Mandana Fallahpour, RegOT, PhD1,2, Anders Kottorp, RegOT, PhD1, Louise Nygård, RegOT, PhD1 and Maria Larsson Lund, RegOT, PhD2
From the 1Department of Neurobiology, Care Sciences and Society, Division of Occupational Therapy, Karolinska Institutet, Stockholm and 2Department of Health Sciences, Luleå University of Technology, Luleå, Sweden
OBJECTIVE: To compare the perceived difficulty in use of everyday technology in persons with acquired brain injury with different levels of severity of disability with that of controls.
METHODS: This comparison study recruited 2 samples of persons with acquired brain injury and controls, comprising a total of 161 participants, age range 18–64 years. The long and short versions of the Everyday Technology Use Questionnaire and the Extended Glasgow Outcome Scale were used to evaluate participants.
RESULTS: Persons with acquired brain injury demonstrated lower mean levels of perceived ability in use of everyday technology than controls (F = 21.84, degrees of freedom = 1, p < 0.001). Further analysis showed a statistically significant mean difference in perceived difficulty in use of everyday technology between persons with severe disability and good recovery, between persons with severe disability and controls, and between persons with moderate disability and controls. No significant mean difference was found between persons with severe disability and moderate disability, between persons with moderate disability and good recovery, and between persons with good recovery and controls.
CONCLUSION: Perceived difficulty in using everyday technology is significantly increased among persons with acquired brain injury with severe to moderate disability compared with controls. Rehabilitation services should consider the use of everyday technology in order to increase participation in everyday activities after acquired brain injury.
Key words: acquired brain injury; everyday technology; rehabilitation.
J Rehabil Med 2014; 46: 635–641
Correspondence address: Mandana Fallahpour, Karolinska Institutet, Department of Neurobiology, Care Sciences and Society, Division of Occupational Therapy, Box 23200, SE-141 83 Huddinge, Stockholm, Sweden. E-mail: Mandana.Fallahpour@ki.se
Accepted Feb 18, 2014; Epub ahead of print Jun 17, 2014
INTRODUCTION
Acquired brain injury (ABI) encompasses a wide spectrum of brain injuries that include traumatic and non-traumatic aetiologies (e.g. traumatic brain injuries (TBI), and cerebrovascular accident) (1–3) and is a serious health problem (4–6). ABI leads to complex physical, cognitive and psychological impairments (7, 8) with a wide variation in severity (6, 9). Cognitive impairments, for example, problems with memory, attention, concentration and delay in information processing, are often the most prominent (1). Impaired self-awareness has also been identified as a common problem (10, 11). The severity of disability after ABI, referring to limitations in activity and participation, can be classified into 3 main categories: severe disability (SD), moderate disability (MD) and good recovery (GR) (6). Persons with ABI experience restricted participation in various everyday activities, such as self-care and instrumental activities of daily living, leisure, social activities and work (12–16), which in turn dramatically impact on the individuals’ perceived life satisfaction (17). Individuals with ABI might also experience difficulties in using everyday technology (ET), which is an essential pre-requisite for participation in various everyday activities at home and in society (18, 19).
