Mariëtte de Rooij, PT, MSc1, Marike van der Leeden, PhD1,2, Martijn W. Heymans, PhD3, Jasmijn F. M. Holla, PhD1, Arja Häkkinen, PhD4, Willem F. Lems, MD, PhD5, Leo D. Roorda MD, PT, PhD1, Cindy Veenhof, PhD6, Diana C. Sanchez-Ramirez, PT, MPH, PhD7, Henrica C. W. de Vet, PhD3 and Joost Dekker, PhD8
From the 1Amsterdam Rehabilitation Research Centre, Reade, 2Department of Rehabilitation Medicine, VU University Medical Centre, EMGO Institute, 3Department of Epidemiology and Biostatistics, VU University Medical Centre, EMGO Institute for Health and Care Research, Amsterdam, The Netherlands, 4Department of Health Sciences, University of Jyväskylä and Jyväskylä Central Hospital, Jyväskylä, Finland, 5Department of Rheumatology, VU University Medical Centre, Amsterdam, 6Department of Rehabilitation, University Medical Centre Utrecht, Nursing Science and Sports, Utrecht, The Netherlands, 7University of Alberta, School of Public Health, Injury Prevention Centre, Alberta, Canada and 8Department of Rehabilitation Medicine, Department of Psychiatry, VU University Medical Centre, EMGO Institute, Amsterdam, The Netherlands
OBJECTIVE: To systematically summarize the literature on: (i) the course of pain and physical functioning; and (ii) predictors of deterioration of pain and physical functioning in patients with osteoarthritis of the hip.
METHODS: A literature search was conducted in PubMed, CINAHL, Embase, PsychINFO and SPORTDiscus up to July 2015. Meta-analyses and qualitative data syntheses were performed.
RESULTS: Eleven of the 15 included studies were of high quality. With regard to the course of pain and physical functioning, high heterogeneity was found across studies (I2 > 71%) and within study populations (reflected by large standard deviations of change scores). Therefore, the course of pain and physical functioning was interpreted to be indistinct. Clinical characteristics (higher comorbidity count and presence of knee osteoarthritis), health behaviour factors (no supervised exercise and physical inactivity) and socio-demographics (lower education) were found to predict deterioration of pain (weak evidence). Higher comorbidity count and lower vitality were found to predict deterioration of physical functioning (strong evidence). For several other predictive factors weak evidence was found (e.g. bilateral hip pain, increase in hip pain (change), bilateral knee pain, presence of knee osteoarthritis).
CONCLUSION: Because of high heterogeneity across studies and within study populations, no conclusions can be drawn with regard to the course of pain and physical functioning. Several clinical characteristics, health behaviours and psychosocial factors prognosticate deterioration of pain and physical functioning. These findings may guide future research aimed at the identification of subgroups of patients with hip osteoarthritis.
Key words: hip osteoarthritis; longitudinal studies; prognostic factors; pain; physical functioning; review.
J Rehabil Med 2016; 48: 245–252
Correspondence address: Mariëtte de Rooij, Amsterdam Rehabilitation Research Centre Reade, PO Box 58271, NL-1040 HG Amsterdam, The Netherlands. E-mail: m.d.rooij@reade.nl
Accepted Dec 2, 2015; Epub ahead of print Feb 16, 2016
INTRODUCTION
Pain and problems with daily functioning, such as walking, climbing stairs, sitting down and rising from a chair, are common in individuals with hip osteoarthritis (OA). The natural course of pain and physical functioning in OA is highly individual and variable; some patients remain stable, while others improve or gradually worsen (1, 2). Because of this variability, identification of predictors for deterioration in pain and physical functioning is important. Knowledge of predictors can be used to inform patients on the likely course of their condition and to adapt treatment according to the prognosis.
In a previous systematic review, published in 2006, 4 studies on the prognosis of pain and physical functioning in persons with OA of the hip were included (3). Limited evidence (from 1 high-quality study) found that pain and physical functioning did not change from baseline to 3 years’ follow-up, but deteriorated from baseline to 8 years’ follow-up (4). Due to a lack of high-quality studies, no predictive factors could be identified.
