
From the 1Clinical Research Center, Institute of Physical Medicine and Rehabilitation, 2Institute of Physical Medicine and Rehabilitation, 3Department of Orthopedics and Traumatology, University of São Paulo School of Medicine, São Paulo, Brazil, 4Extracorporeal Shock Wave Research Unit, Department of Anatomy II, Ludwig-Maximilians-University of Munich, Munich, Germany and 5School of Medicine, University of São Paulo, São Paulo, Brazil
Objective: To assess the efficacy and safety of radial extracorporeal shock wave therapy (rESWT) for disabling pain due to primary knee osteoarthritis.
Design: Randomized, placebo-controlled trial (level of evidence, 1).
Subjects: A total of 105 women with disabling pain due to primary knee osteoarthritis lasting for a mean of 103 months (range 3–480 months).
Methods: Patients received either rESWT (3 sessions, each one week apart, 2,000 rESWT impulses per session, positive energy flux density 0.10–0.16 mJ/mm2) or placebo treatment. Primary outcome measure was pain on movement 3 months after the final treatment session. Secondary outcomes were pain, stiffness and limitations in physical function on the Western Ontario and McMaster Universities Osteoarthritis (WOMAC) Index and the level of tolerance to pressure over muscles, tendons, ligaments and skin at both the treated and the untreated side at 1 week and 3 months follow-up examinations.
Results: Compared with placebo treatment, rESWT led to a statistically significant improvement only in mean WOMAC scores for pain and a few of the pressure measurements.
Conclusion: rESWT, as performed in the present study, is not efficient for treating patients with disabling pain due to primary knee osteoarthritis. Published data indicate that substantially higher energy flux densities are necessary for treatment success in this condition.
Key words: extracorporeal shock wave therapy; knee osteoarthritis; radial extracorporeal shock wave therapy; rehabilitation.
Accepted Aug 17, 2016; Epub ahead of print Nov 30, 2016
J Rehabil Med 2017; 49: 54–62
Correspondence address: Marta Imamura, Clinical Research Center, Institute of Physical Medicine and Rehabilitation, University of São Paulo School of Medicine, Rua Domingo de Soto 100, Vila Mariana, 04116-030 São Paulo, SP, Brazil. E-mail: marta.imamura@fm.usp.br
Osteoarthritis (OA) is the most common cause of pain and disability worldwide (1), especially in the elderly population (2, 3). Women are affected more frequently than men (4), and the hip and knee joints are most commonly affected (5). Despite its high prevalence and negative impact on quality of life of affected individuals, there is no cure for OA (2, 3). Therapeutic measures aim to relieve painful symptoms and maximize functional capacity and quality of life, while minimizing adverse effects from drugs and invasive interventions (6). Patients worldwide with knee OA reporting severe disabling and refractory pain are usually referred for a total or partial arthroplasty (7, 8).
Total knee replacement has been shown in a recent study to result in greater pain relief and functional improvement after 12 months than non-surgical treatment involving exercise, education, dietary advice, use of insoles and pain medication (8). However, total knee replacement was associated with a higher number of serious adverse events than the non-surgical treatment (8). Thus, and since total knee replacement may not be possible due to the patient’s medical condition, or the limited availability and/or expense of the procedure, there is a need for alternatives to surgery for the treatment of knee OA. Extracorporeal shock wave therapy (ESWT) is one of the best investigated treatment modalities for various musculoskeletal conditions (for reviews see, e.g. 9–12). Extracorporeal shock waves are acoustic high-pressure waves generated by electrohydraulic, electromagnetic, piezoelectric or ballistic/radial methods (11–16). Experimental studies in animal models have indicated that ESWT may be effective in treating disabling pain due to primary OA (17–20). This was corroborated by 2 randomized controlled trials (RCTs) in which ESWT was used successfully to alleviate pain in patients with knee OA (21, 22). However, these RCTs varied considerably with respect to the applied shock wave energy (the total applied energy flux density varied between 120 and 4,000 mJ/mm2). Furthermore, none of these RCTs adhered to the Consolidated Standards of Reporting Trials (CONSORT) Statement, which is an evidence-based, minimum set of recommendations for reporting RCTs (23) (for example, in none of these RCTs was a power analysis reported). Thus, it is not known whether ESWT is an effective and safe treatment for disabling pain due to severe primary knee OA.
