Guido Pasquini, RT, BSc, Federica Vannetti, Eng, PhD and Raffaele Molino-Lova, MD
From the Cardiac Rehabilitation Unit, Don Gnocchi Foundation, Florence, Italy
OBJECTIVE: During maximal incremental exercise, the ability to work in the anaerobic condition, expressed by the respiratory exchange ratio, is associated with physical performance. Further, peak respiratory exchange ratio is regarded as the best non-invasive measure of a patient’s actual exercise effort. This study examined whether ability to work in the anaerobic condition is also associated with physical performance in submaximal constant work rate exercise.
Subjects and methods: A total of 75 older patients (51 men, 24 women), mean age 71.1 years (standard deviation 6.7 years), who had recently undergone cardiac surgery, performed cardiopulmonary exercise testing in a 6-min walk test before and after rehabilitation.
RESULTS: The distance walked, steady-state oxygen uptake, carbon dioxide output and respiratory exchange ratio increased significantly after rehabilitation (p < 0.001 for all). In multivariable models predicting the distance walked before and after rehabilitation, higher steady-state respiratory exchange ratio was independently associated with longer distance (p < 0.001 for both).
CONCLUSION: In older patients receiving post-acute cardiac rehabilitation the ability to work in the anaerobic condition is associated with physical performance in submaximal constant work rate exercises. Thus the steady-state respiratory exchange ratio might be regarded as a measure of the patient’s actual exercise effort. This information may prove useful in customizing exercise prescription and assessing the effects of rehabilitation.
Key words: cardiac rehabilitation; elderly; cardiopulmonary exercise testing; respiratory exchange ratio; 6-minute walk test.
J Rehabil Med 2015; 47: 472–477
Correspondence address: Raffaele Molino-Lova, Cardiac Rehabilitation Unit, Don Gnocchi Foundation, Via di Scandicci snc, 50143 Florence, Italy. E-mail: rmolino@dongnocchi.it; raffmoli@tin.it
Accepted Jan 13, 2015; Epub ahead of print Mar 26, 2015
INTRODUCTION
Following cardiac surgery older patients are commonly referred to medical rehabilitation facilities for post-acute inpatient rehabilitation due to their slower and more complicated recovery (1–3). However, as older patients also have low fitness levels and chronic comorbidities, the intensity of aerobic training, which represents the core of cardiac rehabilitation (3), is often remarkably limited (4).
In these patients physical performance is traditionally assessed using the 6-min walk test (6MWT) (5), a submaximal constant work rate exercise whose work load depends on the patient’s body mass and self-selected walking speed. The 6MWT is safe and well tolerated by older patients; it is regarded as a first-line test in respiratory and cardiac rehabilitation settings: however, it does not provide any objective information on the patient’s actual exercise effort, which is a relevant issue in customizing exercise prescription and assessing the effects of physical training in any single patient.
In maximal incremental exercises, the ability to work in the anaerobic condition, as expressed by the respiratory exchange ratio (RER), is associated with physical performance (6, 7). Further, peak RER is regarded as the best non-invasive measure of the patient’s actual exercise effort (8). This study examined whether the ability to work in the anaerobic condition might also be associated with physical performance in submaximal constant work rate exercises, such as the 6MWT. The hypothesis was tested in a sample of older patients receiving post-acute cardiac rehabilitation.
METHODS
Participants
Participants were enrolled from patients admitted to our rehabilitation centre for a 3-week in-hospital rehabilitation programme after cardiac surgery. Inclusion criteria were: age 65 years or more and having undergone elective cardiac surgery in the previous 7–8 days. Patients with cognitive deterioration (corrected Mini Mental State Examination score < 21) or relevant functional impairment due to previous stroke, peripheral artery disease, severe osteoarthritis of weight-bearing joints or other chronic diseases, such as chronic heart failure or chronic obstructive pulmonary disease, which could, in themselves, remarkably limit physical activity, were excluded from the study. As recommended by the manufacturer, patients with a pacemaker or implantable defibrillator were also excluded, due to possible interference of the portable gas-analyser with cardiac devices. Finally, patients with postoperative sequelae, such as chest-wall or diaphragm mobility impairment, bronchial atelectasis and posture or walking impairment, that were not resolved by intensive individual physiotherapy within the first week after admission, were also excluded in order to obtain a group of patients fit enough to ensure at least 2 weeks of light physical training in the gymnasium. The final study sample was represented by 75 patients (51 men and 24 women) mean age 71.1 years (standard deviation (SD) 6.7 years), age range 65–88 years, all of whom provided signed informed consent.