Since 2006 a number of longitudinal studies have been published on this topic. We systematically searched the literature and found no reviews on the course and prognosis of pain and physical functioning in persons with hip OA that were published since the previous systematic review in 2006 (3). Therefore, the aims of the present review were: (i) to systematically summarize the literature up to July 2015 on the course of pain and physical functioning in patients with OA of the hip; and (ii) to provide an overview of predictors of deterioration of pain and physical functioning in these patients.
METHODS
Search methods for identification of studies
A protocol for conducting this review was developed with reference to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (5) (protocol not published). The literature was systematically searched from inception up to 9 July 2015, using the following databases: PubMed, CINAHL, Embase, PsychINFO and SportDiscus. The search strategy was formulated in PubMed and, after consultation with an experienced medical librarian, adapted for use in other databases. The search terms were as follows: ((“Osteoarthritis, Hip”[Mesh] OR coxarthr*[tiab]) OR ((hip[tiab] OR hips[tiab] OR lower limb*[tiab] OR lower extremit*[tiab]) AND (osteoarthr*[tiab] OR degenerative arthr*[tiab] OR arthrosis[tiab] OR arthroses[tiab] OR arthralgi*[tiab]))) AND (“activity limitation*”[tiab] OR “functional status”[tiab] OR (activity[tiab] OR activities[tiab]) OR disabilit*[tiab] OR disabled[tiab] OR abilit*[tiab] OR limitation*[tiab] OR (function[tiab] OR functional[tiab] OR functioning[tiab] OR functions[tiab]) OR physical[tiab] OR physical fitness[Mesh] OR activities of daily living [Mesh] OR mobility limitations[Mesh] OR mobilit*[tiab] OR perform*[tiab] OR difficult*[tiab] OR pain[Mesh]) AND (cohort studies[Mesh] OR longitudinal studies[Mesh] OR prospective studies[Mesh] OR follow-up studies[Mesh] OR disease progression[Mesh] OR follow-up[tiab] OR followup[tiab] OR prospective[tiab] OR cohort[tiab] OR progress*[tiab] OR prognos*[tiab] OR longitudinal[tiab] OR predict*[tiab] OR course[tiab] OR risk[tiab]OR determinant*[tiab]) Filters: Humans; Adult: 19+ years. The reference lists of all retrieved prognostic studies were also searched.
Criteria for considering studies for systematic review
Inclusion criteria for the present study were as follows: (i) the study population consisted of patients with: (a) radiographically and/or clinically diagnosed hip OA (as defined by the American College of Rheumatology (ACR) criteria (6), according to Kellgren & Lawrence (K&L) grades (7), or diagnosed by a physician; or (b) a high risk of having hip OA (i.e. having hip symptoms longer than 1 month) (8); (ii) the study used at least 1 measure evaluating pain or physical functioning; (iii) the study addressed changes in pain or physical functioning over a period of 6 months or more; (iv) the study was a prospective cohort study (or analysed as a prospective cohort study when the data was obtained from a clinical trial); (v) separate analyses were presented for hip OA in case a mixed hip and knee OA population was included in the study; and (vi) the study was reported in the format of a full-text article. Review articles were excluded. If studies on the same cohort presented different information, or reported on different predictors, or presented results after different follow-up periods, all studies were included (see METHODS: data analysis).
The studies were selected independently by 2 reviewers (MR and ML), using the criteria described above. If agreement was not achieved, a third reviewer (JH) was consulted, who made the final decision.
Data extraction
Two reviewers (MR and ML) systematically extracted the following information from the included studies: authors, year of publication, setting, study population, study design, timing of outcome assessment, outcome measures, mean and standard deviation (SD) or the percentage of change in pain and physical functioning (pre- and post- values), and predictive factors (univariate and multivariate associations (odds ratio (OR), relative risk (RR), beta coefficient)). The threshold level of significance of a predictor was set at p ≤ 0.05. A non-significant association between a baseline characteristic and the outcome was regarded as an indication that this characteristic did not predict the outcome.
