Kristine M. Oostra, MD1, Anne Oomen, MD1, Guy Vanderstraeten, MD, PhD1 and Guy Vingerhoets, PhD2
From the 1University Hospital Ghent and 2Department of Experimental Psychology, Ghent University, Ghent, Belgium
OBJECTIVE: To evaluate the effect of mental practice on motor imagery ability and assess the influence of motor imagery on gait rehabilitation in sub-acute stroke.
DESIGN: Randomized controlled trial.
SUBJECTS: A total of 44 patients with gait dysfunction after first-ever stroke were randomly allocated to a motor imagery training group and a muscle relaxation group.
METHODS: The motor imagery group received 6 weeks of daily mental practice. The relaxation group received a muscle relaxation programme of equal duration. Motor imagery ability and lower limb function were assessed at baseline and after 6 weeks of treatment. Motor imagery ability was tested using a questionnaire and mental chronometry test. Gait outcome was evaluated using a 10-m walk test (near transfer) and the Fugl-Meyer assessment (far transfer).
RESULTS: Significant between-group differences were found, with the vividness of kinesthetic imagery and the walking test results improving more in the motor imagery group than in the muscle relaxation group. There was no group interaction effect for the far transfer outcome score.
CONCLUSION: Motor imagery training may have a beneficial task-specific effect on gait function in sub-acute stroke; however, longer term confirmation is required.
Key words: mental practice; motor imagery; gait rehabilitation; stroke.
J Rehabil Med 2015; 47: 00–00
Correspondence address: Kristine Oostra, Department of Physical and Rehabilitation Medicine, Ghent University Hospital, BE-9000 Ghent, Belgium. E-mail: kristine.oostra@uzgent.be
Accepted Aug 27, 2014; Epub ahead of print Nov 14, 2014
Introduction
Mental practice (MP) can be defined as “the process of imaging and rehearsing the performance of a skill with no related overt actions” (1). Several authors have reported that mental practice, in combination with physical therapy, can improve motor performance in stroke patients (2–7). Because the process of imagery is not dependent on the ability to execute a movement, mental practice can be implemented early in rehabilitation in order to train motor preparation and thus facilitate physical recovery. Furthermore, this training method can be performed by the patient alone after some familiarization and instruction (5).
Patients with impaired motor imagery (MI) ability should be identified as being suitable for imagery training; however, it is not known whether a high level of MI ability is necessary for therapy response before commencing MI therapy (8). Unrelated to cerebral damage, there are individual differences in motor imagery ability. Hall et al. classified subjects as high or low imagers based on their scores on the Movement Imagery Questionnaire (MIQ), and demonstrated that individual differences in motor imagery ability can influence performance of motor tasks (9, 10). Moreover, since motor imagery and motor execution are believed to share a similar underlying neural network, any structural damage to the brain could affect both motor performance and motor imagery (11). Malouin et al. (12) found the vividness of motor imagery in stroke patients to be similar to that of age-matched healthy persons, although they reported better motor imagery vividness for the unaffected side. Given the higher variance of MI ability in stroke patients, the first aim of the current study was to assess motor imagery ability in patients in their sub-acute rehabilitative phase and less than one year following stroke and to determine whether this ability could be trained and stimulated to a higher level of performance in order to maximize the potential rehabilitative effect. We assessed motor imagery vividness in our patients using an MI questionnaire and mental chronometry paradigms. Several studies indicate that ratings from imagery questionnaires provide a good indication of the ability to generate vivid images of movements (12, 13). Mental chronometry paradigms measure the temporal coupling between actual and imagery movements (14, 15). Because temporal characteristics of motor imagery should be screened for the task to be trained, we introduced a walking trajectory test to quantify imagery of gait. This validated test demonstrated a high temporal congruence between actual and imagined walking in a healthy population (15).
Stroke patients rank the restoration of walking as one of the most important goals of their rehabilitation (16). In a prospective cohort study, Kollen et al. (17) showed that independent gait was regained by only 62% of stroke patients 6 months after stroke onset. Although many patients eventually regain some ability to walk, independence in moving about the community often remains compromised (18). Given its clinical importance, therapeutic interventions that assist in gait recovery are highly relevant. The incorporation of mental practice into rehabilitation of the lower limb in a chronic phase after stroke has been assessed by several authors. For example, Dickstein et al. reported a series of case studies in which gait was trained using a home-based motor imagery programme (5, 19) and found an enhancement in gait speed in their stroke population. Recently, Cho et al. (20) found that adding motor imagery to gait training enhanced balance and gait ability in their patients during the chronic phase post-stroke. The second purpose of our study was therefore to confirm and extend these findings and examine whether motor imagery training in combination with physical practice is also beneficial in improving gait function in the sub-acute phase following stroke.