The study was approved by our Institutional Review Board and involved no discomfort or inherent health risks for participants.
Intervention
A detailed description of the rehabilitation programme performed in our centre is given elsewhere (3, 9, 10). Briefly, our comprehensive rehabilitation programme included optimal medication adjustment, educational and psychological counselling, and physical training.
Physical training was based on 2 1-h sessions per day that included:
• aerobic exercise using cycle ergometry to improve aerobic capacity;
• gentle low-level (approximately 25 W) and short-lasting (1–2 min) callisthenic exercises to improve muscle strength;
• gentle passive stretching involving all the main joints to improve flexibility;
• specific exercises for balance and coordination to prevent falls and mobility disabilities.
Outcome measures
Patients performed the 6MWT as recommended by the American Thoracic Society (11), before and after the rehabilitation programme. Cardiopulmonary exercise testing was performed using a portable gas-analyser (Oxycon Mobile, Jaeger, Germany), calibrated before each test according to the manufacturer’s instructions. The gas-analyser was applied on patients a few minutes before the test, to allow patients’ adjustment to the mask. Gas exchanges were monitored continuously during the 6MWT.
All tests were performed by a physiotherapist in the morning, at least 2 h after a light breakfast. To limit the initial learning effect, a 6MWT without assessment of ventilatory gas exchange was performed the day before baseline assessment.
Oxygen uptake (VO2, ml/kg/min), carbon dioxide output (VCO2, ml/kg/min) and the RER were recorded continuously throughout the 6MWT. Occasional errant breaths, due to swallowing, coughing or talking, were marked by the physiotherapist during the test and removed from the data-set before analysis. The course of VO2 and VCO2 over time were fitted into mono-exponential models using a commercially available software (MatLab, MathWorks, Natick, MA, USA). The “goodness of fit” for models was assessed with the coefficient of determination (R2) and fitting procedures were considered satisfactory if R2 was ≥ 0.85. The same software also provided the graphs reported in Fig. 1. The asymptotic segment of the mono-exponential curve that describes VO2 kinetics during the 6MWT was also checked, by comparing the VO2 at the end of the third minute with that at the end of the test, to ensure that the 6MWT was in fact a submaximal exercise (6, 12) for all patients, both before and after rehabilitation. As VCO2 kinetics physiologically show a longer time constant than VO2 kinetics (13, 14), steady-state VO2, VCO2 and RER were calculated both before and after rehabilitation as the mean values of the last minute of the test.
The level of regular physical activity performed by patients in the year preceding the operation was assessed using a questionnaire modelled on the Harvard Alumni Questionnaire and adapted for Italian people, as described previously (2). All patients underwent echocardiography, using a MyLab30 apparatus (Esaote, Genoa, Italy) equipped with a 2.5 MHz imaging transducer. Left ventricular ejection fraction was assessed using standardized criteria (15). Information on medications was gathered from medical records and the use of beta-blocking agents was considered as a categorical variable.
Statistical analysis
Statistical analysis was performed using STATA 7.0 software (Stata Corporation, College Station, TX, USA). Continuous variables are presented as means and SD. Categorical variables are presented as percentages with absolute value in brackets. The RER was log-transformed before being entered into calculations due to its theoretically asymmetric distribution. Preliminary univariable comparisons before and after rehabilitation of the distance walked on the 6MWT, steady-state VO2, VCO2 and RER, regarded both as a continuous and as a categorical (≤ 1 vs. > 1) variable, were performed using paired Student’s t-test or McNemar’s χ2 test, as appropriate. The distances walked on the 6MWT before and after rehabilitation were entered as dependent variables into 2 multivariable models, along with age, sex, left ventricular ejection fraction, use of beta-blockers and reported physical activity in the year prior to surgery. Steady-state VO2, VCO2 and RER were also entered into the 2 models, before and after rehabilitation, respectively. In the final, multivariable autoregressive model (16) we tested the effects of walked distance and steady-state VO2, VCO2 and RER before rehabilitation on the distance walked afterwards. As RER is a calculated variable (VCO2/VO2), we checked the variance inflation factor for each of the 3 variables to ascertain the degree of structural collinearity among independent variables. Finally, as variables entered into the model were expressed in different units, standardized β-coefficients, i.e. the β-coefficients obtained after standardizing all variables as having a mean of 0 and an SD of 1 (Z-scores), are also reported in order to assess the relative magnitude of the effect of independent variables on the dependent variable.