ET refers to a variety of electronic, technical and mechanical equipment existing in people’s everyday lives, such as electronic household equipment, mobile phones and computers, including both newly developed and common well-known, technological artefacts and services (20). The increasing growth in ET is obvious in many services in Western society (20). ET is commonly considered an environmental facilitator, having the potential to facilitate participation in everyday life, as well as make daily life easier and more efficient. However, most ETs have been designed for individuals with no disabilities (19). It is therefore essential when investigating ET use among people with disabilities, such as after ABI, to investigate whether the severity of disability is related to difficulties in the use of ET. Previous research has revealed that even people without disabilities have perceived difficulties in the use of ET (21). It is assumed, therefore, that after disabilities such as ABI, individuals might perceive even more challenges, significantly hindering their participation; consequently, as all people may have difficulties in the use of ET, knowledge is needed about whether difficulties differ between those with and without ABI. Recent empirical studies focusing on ET have shown that people with cognitive impairments (22), ABI (18, 23) and intellectual disabilities (24) have difficulties in using ET. Nevertheless, empirical knowledge regarding the use of ET among persons with ABI is limited. There are only a few studies in this area, which are qualitative studies with small samples (18, 23, 25, 26). An empirical study (18) has indicated that a majority of the sample of persons with ABI reported difficulties using ET. The most common difficulties were reported in relation to telecommunication and computers. That study also demonstrated that the participants perceived that their difficulties in using ET influenced their everyday activities and their possibility to participate at home and in the community (18). However, that study included only 36 persons with ABI, and did not include any comparison of findings with healthy controls . Thus, further research is required into this area. Firstly, difficulties in ET use after ABI have not been empirically studied in comparison with healthy controls. It is assumed that there might be a difference between these 2 populations that can be taken as a hypothesis that needs to be empirically confirmed. Secondly, no study has examined whether the perceived difficulty in use of ET might differ among persons with ABI with different levels of severity of disability and, if it differs, to what extent. Thirdly, difficulties in ET use have not been studied in larger samples of working age individuals.
To sum up, it is essential to investigate individuals’ perception of difficulty in use of ET during participation in everyday activities at home, at work and in society after ABI. The overall aim of this study was to compare the perceived difficulty in use of ET in persons with ABI with different levels of severity of disability and controls.
METHODS
Participants and design
The study was designed as a cross-sectional comparison study between persons with ABI and controls. A total of 161 participants were included in the study. Participants’ characteristics are shown in Table I. Two participant samples were recruited; persons with ABI and controls, which included adults with no ABI or other known impairments. Participants with ABI were selected from a database of clients of a rehabilitation medicine clinic. All the clients in their database during the period 2003–2010 who met the inclusion criteria were included in the sampling. Inclusion criteria for the ABI group were: (i) having a diagnosis of ABI; (ii) working age (18–64 years); (iii) living in 1 of 2 municipalities that the study was performed in; (iv) not having aphasia; and (v) not having other conditions or diseases, e.g. dementia.
In accordance with ethical guidelines, written information about the study was sent to the identified participants. They were asked to provide written consent to participate in the study. Subjects who did not respond to the request were contacted by telephone to ensure that no volunteers were missed. Of the 215 clients in the database who fulfilled the inclusion criteria, 81 agreed to participate in the study. Of the remaining, 91 declined and 43 did not respond.
Controls were selected by choice of convenience, using a snowball sampling technique. In order to enhance the representativeness of this sample and capture a variety of experiences of using ET, recruitment of participants focused on including people from different areas (e.g. urban, rural and suburban), of different ages, with different jobs and varied marital status. During the recruitment process, before the data collection started, individuals were asked if they had any functional limitation or diagnosis, to ensure that they did not have any known impairments. They received written information about the study in accordance with ethical guidelines, including that their data would be compared with those with disabilities, before they gave their written informed consent to participate in the study.
The study was approved by the Regional Board of Research Ethics at Umeå University, Sweden (UmU Dnr 2010-235-31).
Instruments and procedures
Data collection for persons with ABI was carried out by 3 registered occupational therapists, each of whom had more than 10 years of experience of providing rehabilitation services for this group of clients. For controls, data were collected by occupational therapy (OT) students during the last semester of their Bachelor level education. Through the course that was held by the third author (LN), all data collectors were educated on how to administer and score the Everyday Technology Use Questionnaire (ETUQ) (27, 28) and its short version S-ETUQ (28, 29) to assess perceived difficulty in ET use, as well as how to collect demographic data. They also had the opportunity to receive guidance and feedback from the instrument developers (LN, AK) during the data collection process. Data were collected in the participants’ homes or other places of their choice and began with questions about socio-demographic variables. Thereafter, the ETUQ or S-ETUQ interviews were conducted. Finally, those with ABI were assessed with the Extended Glasgow Outcome Scale (GOS-E) (30).
