Justin N. Chee, MSc1,2, William H. Gage, PhD2,3, William E. McIlroy, PhD1,2,4 and Karl F. Zabjek, PhD1,2,5
From the 1Graduate Department of Rehabilitation Science, University of Toronto, 2Toronto Rehabilitation Institute, 3School of Kinesiology and Health Science, York University, Sherman Health Science Research Centre, 4Department of Kinesiology, University of Waterloo and 5Department of Physical Therapy, University of Toronto, Toronto, ON, Canada
OBJECTIVE: To develop a video-based system, mounted on a rollator to quantify the step width values of rollator users in the community.
SUBJECTS: A total of 5 able-bodied young adults, age range 24–28 years.
METHODS: A digital video camera system was mounted on the rollator frame to capture the position of the participant’s feet during overground walking. A method of estimating step width from the video data was developed and evaluated against the output from a concurrently recording Vicon MX motion capture system.
RESULTS: Mean step widths of the rollator and motion capture systems were 14.40 cm (standard deviation (SD) 4.64) and 14.37 cm (SD 4.34), respectively, revealing a strong level of agreement; intra-class correlation coefficient 0.999 (95% confidence interval (95% CI) 0.987–1.000); and root-mean-square difference 0.70 cm.
CONCLUSION: The video-based system mounted on a rollator to collect foot placement data enabled accurate measurement of step width during rollator use. The ability to record foot placement measurements outside the laboratory setting, characterizing foot placement patterns occurring in the community, will enable research into how these assistive devices influence mobility during everyday use.
Key words: gait; mobility limitation; monitoring, ambulatory; self-help device; walker; walking.
J Rehabil Med 2015; 47: 00–00
Correspondence address: Justin N. Chee, Graduate Department of Rehabilitation Science, University of Toronto, 500 University Avenue, Room 160, Toronto, Ontario, M5G 1V7, Canada. E-mail: justin.chee@mail.utoronto.ca
Accepted Aug 27, 2014; Epub ahead of print Dec 1, 2014
INTRODUCTION
Mobility aids, such as the rollator or four-wheeled walker, are widely used in community settings by many mobility-impaired populations (1). However, recent research has shown that mobility aids can have a negative impact on the users’ balance and stability in the community. For instance, use of assistive aids has been associated with an increased risk of falls (2). Until recently, only a limited understanding of how these devices are used in everyday environments could be attained. Ambulatory monitoring of gait during rollator use outside the laboratory is now possible with the advent of instrumented devices. Such monitoring may enable a better understanding of the factors responsible for falls in these individuals.
Falls during use of mobility aids may occur for a wide range of reasons, including improper transfers (e.g. falling over a wheeled walker, leaving brakes off) or balance and stability difficulties during gait. In the context of gait-related falls, foot placement is an important factor to monitor in community-based environments. For example, frontal plane foot placement characteristics, such as step width, have been associated with falls risk in older adults (3). Examining step width during rollator use is of particular importance because of the potential for the user’s feet to come into contact with the back wheels of the rollator. Such an occurrence may lead to a trip or loss of balance. Furthermore, the walking environment has features that can alter foot placement characteristics, including step width (e.g. surface texture, attention-demanding distractions, etc.) (4). Since a wide-range of neurological patient populations commonly exhibit altered foot placement characteristics compared with able-bodied individuals (e.g. increased step-to-step variability) (5), this may have implications for their ability to ambulate safely in challenging environments (e.g. uneven surfaces) (6). While foot placement characteristics remain a potentially important index of the control of walking, there are few tools for measuring foot placement during the use of assistive aids outside the laboratory (i.e. in everyday settings).
The aim of this proof of concept study was to develop and evaluate a mobile measurement device for assessing the walking characteristics of rollator users. This comprised a video-based system mounted on an instrumented rollator, which was used to measure foot placement characteristics, specifically step width during use in the community. The development of such ambulatory measurement tools will enable evaluation of the use of mobility aids in everyday situations, thus providing information to clinicians, caregivers and patients about the activity, health and well-being of individuals in daily life.
METHODS
Subjects
Five able-bodied young adults were recruited to this proof of concept study. The participants’ ages range was 24–28 years (mean age 26.8; standard deviation (SD) 2.2). Three individuals were female. These volunteers had no history of neurological or musculoskeletal disorders or mobility impairments. Written informed consent was provided prior to their participation, in agreement with the guidelines of the University of Toronto Research Ethics Board.