The present RCT evaluated the efficacy of a radial ESWT (rESWT) protocol (3 sessions, each 1 week apart, 2,000 impulses each, positive energy flux density (positive EFD) 0.10–0.16 mJ/mm2) in reducing pain and improving knee function in patients with disabling pain due to severe primary knee OA. This rESWT protocol represents the mean number of rESWT sessions, the mean interval between sessions, the mean number of impulses per session, and the mean positive EFD applied in 23 RCTs on rESWT for tendon and other pathologies of the musculoskeletal system with positive outcome (i.e. rESWT statistically significantly better than either placebo or alternative treatment modalities) (12). Based on the outcome of the aforementioned RCTs (21, 22), in which ESWT was successfully used to alleviate pain in patients with knee OA, we hypothesized that the outcome of the rESWT protocol in the current study would be superior to placebo treatment.
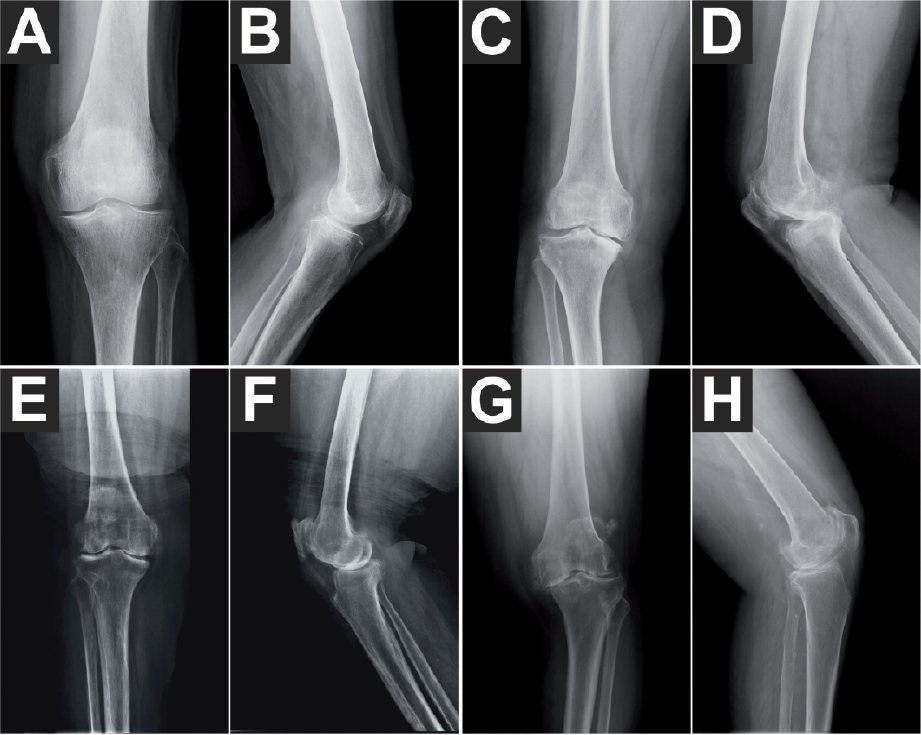
A total of 237 female patients with disabling pain due to severe primary knee OA were assessed between May 2010 and October 2012 for eligibility for enrollment in the present study. Patients of any race and ethnicity were eligible to participate. Some patients were from the waiting list for total knee replacement at the Department of Orthopedics and Traumatology, University of São Paulo School of Medicine, São Paulo, Brazil. Other patients were from the community of São Paulo and referred to the Institute of Physical Medicine and Rehabilitation, University of São Paulo School of Medicine. Thus, the patients assessed for eligibility for enrollment in the present study were representative of the citizens of São Paulo, Brazil. Patients were diagnosed based on their medical history and physical examination at the Department of Orthopedics and Traumatology and the Institute of Physical and Rehabilitation Medicine at the University of São Paulo School of Medicine. Radiographs showed signs of knee OA according to Kellgren & Lawrence (24) grades 2–4 as well as knee deformities. However, individual Kellgren & Lawrence (24) grades were not used to make decisions about eligibility for enrollment in the present study because of the known discordance between pain and radiographic severity in knee OA (25), which was also found in the present study (Fig. 1). The same reasoning applied to the presence or absence of knee deformities (Fig. 1). All patients had undergone 2 or more types of conservative treatment (medications, anti-inflammatory drugs, physical therapy, stretching, acupuncture, orthotics, and others) without success. Patients were considered for participation in the present study according to the inclusion and exclusion criteria summarized in Table I.