Everyday Technology Use Questionnaire. The ETUQ (27, 28) was used to collect information regarding perceived difficulty in using ET in the controls based on a standardized interview (31). This questionnaire was originally designed to investigate the extent to which older adults with cognitive limitations can use the ET that is of relevance to them (27). The instrument does not focus on the reasons for the difficulties, but rather the extent to which persons perceive difficulty in using ET. According to the ETUQ manual (28), there is no limitation in using this instrument for individuals with physical limitations (e.g. paralysis). The ETUQ includes questions about ET that people commonly encounter in their everyday lives (28). The full version comprises 92 items divided into 8 areas that cover questions of artefacts and services in: (i) household activities; (ii) activities in the home; (iii) personal care; (iv) power tools; (v) accessibility; (vi) computer and telecommunications; (vii) economy and shopping; and (viii) transportation. As the study sample was of working age, a work domain was added including 10 items regarding work as the ninth area of the ETUQ. The data collectors were trained to keep the interview focused on whether the participants used or did not use the different technological artefacts and services in the ETUQ, and the extent to which certain technologies caused difficulties or efforts (28). In addition, they were trained to ask follow-up questions to ensure the validity of the participants’ responses. Participants were first asked if an item was relevant for them. According to the ETUQ manual, objects and services that are not available or applicable for the respondent are rated as “not relevant”. In case an item was familiar to the person, but still not in use, it was scored as “not relevant” (28). If it was relevant, a 5-category rating scale was applied as a guide to evaluate the level of perceived difficulty in using each item. Items/everyday technologies that were not relevant to the participant were not scored. More information about the instrument and the scoring is found elsewhere (22, 27, 28). As this study was only a part of a project including a larger data collection, the S-ETUQ (28, 29) was chosen for those with ABI in order not to exhaust them. The S-ETUQ comprises 32 items from 7 of the original 8 areas, covering ETs from easy to difficult, and was applied in the same way as the ETUQ. It was developed using a Rasch analysis, and previous research has shown that the 32-item S-ETUQ generates statistically similar measures to the original 92-item version for the majority of the study sample (93.2%) (29).The psychometric properties of both the ETUQ and S-ETUQ have been evaluated and found to be promising for use with older adults with cognitive impairment (mild cognitive impairment (MCI), dementia, Alzheimer’s), adults with intellectual disabilities, and older adults with no cognitive impairments (24, 27, 29, 32).
Extended Glasgow Outcome Scale. The GOS-E (33) was applied for persons with ABI in the study, as a widely used outcome measure after brain injury to assess severity of disability through a structured interview. The GOS-E reflects disability and handicap and focuses on how the injury has affected functioning in major areas of life. The items of this hierarchical scale include 8 questions regarding: (Q1) vegetative state; (Q2) independence in the home; (Q3) shopping; (Q4) travel: independence outside the home; (Q5) work; (Q6) social and leisure activities; (Q7) family and friendship; and (Q8) return to normal life. The assessment allocates individuals with ABI into 3 main outcome categories: (i) SD, (ii) MD, and (iii) GR (33), based on the answers to these questions. The first 2 questions (Q1 and Q2), covering individuals who were deceased or in a vegetative state of disability, were not relevant for this study. The first category, lower and upper SD (Q3 and Q4), includes individuals who are dependent on assistance. The second category, lower and upper MD (Q5 and Q6), includes individuals who are independent in activities of daily life, but are not able to resume their previous capacity for work, leisure and social activities. Finally, the third category, lower and upper GR (Q7 and Q8), includes individuals who have no, or minor, problems in daily life compared with before ABI (33). This instrument has been found to be psychometrically reliable (33) and valid for use with persons with head injuries (34).
