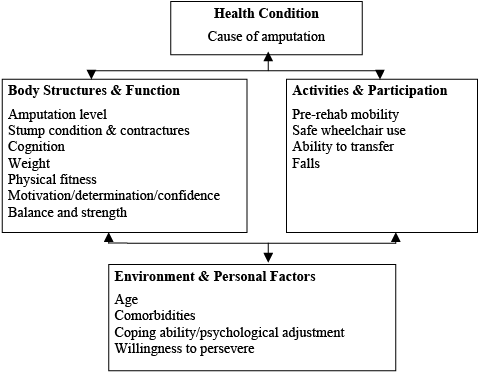
Fig. 3. Patient attributes thought to influence outcome by participants.
Participants placed great importance on the influence of factors which are not easily objectively measured such as motivation, determination and coping ability, which have not been investigated in detail in the literature.
There was general agreement that, apart from in extreme circumstances, every child with a lower limb amputation would be offered a prosthesis as they tend to progress well in rehabilitation. Several participants reflected on the limitations of assessing potential in children as they are more easily distracted, do not always cooperate with the process and most are too small to use an early walking aid.
Early walking aid use. In all centres EWAs were primarily employed therapeutically as part of gait retraining. The ability to use an EWA was seen as a proxy measure of likely ability to use a prosthesis and given considerable weight when deciding appropriateness of prosthetic provision. EWA use was seen as the domain of physiotherapists who communicated patients’ progress to the MDT. This information was generally based on EWA use over several therapy sessions prior to the MDT assessment, but occasionally other professionals would also observe the patient using an EWA in the MDT assessment to aid their decision.
EWAs were also used to estimate future activity levels by enabling assessment of characteristics difficult to evaluate by other means, such as dynamic balance, exercise tolerance and confidence. For transfemoral amputees, clinicians at 3 of the centres felt that patients able to use the Femurett with the knee articulation unlocked were likely to be prescribed a free-knee component and that if possible, patients should use a free-knee at the earliest opportunity to prevent development of compensatory gait deviations. However, clinicians at centre 04 shared a different ethos, reflecting the lack of research in this area. They felt the majority of transfemoral patients should be given a locked-knee to establish independent mobility earlier and then, depending on their progress, a free-knee could be considered at a later stage. This was felt particularly appropriate for older patients with vascular disease who may have a short life expectancy. At this centre, clinicians were also generally more critical of the Femurett, describing the knee mechanism as “crude” and that its use was not a good reflection of future use of a free-knee prosthesis.
Social support. For patients estimated to have borderline ability to use a prosthesis independently, the level of their social support was seen by some as a deciding factor on whether they were prescribed a prosthesis. This was considered particularly relevant for patients with cognitive impairment that may affect their ability to don and doff the prosthesis independently.
Difficulties predicting outcome
Most participants felt that accurately predicting outcome was difficult, particularly for transfemoral amputees. Many reported difficulty assessing baseline predictive factors that could not be objectively measured, such as motivation. Participants described having to speculate about these traits based on their general impression of the patient and reports from other MDT members. They also reflected that information gathered from the patient may not be accurate due to recall difficulties or the patient’s desire to “pass” the assessment. Concern was also expressed about the reliance on a single assessment appointment as it was felt that performance on that day could be influenced by transient features such as infections.
Clinicians working at centre 04 appeared more confident estimating outcome than the other centres, although still recognised that this was imperfect. This centre differed from the others by formally predicting mobility grades to choose components using their local prescription guidelines. They had also previously compared predicted and achieved grades and felt that this had enabled them to adjust their predictions and improve accuracy.
To address the uncertainty in predicting outcome, two strategies were commonly described: potential reassessment and flexible prescribing.
Potential reassessment.Throughout the different stages of amputee rehabilitation, participants emphasised that no decision was final, patients’ abilities could change, and the possibility of further assessment was required to address this uncertainty.
The potential for reassessment was felt to be particularly useful in determining the correct knee component for transfemoral amputees. Many clinicians felt that often patients required a semi-automatic knee unit in the initial stages and once established on this, could be reassessed for a free-knee if they wished.
Flexible prescribing. Another strategy for managing uncertainty of future mobility was the use of hardware systems and components that could be adapted if the patient achieved a different level than anticipated. This was seen as particularly useful in transfemoral amputees for whom there was doubt whether they would be able to safely use a free-knee. Many clinicians advocated the use of hand-operated knee locks for these individuals for flexibility to use the knee locked or free, either as they progress through rehabilitation or in different environments.