Fig. 1. Standard anterior-posterior (A, C, E, G) and lateral (B, D, F, H) radiographs of representative patients with disabling pain due to severe primary knee osteoarthritis (OA) enrolled in the present study. All patients were female. (A, B) 73-year-old, left knee, pain for 10 months, visual analogue scale (VAS) score = 9.9, Kellgren-Lawrence (KL) grade = 2, no knee deformity. (C, D) 60-year-old, right knee, pain for 60 months, VAS score = 9.5, KL grade = 4, genu varum. (E, F) 74-year-old, right knee, pain for 12 months, VAS score = 5.8, KL grade = 2–3, no knee deformity. (G, H) 72-year-old, left knee, pain for 24 months, VAS score = 5.0, KL grade = 4, genu varum. Note that there was no correlation between the individual VAS score on the one hand and the individual KL grade and the presence or absence of knee deformities on the other hand. The final figure was constructed using Corel Photo-Paint X6 and Corel Draw X6 (both versions 16.1.0.843; Corel, Ottawa, Canada). Only minor adjustments of contrast and brightness were made, without altering the appearance of the original materials.
Table I. Inclusion and exclusion criteria for patients with primary knee osteoarthritis (OA) enrolled in the present study
Patients were allowed to withdraw their free and informed consent to participate in the present study at any time. The study was approved by the Ethics Committee for Analysis of Research Projects (CAPPesq), Hospital of Clinics, University of São Paulo Medical School, São Paulo, Brazil (CAPPesq 0130/10) and was carried out in accordance with the World Medical Association Declaration of Helsinki (26). The study has been registered with ClinicalTrials.gov (identifier NCT02197962).
Before randomization, 132 of the 237 patients assessed for eligibility chose to withdraw, declined to sign the consent form, or were excluded because they did not meet the inclusion criteria. After having obtained written informed consent from each of the remaining 105 patients, they were randomly assigned to receive either rESWT (n = 52) or placebo treatment (n = 53). Randomization was performed by a person who was not involved in the study, at the Institute of Physical and Rehabilitation Medicine at the University of São Paulo School of Medicine (São Paulo, Brazil), using a computerized random number generator. The randomization numbers were placed in sealed opaque envelopes, thus concealing allocation from both patients and therapists until treatment started.
The characteristics of the included patients at baseline are shown in Table II. These patients had disabling pain for between 3 and 480 months (25th percentile 48 months, median 72 months, 75th percentile 132 months).
Table II. Characteristics of included patients at baseline (intention-to-treat population)
The intervention group received rESWT with the radial shock wave device, Swiss DolorClast (EMS Electro Medical Systems, Nyon, Switzerland) using the “radial” (blue) handpiece. Each patient received 3 sessions of rESWT, 1 week apart, 2,000 impulses per session, to the most painful area determined by palpation. The air pressure of the device was adjusted to the maximum discomfort the individual patient could tolerate, resulting in individual air pressures of between 2.5 and 4.0 bar and, thus, positive EFD of between 0.10 and 0.16 mJ/mm2. Impulses were applied at a frequency of 8 Hz. Local anaesthesia or analgesic drugs were not applied during the rESWT sessions. The decision to omit the use of local anaesthesia was based on 2 RCTs that demonstrated that application of local anaesthesia to the area of treatment adversely affects the outcome of ESWT (27, 28).
The control group received placebo treatment in an identical manner to the rESWT treatments described above, except for the fact that no EFD was applied. This was achieved by using a placebo handpiece that looked, felt and sounded identical to the “radial” (blue) handpiece of the Swiss DolorClast device, but did not emit radial shock waves (a similar placebo handpiece was used in (29)).
Both groups received a post-application home treatment programme for 3 consecutive days after each treatment session, consisting of surface heat on the skin areas exposed to rESWT or sham-rESWT for 20 min. If necessary, paracetamol (500 mg every 6 h), or a similar medicine in case of allergy, was prescribed for 3 consecutive days after each treatment session.
Treatments were performed at the Institute of Physical and Rehabilitation Medicine, University of São Paulo School of Medicine. Thus, at first glance the intervention was undertaken in a specialist centre that was not representative of the hospitals and clinics that most of the source population would attend. However, all treatments were performed on an outpatient basis and, thus, representative of that in use in the source population.
Clinical assessments included assessment of pain on movement and physical function. The primary outcome measure was pain on movement, measured using a 10-cm visual analogue scale (VAS) (30), with 0 indicating no pain and 10 maximum pain. Secondary outcomes were pain, stiffness and limitations in physical function on the WOMAC Index (31) on both the treated and the untreated side. Evaluation was performed at baseline, and 1 week (W1) and 3 months (M3) after the final treatment session.
The WOMAC Index assesses the symptoms of OA and is a validated, disease-specific, self-reporting questionnaire referring to the 48 h before assessment (31). The index consists of 5 questions for severity of knee pain, 2 for stiffness, and 17 for limitations in physical function. In the present study a modified WOMAC score was calculated, ranging from 0 (best) to 4 (worst) for each criterion (i.e. severity of knee pain, stiffness, and limitations in physical function).