Data analysis
Data analysis was performed in 2 steps, as follows:
Preparatory analysis. At the beginning of the first step in data analysis, an application of Rasch analysis (35) was used to transform the ordinal raw scores from both versions of the ETUQ into interval measures using the Winsteps computer programme, version 3.63.0 (http://www.winsteps.com), which converts the raw item scores from a test or questionnaire into equal-interval measures through logarithmic transformations. These transformations produce an estimation of personal ability measures along the continuum of the construct being measured (35), perceived difficulty in ET use. Furthermore, Rasch analysis makes it possible to combine items from the ETUQ and S-ETUQ into a single analysis to examine psychometric properties; it is also possible to compare the Rasch-generated person measures from these instruments after transforming the raw data into interval measures. Although the psychometric properties of both the long and short versions of the ETUQ have supported aspects of validity for different clinical samples (24, 27, 29, 32), an initial analysis of the validity of the response patterns among the participants was conducted in this study. The criteria for acceptable goodness-of-fit for both items and persons were set at a mean-square (MnSq) ≤ 1.4 (36) with an associated standardized z < 2.0 (37).
Furthermore, descriptive statistics were applied in the study to describe the characteristics of the participants. In this step of the analysis, persons with ABI (n = 81) and controls (n = 80) were compared in terms of demographic variables, such as age, sex, educational level, and occupational groups, since the use of ET might vary with these variables. For this purpose, a t-test analysis was used to compare the 2 samples with respect to age and a χ2 test analysis was used to compare the 2 samples with respect to gender, educational level and occupational groups. The results of the χ2 test indicated no statistically significant difference between them in the variables gender (χ2 = 1.044; degrees of freedom (df) = 1; p = 0.307), educational level (χ2 = 0.952; df = 2; p = 0.621), and occupational groups (χ2 = 0.084; df = 2; p = 0.959). However, since there was a significant difference between mean ages in 2 samples (F = 33.321; df = 159; p < 0.001), they were matched for age and gender to control for these factors as the possible confounders before comparing the perceived difficulty in ET use between the 2 samples. This matching approach decreased the number of total participants from 161 to 115 individuals (63 ABI; 52 controls). To ensure that there were no differences between the 2 groups in the sample after matching, the same analyses were used to compare the 2 groups with respect to age, gender, educational level and occupational group.
Main analysis. In the second step of the main analysis, the perceived difficulty in ET use between persons with ABI and controls was compared using one-way analysis of variance (ANOVA). To compare the perceived difficulty in ET use between the 2 samples, the person measures generated by Rasch analysis were considered as the dependent variable. Post-hoc Tukey’s procedures were used in ANOVA analyses to determine the significant difference between the sub-samples of persons with ABI (n = 63) and controls (n = 52) based on the variable of severity of disability. The 4 groups that were compared included: (i) controls (n = 52); (ii) ABI with GR (n = 19); (iii) ABI with MD (n = 29); and (iv) ABI with SD (n = 15). The p-value was set as p < 0.05 for all the statistical analyses. The SPSS software programme, version 20.0, was used for data analysis in the study.
RESULTS
Findings of the preparatory analysis
The results of the Rasch rating scale analyses demonstrated acceptable goodness-of-fit for both items and persons to the Rasch model, indicating the internal scale validity and person response validity of the used scale in the study. A total of 113 out of 116 items (97%) in the combined items of both the long and short version of ETUQ in the Rasch analysis, and 159 out of 161 participants (99%) indicated acceptable goodness-of-fit to the Rasch model, as indicated by a MnSq ≤ 1.4 (36) with an associated standardized z < 2.0 (38). It was therefore assumed that the generated measures of perceived difficulty in ET use could be applied as valid measures to use for further statistical analysis.
Descriptive characteristics of the participants are shown in Table I. The results of t-test analysis after matching 2 groups showed no significant difference in mean age between the 2 groups (F = 0.396; df = 113; p = 0.130). The results of the χ2 test between the 2 groups in the variables sex (χ2 = 0.353; df = 1; p = 0.552), educational level (χ2 = 0.150; df = 2; p = 0.928), and occupational groups (χ2 = 2.764; df = 2; p = 0.251) after matching also indicated no statistically significant difference between them.