It was also felt that the use of pyramid systems allowed flexibility, enabling components to be easily changed if the individual achieved a different activity level than anticipated.
Patient choice
Most participants stated that clinical decisions should be made in collaboration with the patient. Although clinicians ultimately decided if prosthetic provision was appropriate, there was recognition that patients had the autonomy to decline this. There was a prevalent view that not all patients would benefit from a prosthesis with some having more independent function using a wheelchair.
When it was decided that an individual was suitable for a prosthesis, the mechanical component choice for their first prosthesis was generally made by the treating clinicians. Many participants described teaching patients about components to enable them to be more involved in future component choice.
In contrast to the choice of mechanical components, most participants described routinely involving patients in choice of cosmesis, possibly because the difference between cosmetic covers is easier to explain in non-technical language than the variety of mechanical components available.
Patient choice was felt to be mediated by 3 factors: influence of family members, clinicians’ management of patient’s expectations and patient directed goals.
Family influence. Family influence was seen as potentially beneficial, providing social support and advocacy for patients, but could have negative effects at times. Several participants recalled instances where family members had put undue pressure on a patient to persist with prosthetic rehabilitation when the patient and treating clinician felt that wheelchair mobility was preferable.
The influence of family members was most prominent when participants were talking about child amputees where it was seen as imperative that parents were happy with the prosthesis as their view could influence the child’s attitude to and use of it.
Managing expectations. The need to manage expectations and inform patients of their anticipated outcome was a prevalent theme. This was seen as essential to maximise patients’ involvement in the decision making process. Patients were perceived as commonly having unrealistically high expectations about what a prosthesis could do for them, mistakenly believing that components determined ability to walk rather than this being largely related to their own physical abilities.
Many participants felt the availability of information in the media had contributed to increased unrealistic expectations. They commented that the portrayal of amputees, such as “celebrity amputees” and war veterans, used individuals not representative of the majority, who are generally older adults with vascular disease and unlikely to achieve the same mobility level.
Although participants felt it was necessary to address patients’ unrealistic expectations this was seen as a negative aspect of their role.
Patient goals. Although patients were not usually involved in choosing components for their first definitive prosthesis, many participants reported considering the patient’s functional and participatory goals when formulating the prescription. For the goal to influence component choice, it needed to be seen as achievable by the clinician, primarily by matching the goal to their predicted mobility.
Barriers to prescribing
To make these clinical decisions, participants described balancing their estimation of walking potential with patients’ preferences as described above. However, there were also specific barriers to provision of a prosthesis and certain components that took priority over other factors in the decision making processes. These broadly fell into three categories of budget, risk aversion and lack of children’s components.
Budget. Finite departmental budget was perceived as a significant barrier to prescribing high cost components. No centre was able to provide the most expensive components on the market, such as certain microprocessor-controlled knee units, and the majority did not provide bespoke silicone cosmetic covers. There was general agreement that all patients thought appropriate for prosthetic provision were provided with a limb broadly meeting their needs, although not always to the optimum level possible with more expensive componentry.
As most of the physiotherapists were not directly involved in component choice, they did not feel that budget played a significant part in their clinical decisions. Some expressed relief that their role did not require this of them. Many prosthetists and doctors felt reluctant to consider cost when formulating prescriptions, but reflected that this was necessary to ensure sufficient resources to provide limbs to all patients needing them.
To ration resources, participants described reserving higher cost components for people with specific needs justifying this additional expense. Higher cost cosmetic covers, such as silicone, were not offered routinely at any of the centres, but would be discussed with patients who specifically asked or expressed dissatisfaction in the aesthetics of their prosthesis.
Risk aversion. Perceived risk of injury was the commonest barrier to provision of limbs and the use of certain components, such as free-knees. Transfemoral amputation was seen as carrying additional risk of falling compared to transtibial, as the knee had to be positioned correctly to lock or ensure sufficient stability to weight bear. For transfemoral amputees in whom safe free-knee use was uncertain, risk was an important factor for many clinicians in opting for a locked-knee.
Lack of children’s components. The decision regarding components for children’s prostheses differed from adults, partly due to lack of choice. Many participants expressed frustration over the limited range of children’s components, which they felt was due manufacturers’ reluctance to invest in research and development in this small market, owing to potential poor financial returns.