Methods
Participants
This study was a single-centre, randomized controlled trial. Patients who were eligible for the study were invited to participate. Those who volunteered and gave written consent were then randomly allocated into 1 of 2 different treatment groups using a process of blinded random number allocation. Forty-six patients were eligible; 44 patients gave written consent and 2 declined to take part. Twenty-one were placed in the motor imagery training (MIT) group and 23 in the muscle relaxation (MR) group. In order to compare patients’ performance with neurologically intact participants, 27 healthy age-matched control subjects were recruited.
The participant flow through the trial is shown in Fig. 1 and the demographic variables of all participants are shown in Table I.
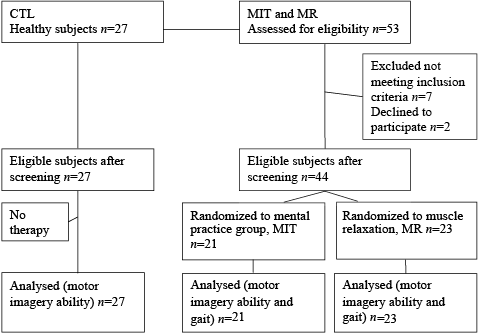
Fig. 1. Flow of participants through the trial. MIT: motor imagery training; MR: muscle relaxation; n: number.
|
Table I. Participants’ characteristics |
|||||
|
Characteristics |
MIT group n = 21 |
MR group n = 23 |
p-value (MIT vs MR) |
Control group n = 27 |
p-value (patients vs controls) |
|
Sex, male/female |
15/6 |
14/9 |
0.46 |
14/13 |
0.24 |
|
Age, years, mean (SD) |
50.3 (12.8) |
53.7 (12.0) |
0.38 |
47.3 (12.3) |
0.12 |
|
Disease duration, months, mean (SD) |
4.7 (3.1) |
3.6 (2.0) |
0.15 |
NA |
|
|
Hemiplegic side, n |
0.38 |
||||
|
Right |
11 |
10 |
NA |
||
|
Left |
10 |
13 |
NA |
||
|
Cause of hemiplegia, n |
0.82 |
||||
|
Ischaemic |
13 |
15 |
NA |
||
|
Haemorrhagic |
8 |
8 |
NA |
||
|
LE-FM (/34), mean (SD) |
19.1 (5.6) |
19.8 (5.6) |
0.73 |
NA |
|
|
SD: standard deviation; MIT: motor imagery training; MR: muscle relaxation; NA: not applicable; LE-FM: lower-extremity Fugl-Meyer. |
|||||
In addition, the physician responsible for assessment of patients throughout the study remained blinded to the patients’ group allocation for the full duration of the trial.
All patients sustained their stroke between August 2009 and June 2013. The patients were recruited via the University Hospital and from hospitals in East and West Flanders to the Rehabilitation Centre, University Hospital of Ghent.
Participants were eligible if they: (i) had experienced a first-ever stroke less than one year before entering the study; (ii) were able to walk 10 m with minimal assistance (Functional Ambulation Category ≥ 3); (iii) were able to pass the Time Dependent Motor Imagery screening test (TDMI, see below); (iv) were between 16 and 70 years old; and (v) did not have psychiatric symptoms or any other neurological disease.
The TDMI was developed and validated by Malouin et al. (14) and requires the examiner to record the number of movements imagined over 3 time-periods (15, 25 and 45 s) and specifically involves only imagined movements. The test indicates whether a person is able to understand instructions and simulate movements.
The study was approved by Ghent University Hospital ethics Committee.
Procedures
All patients (MIT and MR) received a standard rehabilitation programme, consisting of 2 h physical therapy and 1 h occupational therapy daily, 5 days per week. Physiotherapy was based on the Bobath concept using facilitation and guidance techniques. Additional physiotherapy and occupational therapy consisted of task-specific functional training including transfer and balance practice and walking incorporated in different daily activities.