Methodological quality
The methodological quality of the selected studies was assessed independently by 2 reviewers (MR and ML) using the Hayden criteria (9). The Hayden criteria are appropriate to assess the methodological quality of studies on prognosis and predictive factors, and pertain to 6 areas of potential bias related to: (i) participation, (ii) study attrition, (iii) measurement of predictive factors, (iv) outcome measurement, (v) confounding, and (vi) analysis. We did not rate the risk of bias of confounding, because the aim of a predictive model is to estimate the probability of a particular outcome and not to explore the causality of the association between a specific factor and the outcome. The risk of bias of all 5 areas was rated as low, moderate, or high. As recommended by Hayden et al. (9), the studies were classified as being of high quality if, in all 5 areas, there was a low or a moderate risk of bias. Studies with a high risk for at least one area of bias were defined as low-quality studies. In case of disagreement between both reviewers, a third reviewer (JH) was consulted in order to achieve a final judgement.
Data analysis
A quantitative data analysis (meta-analysis) was planned when homogeneity in study design, population, measured determinants and assessed outcome was assumed. Data of the course or predictors were regarded eligible for pooling if a minimum of 3 studies with eligible data were available and sufficient data (means and SDs of the baseline and follow-up measurement or change scores between baseline and follow-up with SD, or OR, RR or regression coefficients, respectively) were presented in each individual study. In case of predictors, when univariable results were available, these were used for pooling: otherwise the multivariable estimates were used.
Pooling of effect sizes across studies was done using the standardized mean change (SMC), log ORs, RRs, or standardized coefficients in a random effects model, weighted by the inverse variance (10). The results were presented in a forest plot. Heterogeneity among studies was tested using the I2 statistic (11). The literature suggests 25% as low heterogeneity, 50% as moderate, and 75% as high (11).
In case of sufficient number of studies a sensitivity meta-regression analysis of the course of pain and physical functioning were planned using a random-effects model to examine the effects of: (i) follow-up length (shorter than 3 years vs longer than 3 years), (ii) study population (radiographically or clinically diagnosed hip OA vs hip pain population), and (iii) quality of studies (high vs moderate/low quality) on the outcome. Finally, data from included studies were entered into a funnel graph (a scatter-plot of study effects against a measure of study sizes) in order to investigate the likelihood of publication bias (12).
In case of absence of homogeneity or insufficient number of studies, a qualitative data analysis (best-evidence synthesis) was planned to summarize the data. Five levels of evidence (strong, moderate, weak, inconclusive, and inconsistent) were defined to summarize the available evidence for the predictive value of identified predictors (13, 14) (Table I). In order to establish levels of evidence, the number of studies, the methodological quality of the studies, and the consistency of a predictor for the outcome were taken into account. Findings were deemed to be consistent if, in more than 75% of the studies reporting on a predictor, the direction of the association was the same (15). In cases where studies were based on the same database we used the results of the study: (i) with the highest quality rating, (ii) that reported univariate instead of multivariate associations, or (iii) with the longest follow-up period. In describing the results, a distinction was made between self-report and performance-based outcome measurements.
|
Table I. Levels of evidence for predictors of pain and physical functioning in persons with hip osteoarthritis (OA) |
|
|
Level of evidence |
|
|
Statistically significant associations |
|
|
Strong |
Consistent significant associations found in at least 2 high-quality studies |
|
Moderate |
Consistent significant associations found in 1 high-quality study and at least 1 low-quality study |
|
Weak |
Significant association found in 1 high-quality study or consistent significant associations found in at least 3 low-quality studies |
|
Inconclusive |
Significant association found in fewer than 3 low-quality studies |
|
Inconsistent |
Inconsistent significant findings irrespective of study quality |
|
Statistically non-significant associations |
|
|
Strong |
Consistent non-significant associations found in at least 2 high-quality studies |
|
Moderate |
Consistent non-significant associations found in 1 high-quality study and at least 1 low-quality study |
|
Weak |
Non-significant association found in 1 high-quality study or consistent non-significant associations found in at least 3 low-quality studies |
|
Inconclusive |
Non-significant associations found in fewer than 3 low-quality studies |
|
Inconsistent |
Inconsistent non-significant findings irrespective of study quality |
RESULTS
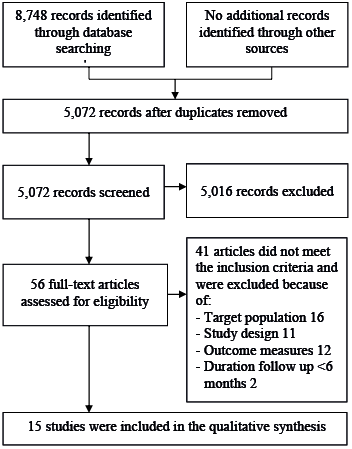
The literature search resulted in a total number of 8,748 hits. After duplicate removal, 5,072 hits were screened on title and abstract. This resulted in 56 full-text articles that were studied for eligibility, of which 15 articles were included in the present study (see Fig. 1).