A further evaluation criterion was the level of tolerance to pressure (32, 33) in the following muscles: vastus medialis, vastus lateralis, rectus femoris, gracilis, adductor longus, tibialis anterior, peroneus longus, quadratus lumborum, iliopsoas, and popliteus; pes anserinus and the patellar tendon, the medial joint line, supraspinous ligaments from L1 to S1 and the territory of the dermatomes of L1 to S2. These measurements were performed using a Fischer algometer (Pain Treatment, Great Neck, NY, USA).
Treatment success was defined as individual improvement in the primary outcome measure (VAS score for pain on movement) by >50% compared with baseline.
Complications, adverse effects and complaints during treatment were documented.
Both patients and the study investigators were blinded for the entire duration of the study. Specifically, the patients were not aware whether they received rESWT or placebo treatment, and the study investigators did not have access to the patients’ treatment records, including patient allocation or the allocation sequence, until all patients had completed the 3-month follow-up examination.
As in case of all studies on ESWT listed in the open-access Physiotherapy Evidence Database (PEDro) (12), the therapists who applied the treatments were not blinded. To prevent any bias, they interacted with the study participants strictly in a standardized way irrespective of treatment allocation, preventing any behaviour that could have indicated to the patients whether they received rESWT or placebo treatment. This was further supported by the fact that the look, handling and sound of the rESWT device were identical in both rESWT and placebo treatments, and all rESWT or placebo treatment sessions took approximately 10 min. Furthermore, only patients who had not received ESWT treatments previously were enrolled in the present study, and the names of other patients in the study were not disclosed. Thus, patients could not determine whether they were in the rESWT or the placebo group based on slight pain and discomfort experienced during treatment (which is inherent to rESWT; c.f., e.g. (11)).
The patient flow in the present study according to CONSORT (23) is shown in Fig. 2. Of the 237 patients assessed for eligibility, 105 were randomly allocated to rESWT (n = 52) or placebo treatment (n = 53), respectively. All patients received treatment as allocated. Six out of the 52 patients in the rESWT group and 6 out of the 53 patients in the placebo group were lost to follow up, resulting in full analysis of, respectively, 46/52 (88.5%; rESWT) and 47/53 (88.7%; placebo) of the patients who were randomized.
Fig. 2. Study participants according to the Consolidated Standards of Reporting Trials (CONSORT) Statement (23).
Based on anecdotal evidence from colleagues and our own preliminary data we expected treatment success (i.e. individual reduction of the VAS score by >50% compared with baseline) in 65% of the patients to be treated with rESWT, and in 30% of the patients to be treated with placebo. Considering a 2-sided significance level of 95%, power of 0.9 and equal samples, the power analysis retrieved a minimum number of, respectively, 43 (according to (34)) or 41(according to (35)) per group to be enrolled in the present study. Power analysis was performed with the online tool, Open Source Epidemiologic Statistics for Public Health (36).
Statistical analysis was performed on an intention-to-treat basis using the last observation carried forward approach (37). Mean and standard error of the mean (SEM) were calculated for all investigated variables.
Differences at baseline between the patients treated with rESWT and those treated with placebo were tested with Student’s unpaired t-test in case of the mean age of the patients, Mann–Whitney test in case of the mean duration of pain before treatment, VAS score, and WOMAC scores for pain, rigidity and limitations in physical function, and Fisher’s exact test in case of the affected side.
Treatment-related differences in mean VAS scores and mean levels of tolerance to pressure over the supraspinous ligaments between the patients treated with rESWT and those treated with placebo were tested with repeated measures analysis of variance (ANOVA), with the different times (BL, W1, M3) as within-subject factor, and the treatment (rEWST, placebo) as between-subject factor.
Treatment-related differences in mean WOMAC scores for pain, rigidity and limitations in physical function, as well as mean levels of tolerance to pressure over muscles, tendons and skin between the patients treated with rESWT and those treated with placebo were tested with 2-way repeated measures ANOVA, with the different times (BL, W1, M3) and the side (treated, untreated) as within-subject factors, and the treatment (rEWST, placebo) as between-subject factor.
Treatment success (i.e. number of patients with individual improvement in the VAS score by more than 50% at W1 and M3) was tested with Fisher’s exact test.
In all analyses an effect was considered statistically significant if its associated p-value was smaller than 0.05. Calculations were performed using SPSS (Version 23 for Windows; IBM, Armonk, NY, USA).