|
Table I. Characteristics of participants in the study in 2 samples of persons with acquired brain injury (ABI) and controls before and after matching |
|||||
|
Variables |
Before matching (n = 161) |
After matching (n = 115) |
|||
|
Persons with ABI |
Controls |
Persons with ABI |
Controls |
||
|
Participants, n |
81 |
80 |
63 |
52 |
|
|
Age, yearsa Mean (SD) [range] |
55.32 (9.25) [23 to 65] |
42.31 (14.4) [18 to 64] |
53.37 (9.56) [23 to 64] |
50.50 (10.57) [19 to 64] |
|
|
Sex, n Male Female |
47 34 |
40 40 |
35 28 |
26 26 |
|
|
Marital status, n Single Cohabitant or married |
25 56 |
18 62 |
20 43 |
13 39 |
|
|
Educational level, n Primary (≤ 9 years) Secondary (10–12 years) University (≥ 13 years) |
12 42 27 |
8 42 30 |
9 35 19 |
8 30 14 |
|
|
Occupational groups, n Professional Skilled Manual labour |
25 40 16 |
25 36 15b |
19 33 11 |
9 29 13c |
|
|
Type of ABI, n Stroke Trauma |
74 7 |
57 6 |
|||
|
Time post-injury, years Mean (SD) [range] |
5.79 (5.16) [2–30] |
6.08 (5.7) [2–30] |
|||
|
Severity of disability, nd Severe disability, total (lower/upper) Moderate disability, total (lower/upper) Good recovery, total (lower/upper) |
19 38 24 |
15 29 19 |
|||
|
aInclusion criteria were age range 18–64 years. Some participants’ ages were rounded up to 65 years during the calculation. bFour persons as missing data (n = 76). cOne person as missing data (n = 51). dAccording to the Extended Glasgow Outcome Scale. ABI: acquired brain injury; SD: standard deviation. |
|||||
Findings of the main analysis
Perceived difficulty in the use of ET. Analysis of perceived difficulty in use of ET between persons with ABI and controls revealed that the sample of persons with ABI demonstrated a higher mean level of perceived difficulty in use of ET than did the controls (F = 21.84, df = 1; p < 0.001). Table II shows means and standard deviations for comparing the means of perceived difficulty in ET use in the 4 groups. ANOVA analysis between persons with ABI with different levels of severity, as grouped above, and controls based on the mean level of perceived difficulty demonstrated a statistically significant difference between the 4 groups (F = 13.251, df = 3; p < 0.001) (see Table II). Persons with ABI with SD showed the lowest mean level of perceived ability in ET use, followed by individuals with MD, individuals with GR, and controls.
|
Table II. Results of analysis of variance to compare perceived ability in everyday technology use between groups based on mean estimates of Rasch-generated person measures of the use of everyday technology (ET) (n = 151) |
||
|
Groups |
Participants n |
ETUQ measure in logits Mean [Range] (SD) |
|
Controls |
52 |
64.27 [52.73 to 91.88] (11.67) |
|
ABI with good rec. |
19 |
61.58 [52.42 to 79.32] (9.44) |
|
ABI with mod. dis. |
29 |
55.14 [48.14 to 76.13] (5.81) |
|
ABI with sev. dis. |
15 |
48.99 [43.56 to 55.57] (3.78) |
|
Groups: persons with ABI with good recovery, moderate disability, severe disability. ETUQ: Rasch-generated person measures of the ET use; ABI: acquired brain injury; SD: standard deviation. |
||
Distribution of measures, as well as mean differences of the measures of perceived difficulty in ET use between the 4 groups, as shown in Fig. 1, show overlap in the measures of perceived difficulty in use of ET between the persons in the 4 groups.
Fig. 1. Distribution and mean differences of the measures of use of everyday technology (ET) between groups (n = 115).