RESULTS
All patients completed the scheduled rehabilitation programme and no relevant adverse events occurred. Fifty-one patients (68%) reported a sedentary lifestyle or low-intensity physical activity in the year prior to surgery, while 24 (32%) reported moderate-intensity physical activity. Left ventricular ejection fraction was 53.7% (SD 8.6) (reference intervals <30% severely abnormal, 30–44% moderately abnormal, 45–54% mildly abnormal, ≥ 55% normal) (15). Thirty-eight patients (51%) were on beta-blocking agents.
Table I shows the results of the 6MWT before and after rehabilitation. Walked distance and steady-state VO2, VCO2 and RER were all significantly increased after rehabilitation.
|
Table I. Results from the 6-min walk test performed before and after rehabilitation (n = 75) |
||||
|
Before rehabilitation |
After rehabilitation |
Effect size (95% CI) |
pa |
|
|
Distance walked, m, mean (SD) |
324 (79) |
389 (76) |
65 (55–74) |
< 0.001 |
|
Steady-state VO2, ml O2/kg/min, mean (SD) |
10.7 (2.0) |
11.9 (2.7) |
1.24 (0.78–1.70) |
< 0.001 |
|
Steady-state VCO2, ml CO2/kg/min, mean (SD) |
10.1 (2.2) |
12.0 (3.0) |
1.86 (1.32–2.39) |
< 0.001 |
|
Steady-state RER, mean (SD) |
0.94 (0.09) |
1.00 (0.09) |
0.06 (0.04–0.07) |
< 0.001 |
|
Steady-state RER > 1, % (n) |
27 (20) |
49 (37) |
22 (10–35) |
< 0.001 |
|
aFrom paired Student’s t-test or McNemar’s χ2 test, as appropriate. |
||||
Tables II–III show the multivariable models predicting the distance walked on the 6MWT before and after rehabilitation, respectively. In both models VCO2 had to be removed due to structural collinearity. Left ventricular ejection fraction, use of β-blockers and reported level of physical activity in the year prior to surgery were not significant predictors of the distance walked on the 6MWT, while age and female sex were independent negative predictors. The model reported in Table II shows a significant positive association of steady-state VO2 and RER with distance walked before rehabilitation, and that reported in Table III shows a significant positive association of steady-state VO2 and RER with distance walked after rehabilitation. However, the standardized β-coefficient of steady-state RER was greater before rehabilitation, while that of steady-state VO2 was greater afterwards.
|
Table II. Multivariable regression model predicting the distance walked on the 6-min walk test (6MWT) before rehabilitation. Model: Obs =75; F = 18.14; Prob > F < 0.001; adjusted R2 = 0.619 |
|||
|
Distance walked on the 6MWT before rehabilitation (m) |
β (SE β) |
p-value |
Standardized β |
|
Age, years |
–3.61 (0.58) |
< 0.001 |
–0.46 |
|
Female sex, Yes/No |
–39.05 (13.40) |
0.005 |
–0.23 |
|
Left ventricular ejection fraction, % |
0.07 (0.55) |
0.896 |
0.01 |
|
Reported physical activity in the previous year (score 0–4, 4 best) |
–12.18 (14.53) |
0.405 |
–0.07 |
|
Use of beta-blockers, Yes/No |
4.67 (11.49) |
0.686 |
0.03 |
|
Steady-state VO2 before rehabilitation, ml O2/kg/min |
16.45 (2.96) |
< 0.001 |
0.42 |
|
Log-transformed steady-state RER before rehabilitation |
239.33 (69.14) |
0.001 |
0.29 |
|
Steady-state VCO2 before rehabilitation was not entered into the model due to collinearity (variance inflation factor = 179). RER: respiratory exchange ratio; SD: standard deviation; VO2: oxygen uptake; VCO2: carbon dioxide output; SE: standard error. |
|||
|
Table III. Multivariable regression model predicting the distance walked on the 6-min walk test (6MWT) after rehabilitation. Model: Obs = 75; F = 34.78; Prob > F < 0.001; adjusted R2 = 0.762 |
|||
|
Distance walked on the 6MWT after rehabilitation (m) |
β (SE β) |
p |
Standardized β |
|
Age, years |
–3.14 (0.45) |
< 0.001 |