Study characteristics
Thirteen (2, 4, 16–26) out of the 15 studies included patients diagnosed according to the ACR criteria or K&L grade (of which 2 studies included patients with severe hip OA) (21, 22). Two studies included patients who were at risk for having hip OA (8, 27). There was considerable variation across studies regarding sample size and length of follow-up. The sample size ranged from 20 to 745 subjects. The mean follow-up ranged from 0.5 to 8 years, of which 4 studies had a follow-up longer than 3 years (4, 16, 19, 23). All 15 included studies were analysed as prospective cohort studies. A detailed description of the included studies is presented in Table SI1.
Methodological quality
Different categories of bias were rated. Overall agreement on methodological quality scores between reviewers was 93.7%. The disagreement mainly concerned the rating of participation and attrition of patients. No consultation of a third reviewer was necessary to resolve disagreement. Eleven studies were considered to be of high quality (2, 8, 16–18, 21, 23–27), and 4 were of low quality (4, 19, 20, 22) (see Table SII1).
Course of hip pain and physical functioning
Four (17, 21, 22, 27) out 6 studies (4, 17, 20–22, 27) reporting on the course of hip pain were included in the meta-analysis (of which 3 were high-quality studies). There was evidence of high statistical heterogeneity across studies (I2 = 71.16%, p = 0.02) (see Fig. 2). Also large SDs of change scores were seen within studies. For example, in the study of Botha-Scheepers et al., the mean change and SD of hip pain was 0.38 (SD 2.3) (27). Six (8, 17, 19, 21–23) out of 7 studies reporting on the course of physical functioning were included in the meta-analysis (8, 17, 19, 21–23, 25) (of which 4 were high-quality studies). Again, we found evidence of high statistical heterogeneity across studies (I2 = 96.98%, p < 0.01) (see Fig. 2) and large SDs of change scores within studies (8). Neglecting the heterogeneity, the results would suggest that the mean course of pain and physical functioning is stable over time: for hip pain SMC = 0.06; 95% confidence interval (95% CI) –0.13 to 0.26, for physical functioning SMC = –0.11; 95% CI –0.38 to 0.15 (see Fig. 2).
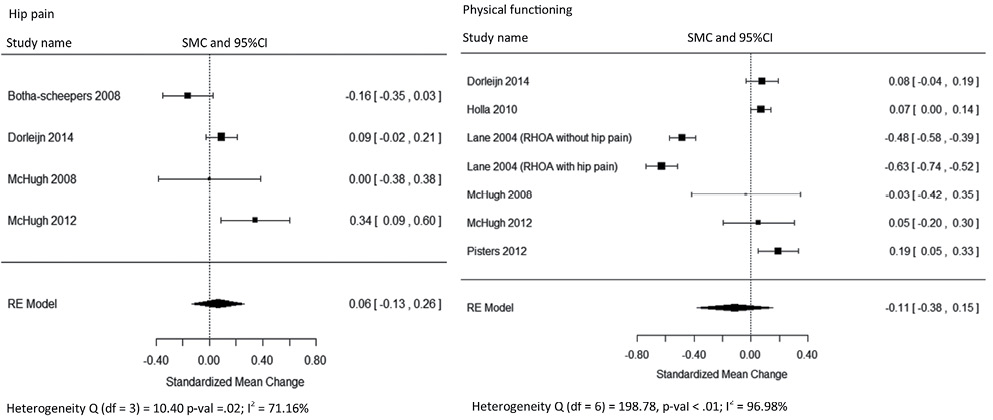
Fig. 2. Standardized mean change (SMC) of the overall course of knee pain and physical functioning in patients with hip osteoarthritis (OA). A positive mean change score indicates improvement in pain or physical functioning and a negative mean change score indicates deterioration in pain or physical functioning.