Experimental procedure
Participants were instructed to walk across a 7-m walkway, in the Biomechanics and Assistive Technologies Laboratory at the University of Toronto, while using a rollator. Subjects completed 3 passes of the walkway at their preferred speeds. Excluding gait initiation and termination, approximately 5 steady-state walking steps were performed during each pass, resulting in the acquisition of 4 step-to-step widths per pass. As a result, in total, there were 12 step-to-step widths available for analysis from each of the 5 subjects.
Equipment
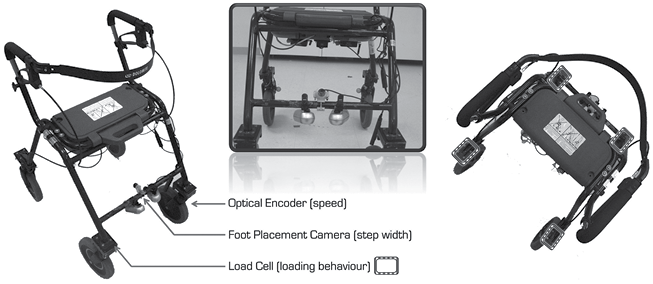
Two measurement systems were used to quantify foot placement: (i) a video system mounted to the rollator and (ii) 3D motion capture. The ambulatory system was mounted on a standard rollator (Invacare Dolomite AB, Diö, Sweden) and consisted of a portable digital video camera system (Archos Helmet Camcorder/404 Media Player, Archos, Inc., Greenwood Village, CO, USA) with a wide-angle lens oriented at the feet (1.7 mm, Edmund Optics, Barrington, NJ, USA) (Fig. 1). Motion capture was performed using a 7-camera VICON MX Motion Capture System (Vicon, Denver, CO, USA) and served as the gold standard for evaluation of outcomes.
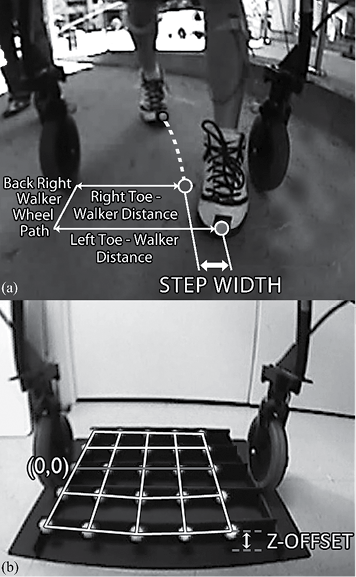
These 2 systems were used concurrently to record the position of the same passive foot markers (2.5 cm diameter) positioned on the feet. To facilitate the visibility of the markers in the rollator-mounted cameras, the foot markers were placed over the tips of the toes at the midlines of the feet, near the third metatarsals, and at a fixed height above the ground (i.e. 5 cm) (i.e. Z-offset in Fig. 2b). The position of these markers was recorded by the rollator-mounted cameras in relation to a local co-ordinate system defined by markers mounted above the medial side of both rear wheels of the rollator. The motion capture system recorded the position of these markers in relation to a global co-ordinate system in the laboratory.
Procedure for step width estimation
Step width is traditionally defined as the medio-lateral distance between the feet during 2 consecutive footfalls. Previous work has utilized the position of the heel, at heel strike, to define step width. However, in the present study, it is important to take into consideration that the video system was mounted on the rollator and pointed backwards and downwards towards the feet. The heels are obscured, and thus, the toe markers were chosen as the location to track foot position (Fig. 2a). Since the video system mounted on the rollator is in continuous movement, it was important to reference the position of the foot with respect to the rollator. All data-points for the position of each foot-fall were thus estimated at the point in time during foot flat-mid-stance when the antero-posterior position of the toe marker intersected the projected line between the 2 rear wheels of the rollator (Fig. 2). The calculation was also performed for the motion capture collection to ensure that foot placement was determined at the same absolute time between the 2 collection systems.