–0.42 |
|
Female sex, Yes/No |
–45.87 (10.49) |
< 0.001 |
–0.28 |
|
Left ventricular ejection fraction, % |
0.57 (0.42) |
0.180 |
0.08 |
|
Reported physical activity in the previous year (score 0–4, 4 best) |
–5.45 (10.10) |
0.592 |
–0.03 |
|
Use of beta-blockers, Yes/No |
9.07 (8.69) |
0.300 |
0.06 |
|
Steady-state VO2 after rehabilitation, ml O2/kg/min |
14.37 (1.80) |
< 0.001 |
0.52 |
|
Log-transformed steady-state RER after rehabilitation |
117.86 (52.91) |
0.029 |
0.14 |
|
Steady-state VCO2 after rehabilitation was not entered into the model due to collinearity (variance inflation factor = 195). RER: respiratory exchange ratio; SD: standard deviation; VO2: oxygen uptake; VCO2: carbon dioxide output; SE: standard error. |
|||
Table IV shows the multivariable autoregressive model predicting the distance walked after rehabilitation based on the walked distance and steady-state VO2, VCO2 and RER assessed during the 6MWT performed before rehabilitation. VCO2 had to be removed from the model due to structural collinearity. Steady-state VO2, use of beta-blockers and reported level of physical activity in the year prior to surgery were not significant predictors of the distance walked after rehabilitation, while age and female sex were independent negative predictors. Left ventricular ejection fraction and distance walked before rehabilitation were independent positive predictors of distance walked after rehabilitation, while steady-state RER was an independent negative predictor: the lower the steady-state RER before rehabilitation, the longer the distance walked in the 6MWT after rehabilitation
|
Table IV. Multivariable autoregressive model predicting the distance walked on the 6-min walk test (6MWT) after rehabilitation. Model: Obs = 75; F = 45.15; Prob > F < 0.001; adjusted R2=0.827 |
|||
|
Distance walked on the 6MWT after rehabilitation (m) |
β (SE β) |
p |
Standardized β |
|
Age, years |
–1.34 (0.47) |
0.006 |
–0.18 |
|
Female sex, Yes/No |
–34.97 (9.18) |
< 0.001 |
–0.22 |
|
Left ventricular ejection fraction, % |
0.97 (0.36) |
0.009 |
0.14 |
|
Reported physical activity in the previous year (score 0–4, 4 best) |
–5.85 (9.43) |
0.537 |
–0.04 |
|
Use of beta-blockers, Yes/No |
2.16 (7.43) |
0.772 |
0.02 |
|
Steady-state VO2 before rehabilitation, ml O2/kg/min |
0.68 (2.31) |
0.769 |
0.02 |
|
Log-transformed steady-state RER before rehabilitation |
–117.81 (48.47) |
0.018 |
–0.15 |
|
Distance walked on the 6MWT before rehabilitation, m |
0.71 (0.08) |
< 0.001 |
0.74 |
|
RER: respiratory exchange ratio; SD: standard deviation; VO2: oxygen uptake; VCO2: carbon dioxide output; SE: standard error. Steady-state VCO2 before rehabilitation was not entered into the model due to collinearity (variance inflation factor = 179). |
|||
The post-hoc statistical power of the multivariable regression models reported in Tables II–IV was > 0.99.
Fig. 1 show some examples of the course of carbon dioxide output kinetics. Carbon dioxide output kinetics show an ascending course and cross oxygen uptake kinetics before the end of the test (Fig. 1a) so that the steady-state RER is > 1. This occurred in 20 patients (27%) before and in 37 patients (49%) after rehabilitation. Carbon dioxide output kinetics show an ascending course, but do not cross oxygen uptake kinetics before the end of the test (Fig. 1b) so that the steady-state RER remains < 1 but is very close to 1. This occurred in 25 patients (33%) before and 17 patients (23%) after rehabilitation. Carbon dioxide output kinetics reach a steady-state phase, as shown in Fig. 1c and the RER is approximately 0.85. This occurred in 30 patients (40%) before and in 21 patients (28%) after rehabilitation.