In addition to standard training, the MIT group received 30-min daily mental practice treatment sessions, based on the protocol described by Dickstein et al. (19). Each session was individually delivered in a quiet room in the hospital by 2 experienced therapists who were not involved in any other part of the study. Every session started with 2 min of relaxation preceding the imaging session. During motor imagery practice participants were seated in a (wheel) chair and instructed to keep their eyes closed. The practice was performed from an internal perspective with both a visual (“viewing” themselves performing the task) and kinesthetic mode (“feeling” the experience of performing the task), with emphasis on the latter. During the first week the MIT participants were familiarized with the MI technique, whereby the therapist gave visual, auditory and sensory cueing to each patient, focusing on imaging of environmental situations well known to the patient. During the second week MI training was focused on the individual patients’ gait problems, such as forefoot landing, absence of knee loading response, knee hyperextension in stance and stiff knee gait. Gait-specific lower limb movements (hip flexion/extension, knee flexion/extension, ankle flexion/extension) were thus guided by individual gait analysis (n = 15). In addition, information concerning the patient’s gait problem areas was provided to the MI therapist by the treating rehabilitation therapist. During the third and fourth weeks, gait symmetry and velocity were rehearsed using different (motor imagery) walking tasks, focusing on integrating the components practiced previously into the (mental) gait cycle. Participants were asked to pay specific attention to step length and walking speed. Auditory cues were used to guide walking speed. During the last 2 weeks of practice, gait exercises were embedded in activities of daily living. Patients were instructed to “view” and “feel” themselves walking in different situations and environments and on different terrains. Throughout the MI sessions, patients were asked open questions about the content of motor imagery sensations in order to verify their involvement in mental practice. Their feedback was used by the therapist to optimize further instructions regarding movement exercise and associated sensory perceptions.
The MR group, on the other hand, received the same amount of muscle relaxation therapy over and above the standard rehabilitation training. Muscle relaxation was used to control for therapeutic attention and consisted of relaxation therapy of daily 30-min one-to-one sessions. Relaxation followed the principles of progressive muscle relaxation according to Jacobson (21). The basic principle of this technique is to begin by instructing participants to physically tense particular muscle groups in a given order and then to relax and let go of the muscle contraction. During the same session the subjects were asked to concentrate on using diaphragmatic breathing to aid relaxation.
The motor imagery ability of the healthy control group was also assessed to provide age-matched reference data.
Outcome measures
All participants (patients and healthy volunteers) were assessed at baseline, and both patient groups (MIT and MR group) were re-assessed after 6 weeks by the same assessor. A brief description of the tests used is provided below.
The first 2 tasks were used to assess aspects of motor imagery ability.
Movement Imagery Questionnaire-revised. The MIQ-R is a self-report questionnaire developed and validated by Hall & Buckholtz (9) in order to assess visual and kinesthetic modalities of movement imagery. A revised version, the MIQ-RS was developed and validated by Gregg et al. (22). The MIQ-RS is composed of 2 sub-scales of 7 relatively simple movements (e.g. bending forward, or pulling a door handle) for use with people with limited mobility. For each item, 4 steps are required. First, the starting position of the movement is described by the examiner and the subject is asked to assume this position. Secondly, the movement is described and the subject is asked to perform it. Thirdly, the subject is asked to reassume the starting position and imagine producing the movement (no actual movement is made). Finally, the subject is instructed to rate the ease/difficulty with which he or she imagined the movement on a 7-point scale, where 1 is very difficult and 7 is very easy to picture (visual sub-scale, MIQ-RSvis) and feel (kinesthetic sub-scale, MIQ-RSkin).
Walking trajectory test. For this test, the participants were seated in a chair in front of a computer screen that displayed photographs of 3 walking trajectories. The walking trajectories had a varying length of 2, 5 and 10 m. The beginning of the walking trajectory was marked with a blue line and the end with a cone. There were 2 practice sessions, an imagery session, referred to as the imagined walking time (IWT), and an actual walking session, known as actual walking time (AWT). These 2 times were expressed as a ratio: IWT/AWT, which, if a subject took exactly the same time to walk as to imagine walking, would equal 1. Each imagery session began with the presentation of a photograph of a walking trajectory. The subjects were then asked to imagine walking at comfortable speed along the path and indicate when they had reached the cone. The examiner recorded the duration of each trial. Subjects subsequently performed the actual walking trial. The actual walking session was always performed after the imagery session in order to minimize the amount of tacit knowledge about the time it actually took to walk along the trajectory.