Data analysis
Each frame of video data was rectified in MATLAB (Mathworks, Natick, MA, USA) to correct for image distortion, which was caused by parallax error associated with the curvature of the camera lens (7). Each video frame was then colour-filtered to accentuate the foot markers, and thus, help to distinguish them from the image background. This was accomplished using: (i) standard built-in routines in the VirtualDub software (Santa Barbara, CA, USA), which adjust the saturation (× 200%), hue-saturation-value (HSV) (–41%), brightness (–3%) and contrast (+131%); and (ii) a custom-made marker localization algorithm in MATLAB, which brightens the intensity of pixels in each video frame that have RGB components within a similar range to the foot marker’s distinctive orange colour. The outcome of this filtering technique was imported into video marker tracking software (Peak Motus 7.0, Vicon, UK) and the foot marker’s coordinate position was extracted by automatically locating the centroid of marker pixels in the video frame. Once extracted, these foot marker coordinate values were expressed in relation to the coordinate positions of markers on the rollator frame. Lastly, the pixel distance, between the foot and the rollator, was scaled to reflect its actual distance in millimetres. This scaling procedure was performed by multiplying the foot-rollator pixel distance by a specific scaling coefficient, which depended on the position of the foot in the camera’s field-of-view. Specific scaling coefficients were obtained by calculating the quotient of actual, known distances, in millimetres, and virtual distances, in pixels, between points on a custom-made calibration tool. Prior to each data collection, the calibration tool was placed in a consistent position within the field-of-view of the rollator-mounted camera and recorded for 5 s (Fig. 2b), such that this scaling procedure could be performed during post-processing.
Statistical analysis
To evaluate the association between the video-based system on the rollator and the motion analysis system, an intra-class correlation coefficient (ICC3,k) was computed, using a 2-way mixed-effects model with an absolute agreement approach. Reasonable validity was assumed if the ICC exceeded 0.90, with the level of significance set at 0.05. To compute the measurement error, the root-mean-square (RMS) was determined between the step width values of the 2 systems. A Bland-Altman analysis was also performed to further assess the level of agreement between the 2 systems and detect any relationships between the variance in measures and the size of the reference method values (8, 9). Agreement would be confirmed visually if no considerable measurement bias, trends, or heteroscedasticity were evident in the data-points on the plot.
RESULTS
A very high level of concordance was observed between the rollator-based and Vicon systems, as revealed by an ICC of 0.999 (95% confidence interval (95% CI) 0.987–1.000) using a 2-way mixed effects model. The step widths estimated using the rollator-based system (mean 14.40 cm (SD 4.64), range 9.82–21.85 cm) were highly comparable to those generated by the Vicon system (mean 14.37 cm (SD 4.34), range 10.13–21.22 cm) (Fig. 3). This was also revealed by the small mean RMS difference between the step width estimates of the 2 systems (0.70 cm). Lastly, a strong level of agreement between the 2 systems was corroborated using Bland-Altman analysis. The range of agreement between the step width estimates of the 2 systems (i.e. the mean bias of the systems ± 1.96 SD) had a maximum of 1.43 cm and minimum of –1.38 cm (Fig. 4). The plot also confirmed visually that there were no relationships present between the variance in measures and the size of the reference method values that required mathematical compensation.
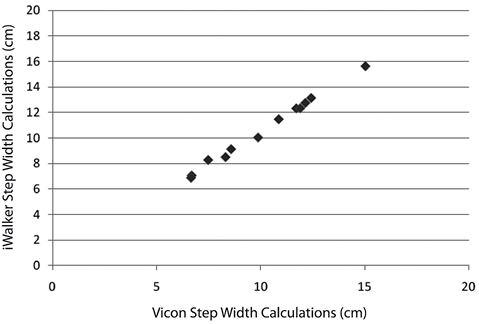
Fig. 3. Scatter plot of step width values computed by the Vicon and iWalker systems for a representative participant. Each data-point represents a single step-width calculation for the participant.
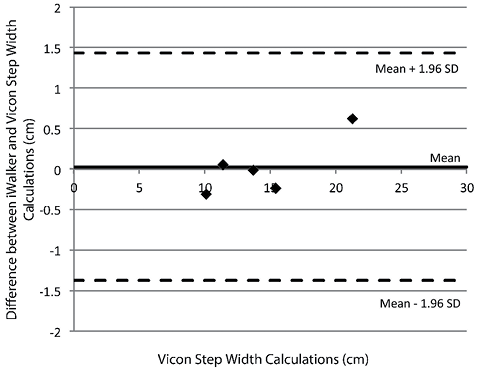
Fig. 4. Difference against the size of the reference method value (Bland-Altman plot) for the rollator-based and Vicon calculations of step width in able-bodied young adults. Each data-point represents the mean step width values for a single participant.