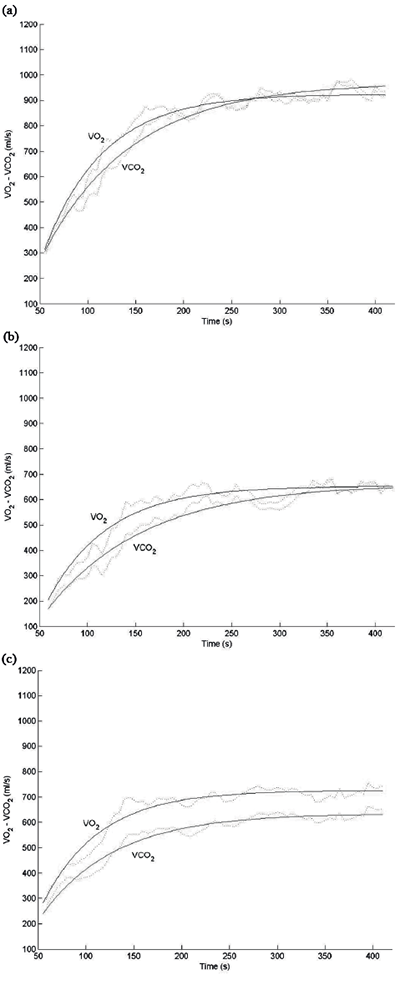
Fig. 1. Three examples of the course of carbon dioxide output. (a) VCO2 kinetics show an ascending course that crosses the oxygen uptake (VO2) kinetics before the end of the test. (b) VCO2 kinetics show an ascending course but do not cross the VO2 kinetics before the end of the test. (c) VCO2 kinetics reach the steady-state phase.
DISCUSSION
This study tested the hypothesis that the ability to work in the anaerobic condition, as expressed by the RER, might also be associated with physical performance in submaximal constant work rate exercises. In a sample of older patients receiving post-acute cardiac rehabilitation we found that both before and after rehabilitation, along with higher steady-state VO2, higher steady-state RER was also independently associated with longer distance walked on the 6MWT.
To the best of our knowledge these findings have not been reported previously, and thus we cannot make direct comparisons with the existing literature; however, a few comments are warranted.
In maximal incremental exercises, either treadmill or cycle ergometry, the assessment of ventilatory gas exchanges provides relevant information, such as the peak VO2, which is a measure that defines the limits of the cardiopulmonary system (7, 10), and peak RER, which is a measure that reflects the ability to work in the anaerobic condition and is regarded as the best non-invasive indicator of a patient’s actual exercise effort (7, 8). In submaximal constant work rate exercises, steady-state VO2, although directly related to walked distance, does not define the limits of the cardiopulmonary system, given the submaximal nature of the test: however, assessment of ventilatory gas exchange still provides useful information. In fact, despite encouragement of the patient, provided by the physiotherapist every minute throughout the test, as recommended by the American Thoracic Society (11), the work load, specifically walking speed, remains under the control of the patient, and the distance walked during the 6MWT might not in itself reflect the patient’s actual exercise effort. Furthermore, neither the CR10 Borg Scale for dyspnoea, which is a subjective rating of perceived exertion (11), nor objective cardiovascular measures, such as heart rate, or the rate-pressure product, can provide information on the patient’s actual exercise effort, given the wide variability of heart rate in the general population and the widespread use of b-blocking agents that blunt the heart rate response to exercise (7). Thus, an objective measure, such as the steady-state RER, has the potential to be an indicator of the patient’s actual exercise effort under submaximal constant work rate exercises, particularly in the 6MWT, in which the work load is self-selected by the patient. Indeed, our findings (Tables II and III) show that both before and after rehabilitation, along with higher steady-state VO2, higher steady-state RER was also independently associated with longer distance walked. On the one hand, this confirms the established notion that steady-state VO2 is a determinant of physical performance and, on the other hand, suggests that steady-state RER can be regarded as an indicator of the patient’s actual exercise effort in submaximal constant work rate exercises. Thus, our finding that the steady-state RER before rehabilitation was an independent negative predictor of distance walked after rehabilitation (Table IV) is not surprising: patients who walked longer distances after rehabilitation were those who engaged less in the test performed earlier. As a consequence, it is likely that these patients received an under-prescription of physical training and that the effects of rehabilitation on their physical performance were overestimated.