Clinical outcome was assessed using validated and reliable tools for lower limb function after stroke: the 10-m walk test and the Lower-extremity Fugl-Meyer assessment scale (LE-FM) (23, 24). The former test was used to assess an immediate training response of MI on walking and thus represents a near transfer effect of MI training. The latter test investigates possible far transfer effects of motor imagery, since it encompasses a more general evaluation of lower limb function and is not restricted only to gait.
10-m walk test. Gait velocity was measured by asking the patient to walk a 10-m distance at comfortable speed. Times were recorded with a stopwatch after 2, 5 and 10 m. The patients performed this test with their usual assistive device and/or brace, using the same device at the pre- and post-training assessment.
Lower-extremity Fugl-Meyer assessment scale. This instrument measures distinct parameters of motor recuperation, such as reflexes, voluntary control of isolated movement, co-ordination, speed and balance. The lower-extremity component of the scale was applied in this study. It consists of a total score of 34 points with 17 items, scored on a 0–2 scale.
Statistical analysis
Statistical analysis was performed using SPSS Statistics 21.0 software. Data are expressed as median and interquartile range. For nominal scale data, Pearson’s Chi-square tests were used. Related-samples Wilcoxon Signed-Rank tests were used to investigate within-group differences and independent samples Mann-Whitney U tests were used to examine between-group differences. Analysis of variance (ANOVA)was used to assess the interaction effect between group and pre-post measurements. Significance was accepted at p ≤ 0.05.
Results
None of the participants dropped out during the study. The results are based on all 44 patients and 27 healthy controls. Individual participant characteristics are summarized in Table I. There were no significant differences between the MIT and MR groups in demographic or clinical variables. At the start of the treatment, independent sample Mann-Whitney U tests showed that MIQ-RSvis and MIQ-RSkin scores were significantly (p = 0.005 and p = 0.004, respectively) higher in the control group than in the patient group (MIT and MR combined as 1 patient group). However, temporal coupling between imagined and actual walking (Imagery Walking Time/Actual Walking Time) revealed no differences between patients and controls (Table II). More importantly, independent sample Mann-Whitney U tests also revealed that the 2 treatment groups did not differ with respect to performance in baseline motor imagery ability performance, as MIQ-RSvis, MIQ-RSkin, and IWT/AWT ratios appeared very similar (Table III).
|
Table II. Descriptive statistics for the motor imagery ability variables (patients vs controls) |
|||
|
Variables |
Patients (MIT + MR) n = 44 Median (IQR) |
Controls n = 27 Median (IQR) |
Sig. |
|
MIQ-RS Visual scale (/49) |
35 (17) |
41 (9) |
0.005 |
|
MIQ-RS Kinesthetic scale (/49) |
30 (15) |
39 (15) |
0.004 |
|
IWT/AWT |
0.95 (1.03) |
1.11 (1.94) |
0.44 |
|
IQR: interquartile range; Sig.: significance level; MIT: motor imagery training; MR: muscle relaxation; MIQ-RS: Movement Imagery Questionnaire – revised second version; IWT: imagery walking time; AWT: actual walking time. |
|||
|
Table III. Patients’ performance and treatment effects in all outcome measures and comparison of treatment effects between the experimental and control group after 6 weeks |
|||||||
|
MIT group n = 21 |
MR group n = 23 |
Sig.a |
Sig.b |
||||
|
Inclusion Median (IQR) |
After 6 weeks Median (IQR) |
Inclusion Median (IQR) |
After 6 weeks Median (IQR) |
||||
|
MIQ-RSvis (/49) |
35 (15) |
40 (9) |
37 (17) |
33 (21) |
0.102 |
0.08 |
|
|
MIQ-RSkin (/49) |
28 (13) |
35 (9) |
30 (15) |
30 (22) |
0.021 |
0.044 |
|
|
IWT/AWT |
1.12 (1.17) |
1.12 (0.64) |
0.84 (0.83) |
1.0 (0.45) |
0.56 |
0.82 |
|
|
AW 10-m(s) |
33.4 (27.0) |
19.3 (21.3) |
29.1 (30.6) |
18.0 (19.1) |
< 0.001 |
0.04 |
|
|
LE-FM (/34) |
17.0 (11.0) |
21.5 (12.0) |
18.5 (9.0) |
22.5 (10.0) |
< 0.001 |
0.35 |
|
|
aMain effect of assessment (pre-post), within-group comparisons, significant values according to the Wilcoxon signed-rank test are in bold. bInteraction effect between treatment type (MIT/MR) and assessment time (pre-post), between-groups comparisons, significant p-values are in bold. IQR: interquartile range; Sig.: significance level; MIQvis: Movement Imagery Questionnaire-Revised second version visual subscale; MIQkin: Movement Imagery Questionnaire-Revised second version kinesthetic subscale; IWT: imagery walking time; AWT: actual walking time; AW: actual walking; FM-LE: lower-extremity Fugl-Meyer; MIT: motor imagery training; MR: muscle relaxation. |
|||||||