With the numbers available, the patients in the intention-to-treat population treated with rESWT were not significantly different statistically from the patients treated with placebo with respect to the sex distribution, mean age, affected side, duration of pain before treatment, mean overall VAS score, and mean WOMAC scores for pain, stiffness and limitations in physical function at both the treated and the untreated sides.
rESWT reduced the mean VAS score by 29.7% (or 2.2 absolute score points) from baseline to 1 week after the final treatment session (W1), and by 21.2% (or 1.6 absolute score points) from baseline to 3 months after the final treatment session (M3) (Fig. 3A). However, similar changes in mean VAS score were also found after placebo treatment (W1: reduction by 25.0% or 1.9 absolute score points; M3: reduction by 22.4% or 1.7 absolute score points) (Fig. 3A). No statistically significant difference was found between rESWT and placebo treatment (p-values are summarized in Table III).
Fig. 3. Tukey box-plots of: (A) visual analogue scale (VAS) scores; (B, C) Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) scores for pain; (D, E) WOMAC scores for rigidity; (F, G) WOMAC scores for limitations in physical function, obtained with intention-to-treat analysis at baseline (BL), 1 week after the final treatment session (W1) and 3 months after the final treatment session (M3) of the patients treated with radial extracorporeal shock wave therapy (rESWT) (grey boxes) or placebo (open boxes). (B, D and F) WOMAC scores obtained on the treated side; (C, E and G) WOMAC scores obtained on the untreated (contralateral) side.
Table III. Statistical analysis of the visual analogue scale (VAS) score, the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) scores for pain, rigidity and limitations in physical function, and the level of tolerance to pressure over muscles, tendons, ligaments and skin using a Fischer algometer
Both rESWT and placebo treatment resulted in similar relative numbers of patients with treatment success (defined as individual reduction in VAS score by >50% compared with baseline) (W1: 25.0% (13/52) after rESWT and 20.8% (11/53) after placebo treatment; M3: 23.1% (12/52) after rESWT and 20.8% (11/53) after placebo treatment). No statistically significant difference was found between rESWT and placebo treatment (W1: p = 0.648; M3: p = 0.817).
rESWT reduced the mean WOMAC score for pain on the treated side by 36.5% at W1, and by 32.2% at M3 (Fig. 3B). The corresponding numbers for placebo treatment were 19.2% at W1 and 11.8% at M3 (Fig. 3B). This difference between rESWT and placebo treatment was statistically significant (p-values are summarized in Table III). The mean WOMAC scores for stiffness and limitations in physical function were not statistically significantly different between rESWT and placebo treatment (Fig. 3D, F).
The mean WOMAC scores for pain, stiffness, and limitations in physical function on the untreated side were statistically significantly lower than the corresponding scores on the treated side (p-values are summarized in Table III) and showed only small changes during follow-up after rESWT or placebo treatment (Fig. 3C, E, G).
Slight, but statistically significant, differences between the patients treated with rESWT and those treated with placebo were only found in the iliopsoas muscle (p-values are summarized in Table III). The other measurements showed no statistically significant differences between rESWT and placebo treatment. Overall, differences between the patients treated with rESWT and those treated with placebo were small.
No complications were observed.
The findings of the present study can be summarized as follows: rESWT, as applied here (3 sessions, each 1 week apart, 2000 impulses each, positive EFD 0.10–0.16 mJ/mm2) was not superior to placebo treatment (except for an improved mean WOMAC score for pain in the treated side and some of the pressure measurements obtained with a Fischer algometer). Thus, rESWT, as performed in the present study, was not superior to placebo.
In order to identify the factors that may have caused the negative outcome of the present study we compared our rESWT protocol with other ESWT protocols that were applied successfully in RCTs on ESWT for alleviating pain in patients with knee OA (21, 22) (Table IV). Initially, it appears that differences in the mean duration of pain before ESWT (92.4 months in our study; between 3 and 19.3 months in the other studies) could have caused the difference in outcome. However, the duration of pain before rESWT varied between 3 and 480 months in our study and had no impact on the individual change in the VAS score after rESWT (data not shown). In fact, the data summarized in Table IV do not allow us to determine why the present study failed to demonstrate any superiority of rESWT over placebo, when other studies using fESWT (21) or rEWST (22) were successful in alleviating pain in patients with knee OA. However, the results of the study by Kim et al. (21) should be interpreted cautiously, as the lower of the 2 total energy flux densities (EFDs) applied in this study (i.e. 120 mJ/mm2) was approximately 10 times less than the mean total EFD applied in 66 RCTs on fESWT for tendon and other pathologies of the musculoskeletal system with positive outcome (12), but was approximately 33 times less than the total positive EFD used by Zhao et al. (22) for treating knee OA with rESWT. Nevertheless, Kim et al.’s results (21) were supposedly better than the results obtained by Zhao et al. (22), let alone the results of the present study. On the other hand, several studies demonstrated that the effects of ESWT on the musculoskeletal system are dose-dependent, i.e. “more is better” (c.f., e.g. 38–40), and fESWT is not better than rESWT (or vice versa) when treating pathologies of the musculoskeletal system (12) except of deep non-unions. It is therefore highly desirable to repeat Kim et al.’s study on an independent sample of patients, including a placebo group (which was not done in the study by Kim et al. (21), but was in the study by Zhao et al. (22) and the present study). When comparing only Zhao et al.’s study (22) with the present one, the best explanation for the different outcome is that Zhao et al. (22) used radial extracorporeal shock waves with a higher positive EFD and a more than 4 times higher total positive EFD than the present study.