The interpretation of our findings in terms of exercise physiology is fairly difficult. In our patients VO2 kinetics satisfactorily fitted the mono-exponential model described by Whipp & Wasserman (12) and showed an asymptotic course in the last 3 min of the test, and therefore we were able to conclude that the 6MWT was a submaximal exercise for our patients (6). However, in a relevant proportion of patients, 60% (n = 45) before and 72% (n = 54) after rehabilitation, VCO2 kinetics did not reach the steady-state phase and showed an ascending course throughout the test, either crossing oxygen uptake kinetics before the end of the test (Fig. 1a) or not (Fig. 1b). Notably, those patients in whom VCO2 kinetics did not cross oxygen uptake kinetics, showed a steady-state RER < 1, but still higher than expected based on the energetic substrates being metabolized (generally, during a 6MWT performed in the morning after a light breakfast the steady-state RER is approximately 0.80–0.85, corresponding to a mixed substrate oxidation of 70% lipids and 30% carbohydrates, and 50% lipids and 50% carbohydrates, respectively, Fig. 1c). A possible explanation of these apparently contradictory findings might be that those patients in whom VCO2 kinetics did not reach the steady-state phase, but showed an ascending course throughout the test, performed the 6MWT very close to the limits of their cardiopulmonary system and that muscle acidosis may have occurred, with consequent formation of additional CO2 from the dissociation of HCO3– during the buffering reaction. Finally, our patients significantly increased steady-state VO2 and steady-state RER after rehabilitation (Table I): however, the relative magnitude of the effect of RER on the distance walked was greater before rehabilitation, while that of VO2 was greater afterwards, as documented by the different standardized β-coefficients (Tables II and III). This suggests that the low-intensity training undertaken by older patients, contrary to the high-intensity training undertaken by endurance athletes (14), affects the aerobic capacity relatively more through improvement of peripheral haemodynamic variables (10), such as endothelial function and arteriolar resistances (17), than the ability to work in the anaerobic condition.
The strength of this study is that it was conducted with patients freely walking overground along a corridor at their self-selected maximal speed, which is a natural task for older persons and shows close similarities to the activities of daily living. However, some limitations must be considered. First, to obtain a group of patients fit enough to ensure at least 2 weeks of light physical training in the gymnasium we introduced a wide series of exclusion criteria, so that our patients represent a selected sample of patients who receive cardiac rehabilitation. The fact that left ventricular ejection fraction was normal or, at most, moderately depressed in all patients, is in fact rather uncommon in everyday clinical practice and is a consequence of our selection criteria. Secondly, patients with chronic heart failure were excluded from the study because, at least for some of them, the 6MWT might be a maximal rather than a submaximal exercise (18–20). Analogous considerations apply for patients with associated chronic obstructive pulmonary disease, who were excluded based on the routine clinical and instrumental functional assessment performed by a specialist in respiratory medicine before cardiac surgery. Thirdly, patients enrolled in this study were all post-surgical older patients receiving in-hospital post-acute rehabilitation, and therefore our results cannot be directly extended to younger patients, to patients attending outpatient cardiac rehabilitation and to patients receiving cardiac rehabilitation for clinical conditions other than cardiac surgery.
In conclusion, our findings show that, in older patients receiving post-acute rehabilitation after cardiac surgery, the ability to work in the anaerobic condition, as expressed by steady-state RER, is also associated with physical performances in submaximal constant work rate exercises, such as the 6MWT. This suggests that steady-state RER might be regarded as a measure of the patient’s actual exercise effort, which would be useful in customizing exercise prescription and assessing the effects of physical training in individual patients. Although the 6MWT in its traditional form remains a first-line test in respiratory and cardiac rehabilitation settings, since portable gas analysers have become more comfortable for patients, more user-friendly for operators and substantially less expensive, due to improvements in technology, the routine assessment of ventilatory gas exchange during the 6MWT should be considered.
REFERENCES