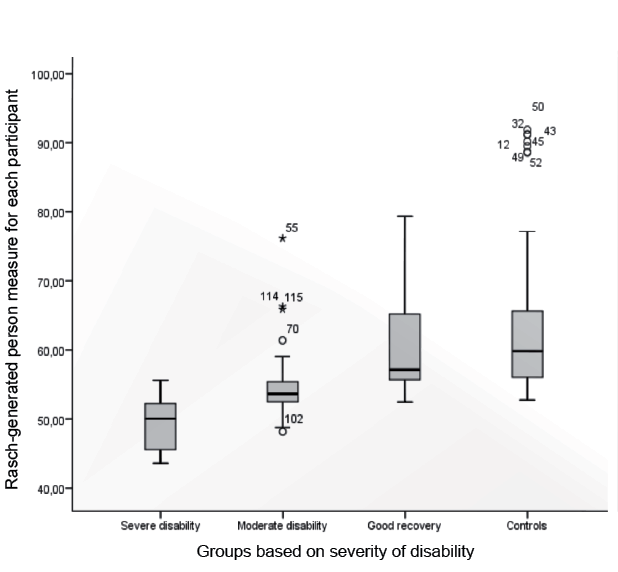
Furthermore, the post-hoc Tukey’s test showed that there is a statistically significant mean difference in perceived difficulty in ET use between persons with SD and GR, between persons with SD and controls, and between persons with MD and controls. No significant mean difference was found between persons with SD and MD, between persons with MD and GR, or between persons with GR and controls (see Table III).
DISCUSSION
This study showed that use of ET was perceived as significantly more challenging for persons with ABI with SD to MD in comparison with controls, i.e. adults with no ABI or known impairment (Table III and Fig. 1). In addition, there was a difference in the perceived difficulty between participants with SD and GR. These findings indicate that individuals with SD to MD might be at risk of being restricted in their participation in everyday activities due to their difficulties in using ET. In similar research with elderly people, it has been shown that those with no known cognitive impairment had the highest ability to use ET in comparison with people with dementia and MCI (22).
|
Table III. Results of post-hoc Tukey’s test to compare the mean difference of perceived ability in use of everyday technology between groups and the significance of p-value for different groups (n = 115) |
||
|
Sub-samples |
Perceived difficulty |
|
|
Mean difference (95% CI) |
Significance of p-value |
|
|
SD-MD |
–6.15 (–13.90 to 1.61) |
0.170 |
|
SD-GR |
–12.59 (–21.01 to –4.16) |
0.001 |
|
SD-Cs |
–15.28 (–22.43 to –8.13) |
< 0.001 |
|
MD-GR |
–6.44 (–13.64 to 0.76) |
0.097 |
|
MD-Cs |
–9.13 (–14.79 to –3.48) |
< 0.001 |
|
GR-Cs |
–2.69 (–9.23 to 3.84) |
0.705 |
|
Cs: controls; GR: persons with ABI with good recovery; MD: persons with ABI with moderate disability; SD: persons with ABI with severe disability; 95% CI: 95% confidence interval. Mean difference is statistically significant (bold). |
||
In addition, the findings showed no statistically significant difference in perceived difficulty between participants with GR and controls (see Table III). These findings indicate that people with GR after ABI do not perceive ET use as more challenging than controls. However, the findings indicate that the ranges of Rasch-generated person measures of perceived difficulty in ET use within the ABI-sample overlap (see Table II). In particular, there is an obvious overlap between the 2 groups of GR and controls (see Fig. 1), which indicates that difficulty in ET use is also related to other factors than severity of disability. This means that it is important to consider each person’s ability to manage ET as it is not solely related to the severity of the disability, i.e. a person with a MD can have a similar ability to use ET as controls. A number of qualitative studies in the area indicate, in agreement with these findings, that several aspects interact and influence the use of ET in people with ABI. Factors such as the various environmental conditions, the design of ET, the task in which the ET is used, the habits of use and the person’s capacity (23, 26, 38) have been found to influence ET use. In line with our findings, studies have also identified overlaps between groups of elderly people with cognitive impairments (22, 39). These highlight the need for more research to increase our knowledge of the factors important to ET use, in addition to the severity of the injury.