Sensitivity analyses on the course of hip pain and physical functioning
With regard to the course of pain, it was not possible to perform a meta-regression for sensitivity analysis due to a low number of available studies. With regard to the course of physical functioning, no factors (effects of follow-up length, study quality) were identified in the meta-regression that could account for the study heterogeneity. Sensitivity analysis based on study population (radiographically or clinically diagnosed hip OA vs hip pain population) was not possible because only one study included patients with hip pain.
Egger’s test provided evidence for no publication bias in the course of physical functioning (data not shown).
Predictors for deterioration of pain
Two high-quality studies (18, 24) assessed a total of 15 predictive factors for deterioration of hip pain. We considered a meta-analysis of predictors of deterioration of pain inappropriate because the predictors under study were measured in fewer than 3 studies, or there were differences in definitions of determinants under study or effect estimates, which hamper calculation of pooled effect estimates. We therefore performed a qualitative data synthesis (best-evidence synthesis). Weak evidence was found for the following factors as predictors for deterioration of hip pain: additional knee OA, higher comorbidity count, no supervised exercise, lower level of physical activity and lower level of education (see Table II).
|
Table II. Results of the qualitative data analysis on studies describing predictors for deterioration of pain in patients with hip osteoarthritis (18) |
||
|
Predictors for deterioration of hip pain |
Level of evidence |
Uni- and/or multi-variable association (number of variables in multivariable model) |
|
Other patient characteristics Lower level of education |
Weak |
Multi (11) |
|
Clinical factors Higher comorbidity count |
Weak |
Multi (11) |
|
Presence of additional knee osteoarthritis |
Weak |
Multi (11) |
|
Health behaviour factors No supervised exercise |
Weak |
Multi (11) |
|
Lower level of physical activity |
Weak |
Multi (11) |
|
Uni: univariable association; Multi: multivariable association. See Table SIII1 for variables not predicting pain. |
||
Strong evidence was found that deterioration of pain is not predicted by sex, age, body mass index (BMI), duration of hip symptoms and radiological OA (K&L grade). For other variables weak or inconsistent evidence for being not predictive was found (Table SIII1).
Predictors for deterioration of physical functioning
Eight studies (of which 1 was a low-quality study) assessed a total of 62 predictors for deterioration of physical functioning (8, 16, 18, 19, 23–26). For the same reasons as above we considered a meta-analysis of predictors of deterioration of physical functioning inappropriate. We therefore performed a qualitative data synthesis (best-evidence synthesis). Strong evidence was found that self-reported deterioration of physical functioning is predicted by higher comorbidity count and low vitality. Furthermore, weak evidence was found that self-reported deterioration of physical functioning is predicted by having moderate or severe cardiac disease or eye-ear-nose throat disease, poor general health, the presence of bilateral hip pain, increase in hip pain (change), bilateral knee pain, additional knee OA, morning stiffness of the hip or knee, decrease in external hip rotation (ROM) (change), reduced knee extension (ROM) (at baseline), decrease in knee extension (ROM) (change), no supervised exercise, a lower level of physical activity, more avoidance of activities and having high bodily pain. For performance-based physical functioning, weak evidence for being predictive was found for more disability at baseline, lower walking speed, higher comorbidity count and having moderate or severe cardiac disease or eye-ear-nose throat disease and reduced hip abduction muscle strength (Table III). For other variables inconsistent evidence was found (see Table SIV1).