Table IV. Details of published studies on extracorporeal shock wave therapy for knee osteoarthritis
It should be noted that Chen et al. (41) used fESWT for treating patients with knee OA and a sesamoid bone in the popliteus muscle (popliteal cyamella). However, the authors focused the extracorporeal shock waves on the sesamoid bones with the aim to treat them similarly to the treatment of calcific tendinopathy. Thus, this study by Chen et al. (41) cannot be compared with the studies summarized in Table IV (including the present one).
The molecular and cellular mechanisms of ESWT mediating pain relief in knee OA are virtually unknown. Ochiai et al. (42) showed in a rat model of knee OA that, compared with control animals, the number of neurones immunopositive (ip) for calcitonin gene-related peptide (CGRP) was increased in those dorsal root ganglia (DRG) innervating the knee, and application of extracorporeal shock waves reduced the number of these CGRP-ip neurones to control levels. This is in line with the results of Hausdorf et al. (43), who found that application of extracorporeal shock waves to the distal femur of rabbits diminished the number of substance P-ip neurones in dorsal root ganglia L5. Substance P and CGRP are important neuropeptides in nociceptive processes (reviewed in (44)) and contribute to the nociceptive input from joints in different types of spinal cord neurones. Depletion of substance P from the small, unmyelinated C-fibres is considered a major player in mediating pain relief by ESWT (45). Other potential mechanisms mediating pain relief in knee OA by ESWT that have been proposed in the literature based on animal experiments are improved subchondral bone remodelling and decreased cartilage degradation (18, 19), as well as reduced progression of knee OA due to decreased levels of nitric oxide and reduced chondrocyte apoptosis (20). However, it appears unlikely that these mechanisms play a major role in human knee OA with disabling pain for several years. More relevant are data from Frisbie et al. (46), who experimentally induced OA in the middle carpal joints of horses without lameness, exposed them to ESWT 2 weeks after induction of OA, performed clinical assessments of the degree of lameness every 2 weeks and weekly synovial fluid analyses, and euthanized the horses 70 days after induction of OA for histological examinations of cartilage and synovial membrane specimens at necropsy. These authors found that the degree of lameness in horses treated with ESWT improved significantly, compared with the degree of lameness in placebo-treated horses. However, no disease-modifying effects were evident in results for synovial fluid, synovial membranes, or cartilage from the horses treated with ESWT (46). In summary, further studies are required to identify the molecular and cellular mechanisms of ESWT mediating pain relief in knee OA.
The present study is an audit of prospectively collected data, and therefore has inherent limitations. First, there was no blinding of the physician who administered the therapy; however, this was also the case in all studies on ESWT listed in the PEDro database (12). Secondly, the final follow-up examination was performed at 3 months, i.e. relatively soon after the treatment; however, the negative outcome 3 months after the final treatment would not have justified an additional follow-up examination at a later time-point. Thirdly, the small number of patients could potentially confound the clinical results; however, to our knowledge the present study on ESWT for knee OA was the one with the largest number of patients performed so far. Fourthly, we did not perform magnetic resonance imaging (MRI) and did not rule out bone marrow oedema and synovitis of the knee, because bone marrow oedema of the knee occurs secondary to a myriad of causes (47). Furthermore, diagnosis of bone marrow oedema or synovitis of the knee would not have had any impact on inclusion or exclusion of patients into the present study. In this regard it is important to note that it is unknown whether rESWT may have any impact on bone marrow oedema. For focused shock waves applied at a substantially higher energy flux density than used in the present study, one study (48) showed that, in patients with chronic plantar fasciopathy, the presence of calcaneal bone marrow oedema on pre-therapeutic MRI is a good predictive variable for a satisfactory clinical outcome of ESWT. However, it is important to note that there are substantial differences in the pathogenesis of plantar fasciopathy and knee OA and, thus, there may also be different mechanisms of action of ESWT in these different conditions. Furthermore, the clinical symptoms, physical findings and radiological examinations used to define knee OA in the present study are generally accepted and considered appropriate for this condition (21, 22, 24).