Although presented separately, participants described considering the themes in combination when making decisions. The importance assigned to each theme differed between participants, but there was greater similarity between responses from clinicians at the same centre than from clinicians at different centres. In particular centre 04 had a different approach, placing more emphasis on estimating outcome, although less on the subtheme of early walking aid use, with predicted outcome guiding component choice using formal local guidelines. Even though the role of the three professions was comparable at all centres this trend persisted when clinicians of the same profession were compared. This indicates a similar approach by clinicians at the same centre, reflecting the team nature of these decisions and likely influence of local culture.
Discussion
This study identified 4 key themes considered important by clinicians making decisions regarding prosthetic prescription: estimated outcome, difficulties predicting outcome, patient choice and barriers to prescribing. In common with previous research (11, 14) estimating outcome was a key factor in prosthetic prescription with similar predictive patient attributes and consideration of social support. This is the first study, however, to focus on the decision of whether to provide a prosthesis for new amputees and to describe the use of EWAs in predicting outcome.
The physical factors described were similar to those previously investigated for their ability to predict mobility after amputation (15, 16). However, there has been little previous research on the predictive ability of some of the psychological factors considered important by participants, such as motivation and determination, possibly because they are challenging to measure objectively. Indeed motivation has been previously highlighted in the rehabilitation literature as something commonly believed to influence outcome (22), but poorly defined (23) and rated (24) by clinicians.
The patient attributes described by participants fitted well into an ICF structure, although none of the participants mentioned using this framework. The use of the ICF may become more explicit when the core sets for persons after amputation (25) are complete.
This study has certain limitations. By using interviews it reflects clinicians’ perception of how they make these decisions which may deviate from actual practice. Most clinicians’ description of their approach to decision making in this study reflect national (6) and international guidance (8, 9) on the need for person-centred multidisciplinary assessment, but further research using observed practice is needed to confirm this. Caution should be applied however, as the very act of observing practice may also influence it. As this study only interviewed clinicians, it was not possible to capture patients’ perspectives. Other professional groups, such as occupational therapists, psychologists and nurses were not included as they are not represented at all NHS centres and are not commonly responsible for these decisions. Given that all 4 key themes were shared by the different professional groups interviewed it is likely that these are also themes considered by other groups, although the emphasis they place on each may differ.
The qualitative analysis would have been enhanced if it had been possible for all transcripts to be coded and analysed by more than one researcher to minimise bias. As the objective was to explore clinicians’ perceptions, it was decided that participant observation and written questionnaires would not gather sufficient depth of information and that spoken data was required. Individual interviews were chosen over focus groups as, although they take longer to complete, potentially sensitive information is more likely to be disclosed in a confidential environment. It is also possible for focus groups to be influenced by the social hierarchy of the group or dominated by a small number whose opinions are not representative of the majority. Individual interviews are also less disruptive to a service as they can more easily be arranged around clinical commitments. Further research including more than one qualitative data source, such as focus groups or observed practice, to triangulate the results would increase the credibility and validity of these findings.
By interviewing clinicians at multiple centres it was hoped to allow generalisable conclusions to be drawn from the findings, and indeed all 4 key themes were identified at all centres. The centres chosen are likely to be representative of other UK amputee rehabilitation services, but given the variation in funding streams in other countries it is likely that the themes of patient choice and barriers to prescribing would differ from those in the NHS. In systems where patients self-fund prostheses it is likely that they have greater involvement in the decision making processes.
Disentangling the four key themes may lead to greater transparency in how these decisions are made and improve patients’ and clinicians’ understanding of the assessment process. The findings suggest inequality in prosthetic provision in the NHS with variation in the provision of high cost items. The financial barriers to prescribing could be explored further and consideration given to the development of national prescription guidelines, taking into account the cost-benefit of components to reduce the occurrence of “postcode prescribing”. This study shows that clinicians do not purely consider predicted mobility when making these decisions, placing importance on other aspects such as social support and risk management. We would therefore argue that in contrast to established prescription guidelines, such as the MFCL, future guideline development should endeavour to include all key themes identified in this research in the formulation of more comprehensive clinical algorithms to guide prescription.
Acknowledgements
The authors would like to express their gratitude to all those who kindly participated in this study. This study was funded by The Meningitis Trust, who had no influence on the interpretation of the data and conclusions drawn.
References