|
Table III. Qualitative data analysis of studies describing predictors for deterioration of physical functioning in patients with hip osteoarthritis |
||||
|
Predictors for deterioration of physical functioning |
Outcome measurement |
Level of evidence |
Uni- and/or multi-variable association (numberr of variables in multivariable model) |
Reference |
|
Socio-demographics Older age |
Performance-based outcome |
Inconsistent |
uni, multi (5) uni, multi (?) multi (5) ns |
Pisters et al., 2012 (23) van Dijk et al., 2010 (25) Steultjens et al., 2001 (24) |
|
Lower level education |
Self-reported outcome |
Inconsistent
|
uni ns multi (11) multi (6) |
Holla et al., 2010 (8) Juhakoski et al., 2013 (18) Pisters et al., 2012 (23) |
|
Clinical characteristics – other More disability |
Self-reported outcome |
Inconsistent |
uni, multi (6) ns uni, multi (6) |
Holla et al., 2010 (8) van Dijk et al., 2010 (25) |
|
More disability |
Performance-based outcome |
Weak |
multi (5) |
Steultjens et al., 2001 (24) |
|
BMI |
Self-reported outcome |
Inconsistent |
uni uni ns multi (11) ns |
Holla et al., 2010 (8) Pisters et al., 2012 (23) Juhakoski et al., 2013 (18) |
|
Higher comorbidity count |
Self-reported outcome |
Strong |
uni, multi (6) uni, multi (6) multi (11) multi (11) ns multi (6) |
Holla et al., 2010 (8) van Dijk et al., 2010 (25) Juhakoski et al., 2013 (18) Juhakoski et al., 2013 (18) Pisters et al., 2012 (23) |
|
Higher comorbidity count |
Performance-based outcome |
Weak |
uni, multi (6) multi (5) |
van Dijk et al., 2010 (25) Pisters et al., 2012 (23) |
|
Having moderate or severe cardiac disease and eye-ear-nose throat disease |
Self-reported outcome/ performance-based |
Weak |
uni, multi (?) |
van Dijk et al., 2010 (25)
|
|
Presence of CIRS 1, 6 (CIRS ≥ 2) |
Self-reported outcome |
Weak |
uni |
van Dijk et al., 2010 (25) |
|
Presence of CIRS 1, 4, 5, 12, 13 (CIRS ≥ 2) |
Performance-based outcome |
Weak |
uni |
van Dijk et al., 2010 (25) |
|
Poor general health perception |
Self-reported outcome |
Weak |
uni, multi (7) |
Holla et al., 2010 (8) |
|
Lower walking speed |
Performance-based outcome |
Weak |
uni, multi (4) |
van Dijk et al., 2010 (25) |
|
Clinical characteristics – hip Increase in hip pain (change from t0 to t1) |
Self-reported outcome |
Weak |
uni, multi (6) |
van Dijk et al., 2010 (25) |
|
Higher hip pain at baseline (VAS score) |
Self-reported outcome |
Inconsistent |
uni ns uni ns multi (8) multi (6) |
Holla et al., 2010 (8) van Dijk et al., 2010 (25) Lane et al., 2004 (19) Pisters et al., 2012 (23) |
|
Morning stiffness hip ≤ 60 min |
Self-reported outcome |
Weak |
uni |
Holla et al., 2010 (8) |
|
Bilateral hip pain with equal symptoms vs no pain |
Self-reported outcome |
Weak |
uni, multi (6) |
Holla et al., 2010 (8) |
|
Decrease in hip external rotation (ROM) (change from t0 to t1) |
Self-reported outcome |
Weak |
multi (6) |
Pisters et al., 2012 (23) |
|
Reduced muscle strength hip abduction |
Performance based |
Weak |
uni, multi (3) |
Pisters et al., 2014 (16) |
|
Reduced hip flexion (ROM) at baseline |
Self-reported outcome |
Inconsistent |
uni, multi (6) multi (6) ns |
Holla et al., 2010 (8) Pisters et al., 2012 (23) |
|
Clinical characteristics – knee Presence of additional knee osteoarthritis |
Self-reported outcome |
Weak |
multi (11) |
Juhakoski et al., 2013 (18) |
|
Bilateral knee pain with index knee vs no pain |
Self-reported outcome |
Weak |
uni |
Holla et al., 2010 (8) |
|
Morning stiffness knee < 30 min |
Self-reported outcome |
Weak |
uni, multi (6) |
Holla et al., 2010 (8) |
|
Reduced knee extension (ROM) at baseline |
Self-reported outcome |
Weak |
uni multi (6) ns |
van Dijk et al., 2010 (25) Pisters et al., 2012 (23) |
|
Decrease in knee extension (ROM) (change from t0 to t1) |
Self-reported outcome |
Weak |
uni |
van Dijk et al., 2010 (25) |
|
Health behaviour factors No supervised exercise |
Self-reported outcome |
Weak |
multi (11) |
Juhakoski et al., 2013 (18) |
|
Lower level of physical activity |