Related-samples Wilcoxon Signed-Rank tests were used to evaluate the effect of treatment in general, that is comparing the pre-post assessment for the entire patient group (n = 44). Main effects of session were found for MIQ-RSkin, actual walking over 10 m, and the lower-extremity Fugl-Meyer score (Table III). Since the treatment by session effect cannot be captured in a nonparametric design, we used ANOVA to assess the interaction effect of treatment condition on the MI ability variables. Group (MIT, MR) was entered as between-subject factor, and session (baseline, final) was included as within-subject factor. A main effect of session was found for MIQ-RSkin and a group by session interaction effect revealed that after treatment the MIQ-RSkin scores had improved significantly more in the MIT group than in the MR group (p < 0.05) (Table III). Analysis revealed that the MIQ-RSkin scores of the MIT group after training showed no statistical difference from those scores of the healthy control group, indicating that the former were now within the normal range. The IWT/AWT ratio did not change statistically after the treatment and there was no group interaction effect. Finally, we similarly assessed the effect of treatment condition on lower limb function. The 10-m walk scores and lower extremity Fugl-Meyer assessment (LE-FMA) scores improved significantly in both groups after treatment (p < 0.001 for both values). We also found a significant group interaction effect for the 10-m walk test (F(1,43) = 4.5, p < 0.05), revealing a significantly reduced walking duration in the MIT group compared with the MR group. There was no significant interaction between session and group for the LE-FMA score.
In order to assess the possible influence of initial MI-vividness on gait improvement, we investigated the association between baseline MIQ-RS scores and walking speed. No significant correlation between initial MIQ-RS scores (nor of pre-to-post changes in the MIQ-RS scores) and gait velocity improvement after treatment was found.
Discussion
Effect of motor imagery training on motor imagery ability
Motor imagery ability can be affected by stroke. It is not known whether being able to perform MI tasks is necessary to gain benefit from it in clinical practice (8, 9). Moreover, Confalonieri et al. report that motor imagery stimulates sensorimotor and pre-motor areas even in poor imagers with stroke (25). In our study we found no correlation between motor imagery ability (as reflected by initial MIQ-RS scores) and our outcome measure of gait velocity improvement after motor imagery training. This suggests that those with poor motor imagery underwent the same improvement as those who were better imagers. When using the MIQ-RS questionnaire, we found that both the visual and kinesthetic imagery modalities differed significantly from normal data in our stroke study population. Although frequently used, the questionnaire scores remain a subjective reflection of the estimated motor imagery vividness. In a further study by Malouin et al. (12), motor imagery vividness was measured using the Kinesthetic and Visual Imagery Questionnaire (KVIQ-20). They found a continuum of good to bad imagers similar to a normal age-matched population. The results of our study also indicate that MI vividness responded well to MI training, with a significant increase in the kinesthetic subscale scores. This may be important, as kinesthetic imagery from the first-person perspective has been shown to best activate the mental processes involved during motor task training (26). Our study results indicate that patients with poor imagery vividness pre-treatment should not be excluded from mental practice. However, the technique should first be taught, incorporating a training period at the start of the intervention period and to provide an extended learning period for poor imagers to become familiar with the procedure.
In our cohort the temporal organization of motor imagery measured by the imagined/actual walking ratio did not differ from the data of the healthy control subjects. Task instructions and the use of two-dimensional photographs might have influenced the results in both groups so they all slightly overstated the time to imagine walking. However, a strong relationship was found between imagery and actual walking times in both groups. Stroke patients were markedly slower on the imagery condition, but their actual walking was slowed to the same extent, indicating a preserved MI performance. These results concur with the findings of Malouin et al. (2), who also found that the temporal representation of a complex locomotor task (Timed Up and Go Test; TUG) was retained following stroke. The close temporal relationship between actual and imagined walking revealed that subjects were able to imagine walking in an environment in which they were not actually present.