DISCUSSION
The results of this study indicate that step width during rollator use can be successfully quantified using a digital video system mounted on a rollator. Although the mean error of the rollator-based system was small (i.e. 0.70 cm) and was in the range of other technologies commonly used to quantify spatiotemporal gait characteristics (e.g. instrumented walkways) (10, 11), it exceeded the error exhibited by three-dimensional optoelectronic motion capture systems (e.g. Vicon and Optotrak) (12, 13). The increased error could be attributed to a number of factors, including: (i) limitations in the effectiveness of the parallax error rectification procedure on data acquired using a wide-angle lens; and (ii) un-intentional, albeit minimized, movements of the camera relative to the rollator frame, which would hinder the accuracy of the calibration and scaling procedures. Nevertheless, the mean step width values obtained using this system (i.e. 14.40 cm) were similar to those observed in previous studies involving able-bodied young adults (e.g. 15.2 cm in Grabiner & Troy (14)). Furthermore, the error exhibited by the rollator-based system constituted merely a proportion of the expected variation in the step widths of both healthy and patient populations (e.g. 2.9–5.2 cm for normal adult gait, and 4.0–9.0 cm for the gait of individuals with multiple sclerosis) (11, 15). Therefore, our results demonstrate the potential of this technique to detect environmentally-induced changes to step width that are larger than the natural variability of this gait parameter.
Several future directions could be explored in order to improve this approach to measuring step width in its current form. For example, the technique involves tracking passive markers over potentially busy backgrounds (e.g. coloured, inter-locking brick walkways). As a result, foot position tracking procedures may be enhanced by switching to an active marker system or a marker-less tracking method (16), as employed in previous work. Alternatively, multiple cameras or portable depth camera solutions may also provide a method that improves tracking. Furthermore, to-date the rollator-based technique has been evaluated only in young adults during straight path walking. However, older adults and persons with neurological disorders may exhibit greater variability in gait patterns, which may affect the accuracy of the technique, and useful information could be obtained from quantifying foot position during turning and obstacle avoidance events (e.g. pedestrian circumvention). Further testing of this technique should be conducted in order to determine whether its performance differs in other populations and as participants perform tasks that involve walking along non-linear paths. In addition, the current application of this technique enables only the quantification of step width. However, in order to obtain a more comprehensive understanding of the factors responsible for falls during the use of assistive devices, it would be useful to consider how this technique can be enhanced to increase the number of gait characteristics and gait-related incidents that are monitored (e.g. step width variability, step-to-step asymmetry, step length, occurrence of collisions and near collisions with the rollator frame, improper transfers, etc.). Testing the accuracy of measuring those additional parameters or incidents would be necessary once the technique has been modified to incorporate them. Lastly, the current technique involves time-intensive post-processing procedures. Future work should therefore explore ways to make the process more automated, since the real-time on-board detection of gait characteristics will eventually be necessary to maximize the utility of such tools.
This is a potentially valuable tool for monitoring everyday community mobility, given the importance of foot placement, specifically step width, as an indicator of balance control and medio-lateral stability. Such measurements can also inform about the situational challenges in daily walking (e.g. where step characteristics are different) and this image-based approach can be combined with other wearable technologies that can yield details of temporal characteristics of foot placement. The present work is limited to a laboratory-based assessment of gait. Thus, it has only been used to measure the gait patterns of individuals under conditions in which: (i) the participants are on their best, not usual behaviour (i.e. Hawthorne effect); and (ii) walking conditions are ideal, not realistic (i.e. using environments with level, even-surfaced walkways under good lighting, as opposed to those that contain both challenging physical and cognitive demands). Nevertheless, this work lays the foundation for the quantification of step width outside of gait laboratories and clinics in future applications. In doing so, one may be able to gain environment-specific insight into the control of balance and challenges to stability that rollator users face in the community.
ACKNOWLEDGEMENTS
The authors acknowledge the support of the Toronto Rehabilitation Institute, which receives funding under the Provincial Rehabilitation Research Program from the Ministry of Health and Long-Term Care in Ontario. The views expressed in this paper do not necessarily reflect those of the Ministry. Equipment and space have been funded with grants from the Canada Foundation for Innovation, Ontario Innovation Trust and the Ministry of Research and Innovation. The authors would also like to thank the Institute of Aging of the Canadian Institutes of Health Research (CIHR) (IAP #82640) and the Ontario Neurotrauma Foundation (graduate student stipend) for providing funding in support of this work.
The authors declare no conflicts of interest.
REFERENCES