Self-reported outcome |
Weak |
multi (11) |
Juhakoski et al., 2013 (18) |
|
Psycho-social factors Poorer cognitive functioning |
Self-reported outcome |
Inconsistent |
uni, multi (6) multi (6) ns |
van Dijk et al., 2010 (25) Pisters et al., 2012 (23) |
|
High bodily pain |
Self-reported outcome |
Weak |
uni, multi (6) |
Holla et al., 2010 (8) |
|
Lower vitality (SF-36) |
Self-reported outcome |
Strong |
uni uni |
Holla et al., 2010 (8) van Dijk et al., 2011 (26) |

|
Table III. Contd. |
||||
|
Predictors for deterioration of physical functioning |
Outcome measurement |
Level of evidence |
Uni- and/or multi-variable association (numberr of variables in multivariable model) |
Reference |
|
More avoidance of activity |
Self-reported outcome |
Weak |
multi (6) uni, multi (3) |
Pisters et al., 2012 (23) Pisters et al., 2014 (16) |
|
More avoidance of activity |
Performance-based outcome |
Inconsistent |
uni ns multi (5) uni, multi (3) |
Steultjens et al., 2001 (24) Pisters et al., 2012 (23) Pisters et al., 2014 (16) |
|
Resting |
Self-reported outcome |
Inconsistent |
uni uni ns |
Holla et al., 2010 (8) van Dijk et al., 2011 (26) |
|
Transformation |
Self-reported outcome |
Inconsistent |
uni uni ns |
Holla et al., 2010 (8) van Dijk et al., 2011 (26) |
|
SF-36: Short-Form 36 Health Survey; VAS: visual analogue scale; BMI: body mass index; CIRS: Cumulative Illness Rating Scale; (?): not known; ns: not significant; ROM: range of motion; t0 to t1: change from baseline to follow-up; Uni: univariable association; Multi: multivariable association. Predictor in bold represents strong level of evidence. See Table SIV for variables not predicting physical functioning. |
||||
Strong evidence for being not predictive for self-report physical functioning was found for age, sex, household composition > 1, employment status, duration of complaints, radiological hip OA (K&L grade), internal hip rotation (ROM), social support, mental health and specific coping strategies (distraction, retreating and worrying). For performance-based physical functioning, strong evidence for being not predictive was found for sex, BMI, duration of complaints, radiological hip OA (K&L grade), specific coping strategies (resting, transformation, reducing demands). For other variables weak or inconsistent evidence for being not predictive was found (see Table SIV1).
DISCUSSION
The aim of this study was to describe the course of pain and physical functioning and to identify predictors of the course of hip OA through a systematic review of the literature. In all, 15 studies were included in this review, of which 11 were of high quality.
With regard to the course of pain and physical functioning we conclude that the course was found to be indistinct over time, because of high heterogeneity across studies and within study populations. Heterogeneity was not reduced by taking into account methodological issues, such as length of follow-up or quality of the study. Furthermore, it was found that individual patients show considerable variation in the course of physical functioning; some patients improve, while others remain stable or deteriorate. A statement on the mean course neglects these between-patient differences. Interestingly, similar conclusions were drawn in our study in patients with knee OA (28). It has been hypothesized that the OA population actually consists of homogeneous subgroups or phenotypes (29). This hypothesis is supported by Verkleij et al. (2), who identified subgroups based on the 2-year course of pain in patients with clinically and radiographically determined hip OA. They identified 5 subgroups consisting of patients with mild pain, moderate pain, continuous pain, regularly progressing pain, or highly progressing pain (2). Our findings underline the importance of identifying predictors for deterioration of pain and physical functioning, and support the need for research aimed at the identification of subgroups or phenotypes in patients with hip OA.