Effect of motor imagery training on gait
More importantly, our study addressed the hypothesis that a combination of physical practice and motor imagery training is more effective than physical practice alone in gait rehabilitation in the sub-acute phase following stroke. The main outcome of this study indicates that there is modest but clear evidence supporting the additional benefit of mental practice in gait rehabilitation in the sub-acute phase after stroke, with a positive effect of a motor imagery intervention on gait velocity measures. We found a significant group interaction effect for gait velocity, measured by the 10-m walk test, in that the velocity of MIT group, despite having initial lower (non-significant) gait velocities, improved more than that of the MR group at 6 weeks. Although gait velocity does not indicate the quality of movement, it is a valid and reliable measure and is sensitive to change in walking capacities (27).
Several studies using mental practice in stroke populations have reported significant positive effects on motor function (5–7). Dunsky et al. investigated the feasibility of a home-based motor imagery training programme for gait rehabilitation in chronic stroke and demonstrated a positive effect on gait performance (5). A locomotor imagery training with a 5-stage protocol was described by Hwang et al. (28). Their subjects received a video-based motor imagery showing a young adult with a normal gait. Problem identification was an important part of the treatment protocol. Although no video-recording was used in this study, it also focused on individual gait problems, guided by gait analysis data where available. Cho et al. combined treadmill training and MI training to investigate the effect of MI in chronic stroke (20). Gait training with motor imagery training improved balance and gait abilities significantly more than gait training alone. The results of the current study concur with these findings.
In a review paper Langhorne et al. (29) report that interventions including high-intensity therapy and repetitive task training can improve gait. Mental practice includes both of these intensive and repetitive aspects. In addition, brain imaging studies have confirmed the functional similarity between real walking and imagined walking (30). The literature further suggests that MI shares cortical circuitry with the preparation and execution of motor tasks and increases motor excitability (31, 32). The inclusion of motor imagery alongside physical practice may therefore promote learning by reinforcing processes at the cortical level and by priming neuromotor pathways required for walking performance.
Motor recovery, independent of treatment group, was evident in our study, but we found no statistically significant group interaction effect for motor recuperation, as measured by the Fugl-Meyer assessment. These results contradict the results of other studies (7, 33). In the current study both groups improved, supported by an intensive rehabilitation programme, and so perhaps the contrast between the 2 experimental protocols was not great enough to detect a possible effect of motor recuperation. In addition, the Fugl-Meyer assessment includes several other aspects of motor function that were not addressed in our training protocol. Due to task-specificity of motor learning, this could explain the absence of a significant “between-group” improvement of this parameter. In their study Ietswaart et al. found no effect of motor imagery training in upper extremity function in sub-acute stroke patients (34). Unlike other studies they did not combine physical and mental practice, which may be essential for a possible benefit of this therapy (35). Thus imagery training may represent a complementary technique to actual motor training, but may not replace it. In our study patients were involved in a standard rehabilitation programme that included intensive actual gait training, thus linking the appropriate kinesthetic information directly to the MI. When gait velocity and symmetry were practiced in this study (especially weeks 3 and 4) we also included auditory cueing to guide motor imagery performance. Kim et al. (36) compared 4 imagery protocols and found that the kinesthetic imagery, combined with auditory cueing, provided the largest treatment effect. The use of rhythmic auditory cueing may assist in co-ordinating sequential movements such as walking.
MI training was well tolerated by all participants. Patients involved in MI highly appreciated the training and were highly motivated. They frequently revealed the further use of MI as a strategy in daily activities after finishing the study. Engagement in MI may increase self-efficacy, thus having a positive effect on motivation and self-confidence.
This study has its limitations, in that it involved a relatively small number of patients. It is important to also be aware that the study included a young sub-population of stroke patients. The full potential of MI in older participants has been investigated and imagery capacity seems to decrease with age (37). The inclusion of a younger group of stroke patients may therefore compromise generalisation of our results. In addition, due to the absence of longer term follow-up in our patient cohort as yet, we could not report on this aspect. Finally, although current best-practice for motor imagery was applied, detailed descriptions of MI training elements in neurorehabilitation are still lacking and further research is warranted (38, 39).
In conclusion, this study indicates that patients in a sub-acute phase following stroke have a preserved temporal coupling between real and imagined walking movements. We found significantly lower MI vividness scores in our study cohort, but our results demonstrate that MI vividness can be trained and stimulated to a higher level of performance. These results concur with other studies in chronic stroke regarding motor imagery training as an adjunct to physical practice in gait rehabilitation. Mental practice appears to be an additional gait rehabilitation method in a sub-acute phase following stroke, but further studies are required to examine the long-term benefit of this treatment.
References