In conclusion, rESWT, as applied in the present study, is not efficient for treating patients with disabling pain due to severe primary knee OA. Data from Zhao et al. (22) show that in order to achieve treatment success this indication requires substantially higher total positive EFDs than were applied in the present study. Further RCTs are warranted to determine whether this can be achieved with more impulses (e.g. 5 treatment sessions with 5,000 impulses per session and a positive EFD of 0.16 mJ/mm2) or whether radial shock waves with positive EFD higher than 0.16 mJ/mm2 must be applied (as was done in (22)). The “Power+” (red) handpiece of the Swiss DolorClast can deliver radial shock waves with positive EFD of up to 0.4 mJ/mm2. In any case, such studies should have both subjective and objective endpoints.
This study was supported by a grant from the Institute of Physical and Rehabilitation Medicine at the University of São Paulo School of Medicine.
Conflicts of interest. C.S. is a paid consultant for Electro Medical Systems (Nyon, Switzerland), the manufacturer of the Swiss DolorClast used in the present study. However, Electro Medical Systems had no role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript. The other authors report no conflicts of interest.


 Click to show fullsize
Click to show fullsize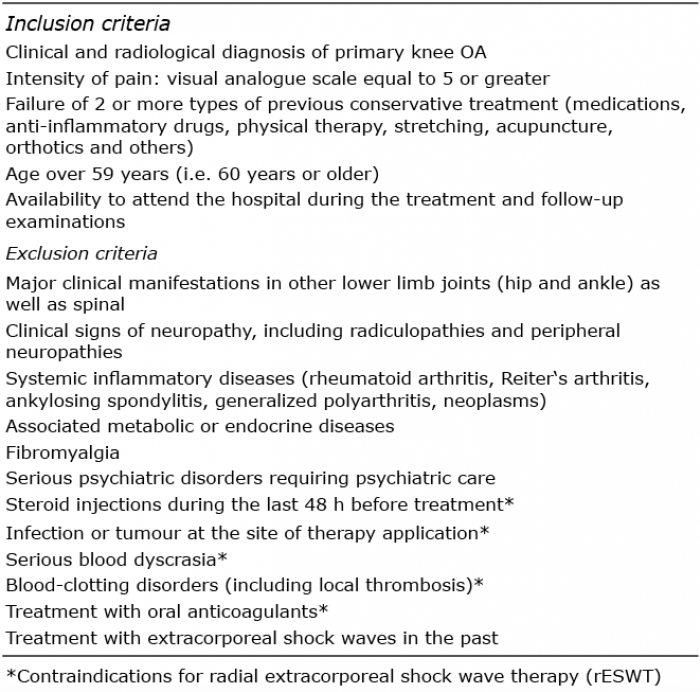 Click to show fullsize
Click to show fullsize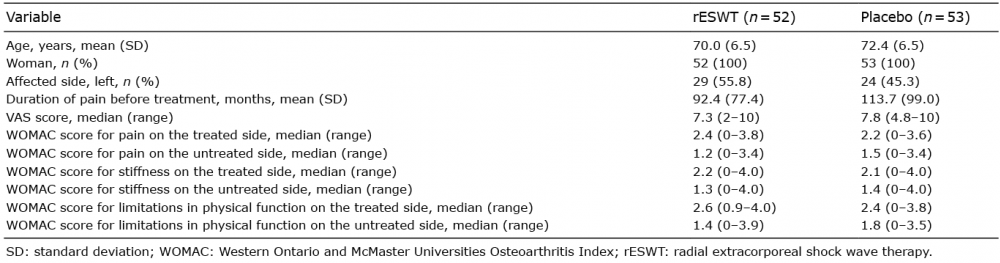 Click to show fullsize
Click to show fullsize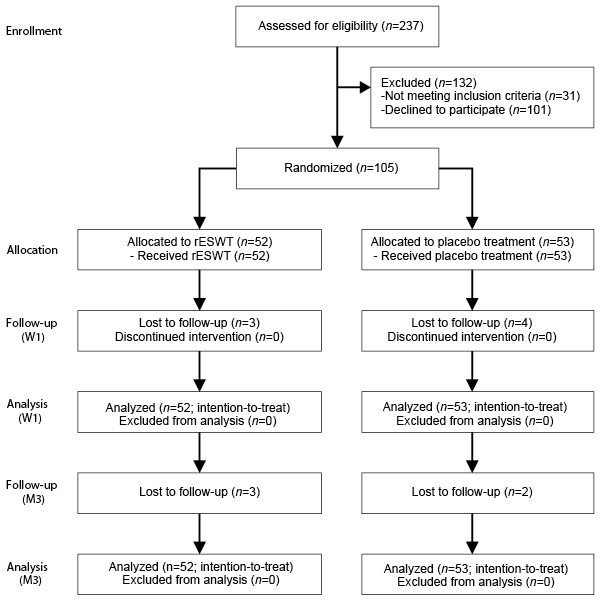 Click to show fullsize
Click to show fullsize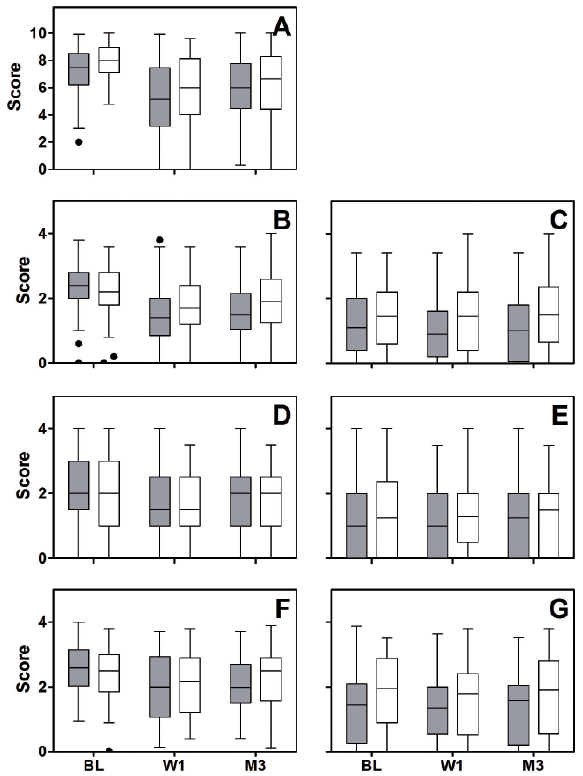 Click to show fullsize
Click to show fullsize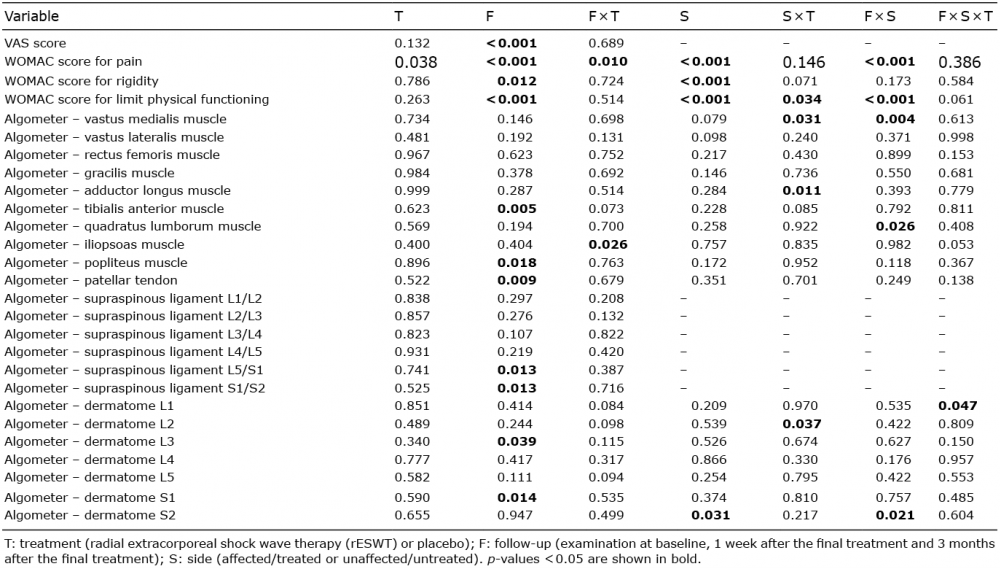 Click to show fullsize
Click to show fullsize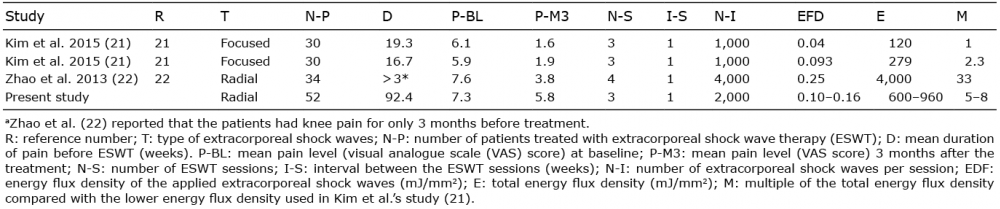 Click to show fullsize
Click to show fullsize