The study findings for the current working-age sample highlight the importance of level of severity of disability in using ET to engage in different activities at home, work and in public places. The link between severity of disability and ET use should be taken into account, and patients screened for perceived difficulties in ET use during the rehabilitation process after ABI, especially those with SD to MD. This is in line with a qualitative study on persons with SD and MD after ABI, showing that their ability to manage ET was not matched to the demands that ET imposed on them at work (26). In order to screen for difficulties in the use of ET, the findings of the preparatory analysis in the study showed that the ETUQ and S-ETUQ are valid for use in people with ABI. The findings also suggest that rehabilitation professionals should pay more attention to the match between the ability to use ET and the demand of the ET, in order to enhance participation in various activities at home, work and public places. However, more research is needed to determine the relationship between ET use and participation in different domains in everyday life after ABI.
Study limitations
This study is the first to compare the perceived difficulty in ET use between persons with ABI and controls. Thus, it was not possible to estimate the required sample size needed before the study in order to detect the number of participants needed to find significant differences between groups. Moreover, no information was available in the database at the rehabilitation clinic about the severity of disability or injury. Therefore, it was not possible to influence the number of participants in the 3 sub-samples of persons with ABI. In addition, the sample selection might have biased the findings, as randomization was not used, and through the matching strategy that was applied to increase the validity of the findings. Future studies with larger samples using more rigorous sampling techniques are therefore needed to compare the perceived difficulty in use of ET between various groups.
Another study limitation is the possible influence of which subjects agreed to participate in the study, as only 81 of the 215 persons in the ABI database participated. There may have been factors that made the participants who agreed to participate different from those who declined, and therefore participants may be non-representative of the population in the database. However, a former recent study of the same population found that there was no difference between those with ABI who participated and those who did not, regarding age, sex and type of injury (40). Therefore, it is reasonable to assume that the participants with ABI were representative of the population in the database.
Even if the participants’ sex, age, educational level and occupational group did not differ significantly, it is important to consider the possibility that those background variables might have biased the findings as the sub-samples were small. Consequently, only a few background variables were considered, and future research should include more variables, such as marital status, living conditions, ethnicity, diagnoses and habits of ET use. Our aim was not to study different factors that predict the perceived difficulties in ET use in the sample, but the GOS scores among the participants with ABI confirm that many of them have residual impairments or consequences of ABI. Therefore, future research should identify the factors related to the injury that predict the perceived difficulties in ET use among persons with ABI.
The use of self-reports and their possible impact on the quality of the data due to cognitive impairments such as impaired memory and self-awareness among persons with ABI can be seen as a limitation in the present study. However, the fact that the data collectors were well educated and experienced in working with the group and used techniques to ensure the quality of the participants’ answers should have increased the validity of the data. Future research based on observational instruments, such as the Management of Everyday Technology Assessment (41), can add more in-depth knowledge about their actual ability and skills in managing ET. On the other hand, self-reports are important in both research and clinical practice using a client-centred approach (42). Another potential limitation is that the data from the controls were collected by OT students due to practical reasons. However, as they were in the last semester of their OT education and received the same education and continuous support as the qualified OTs, it can be argued that the data were collected with similar quality in the 2 groups.
Conclusion
Perceived difficulty in using ET is significantly increased among persons with ABI with SD to MD compared with controls. These findings indicate the importance of rehabilitation services to consider the use of ET in order to increase participation in everyday activities among persons with ABI. However, appropriate planning in rehabilitation requires more future studies specifically focusing on different factors predicting the perceived difficulties in ET use among persons with ABI, as well as studies about how interventions can be designed to reduce difficulties in the use of ET. This study suggests that the ETUQ and S-ETUQ are valid for use in the identification of individuals’ potential to use ET after ABI in the context of everyday life.
ACKNOWLEDGEMENTS
The authors would like to thank the participants for actively taking part in this study, and to thank the occupational therapists who collected the data from the ABI sample: Ann-Charlotte Kassberg, Kristina Johansson and Anita Levén, County Council of Norrbotten, as well as the former occupational therapy students at the Luleå University of Technology who collected data from the controls: Sandra Hedberg, Susanne Nisbel, Benozir Rahman and Natalia Seydakova.
The study was supported by grants from the Promobilia Foundation, the Strategic Research Programmes in Care Sciences at the Umeå University, the Karolinska Institutet and the Luleå University of Technology.
REFERENCES