Our results indicate that deterioration of hip pain is predicted by clinical characteristics (higher comorbidity count, additional presence of knee OA), health behaviour factors (no supervised exercise and a lower level of physical activity) and socio- demographics (lower level of education) (weak evidence). However, as these conclusions are derived from only 1 high-quality study they must be interpreted with caution. Deterioration in physical functioning has been investigated in 8 studies (of which 7 were high-quality studies) and is predicted by higher comorbidity count and lower vitality (strong evidence). We found weak evidence for prediction of deterioration in physical functioning for certain clinical characteristics of the hip (e.g. presence of bilateral hip pain, reduced hip flexion), clinical characteristics of the knee (e.g. bilateral knee pain, decrease in knee extension (ROM)), health behaviour factors (e.g. no supervised exercise), and psycho-social factors (i.e. more avoidance of activities). As consistent with knee OA, we found strong evidence that K&L grade did not predict deterioration in physical functioning (28). This finding is in contrast with the review of Wright et al., who found strong evidence that K&L hip grade 3 is of predictive value of poorer outcome or progression of hip OA (30). This discrepancy is probably related to the use of different outcome measures. We used deterioration in physical functioning as a main outcome measure, while Wright et al. (30) focused mainly on radiographic progression. In addition, it might be that sensitive methods (e.g. magnetic resonance imaging (MRI)), rather than K&L grade have a predictive value.
Some of the identified predictive factors have implications for treatment possibilities and planning. We found that performing no supervised exercise predicts deterioration in pain and in physical functioning. Indeed, land-based exercise has been proven to reduce pain and improve physical functioning in patients with hip OA (31). Furthermore, we found that a higher comorbidity count predicts deterioration in pain and physical functioning. In OA the presence of comorbidity is highly prevalent (32). Comorbidities have a significant influence on prognosis and may influence treatment outcome, therefore they should be closely monitored and managed. In addition, the presence of comorbidity may interfere with treatment possibilities, e.g. exercise therapy. It may be necessary to adapt the OA exercise programme to the comorbid disease in order to avoid serious adverse events (33, 34). Finally, low vitality predicts deterioration in physical functioning. The mechanism behind this can be 2-fold. First, low vitality is associated with avoidance of activities (35) and may reduce the level of physical activity, which in itself can result in decreased muscle strength and deconditioning. Secondly, low vitality is associated with depression (36, 37), which is also related to a lower level of physical activity (38). Both mechanisms can result in deterioration in physical functioning and pain. Behavioural interventions with or without exercise have been proven to positively affect these factors and thereby the course of hip OA (39–41).
Some limitations of the present study must be considered. First, shortcomings in the included studies may have influenced the outcome of this study. Four out of 15 studies were classified as low-quality studies. We found a high risk of bias particular in the description of the study population and study attrition. Improving the report on the selection of participants and reasons for drop-out or loss to follow-up will prevent bias and will allow stronger conclusions. Secondly, it was not possible to pool the data to quantify the strength of relationships between predictors and outcomes due to the small number of studies included, the variety of variables investigated and the different outcome measures that were used. The same limitation we found in analysing predictors of deterioration in pain and physical functioning in patients with knee OA (28). Thirdly, we included studies that used longitudinal data analyses to predict future pain or physical functioning. However, in some studies, using linear mixed models for repeated measurements, it appeared that the relationship between the determinant and the outcome was analysed cross-sectionally on different measurement points. In that case the determinant cannot be considered as a predictor of future pain or physical functioning. We therefore excluded these studies (17, 42). Fourthly, the conclusions are preferably based on the results from univariable analyses, due to the considerable diversity in statistical techniques and choice of covariates used in individual multivariate models. Where univariable effect estimates were not available, we used multivariable effect estimates. This may have influenced the results, because risk factors (if adjusted for potential confounders) have different effect estimates compared with the univariable effect estimates. Fifthly, only 15 studies generated evidence for the course or predictors of deterioration in hip pain or physical functioning in patients with hip OA. To strengthen the evidence, more high-quality longitudinal studies are needed with more uniformity in investigated predictors, measurement outcomes and used definitions of determinants.
In conclusion, because of high heterogeneity across studies and within study populations, no conclusions can be drawn with regard to the course of pain and physical functioning. Several clinical characteristics, health behaviours and psychosocial factors predict deterioration of pain and physical functioning. These findings may guide future research aimed at the identification of prognostically homogeneous subgroups of patients with hip OA.
ACKNOWLEDGEMENTS
The authors would like to thank DG de Rooij, PhD, for advice and critical reading of the manuscript. René Otten and Remke Albers for their contribution as medical information specialists regarding the literature search. This study was financially supported by the Royal Dutch Society for Physical Therapy.

1http://www.medicaljournals.se/jrm/content/?doi=10.2340/16501977-2057
REFERENCES


