
From the 1Comprehensive Cancer Center North, 2OB/GYN, University Hospital for Women, and 3Institute of Sport Science, University of Kiel, Kiel, Germany
Objective: To investigate the safety and efficacy of arm crank ergometry in breast cancer patients after axillary lymph node dissection, with regard to changes in bioelectrical impedance analysis, arm circumference, muscular strength, quality of life and fatigue.
Design: Randomized controlled clinical intervention trial.
Subjects: Forty-nine patients with breast cancer after axillary lymph node dissection.
Methods: Arm crank ergometer training twice-weekly was compared with usual care over 12 weeks.
Results: The arm crank ergometer group improved significantly in terms of lean body mass and skeletal muscle mass, and showed a significant decrease in body fat. In the arm crank ergometer group, as well as the usual care group, a significant increase in armpit circumference was detected during the training period. The magnitude of the gain was higher in the usual care group. For all other measured regions of the arm a significant decrease in circumference was seen in both groups. Muscular strength of the upper extremity increased significantly in both groups, with a greater improvement in the arm crank ergometer group. In both groups a non-significant trend towards improvement in quality of life was observed. The arm crank ergometer group showed significant improvements in physical functioning, general fatigue and physical fatigue.
Conclusion: These results confirm the feasibility of arm crank ergometer training after axillary lymph node dissection and highlight improvements in strength, quality of life and reduced arm symptoms with this training.
Key words: breast cancer-related lymphoedema; arm crank ergometer; physical activity.
Accepted Sep 14, 2016; Epub ahead of print Dec 8, 2016
J Rehabil Med 2017; 47: 78–83
Correspondence address: Thorsten Schmidt, Breast Unit, Comprehensive Cancer Center North, University of Kiel, Arnold-Heller-Str. 3, DE-24105 Kiel, Germany. E-mail: thorsten.schmidt@uksh.de
Breast cancer is the most prevalent cancer in women, with a high survival rate but significant long-term morbidity after treatment. Rehabilitation of post-treatment effects of breast cancer treatment is needed to improve functioning and quality of life (QoL). In addition to surgery of the breast, 61% of patients undergo axillary sentinel lymph node biopsy. Thirty-three percent of patients with breast cancer require complete axillary lymph node dissection (ALND) (1, 2). The risk of developing a lymphoedema, based on the clinical definition, is 5–20% (1, 3, 4).
Rehabilitation of breast cancer patients focuses on side-effects after axillary surgery, such as pain and physical impairments. Meanwhile, there is evidence that physical activity is an important factor in improving overall survival and time to progression (5, 6). Inactivity, related or not related to cancer treatment, can weaken the skeleton, cause muscle loss and lead to fat gain (7–10). These changes in body composition place breast cancer survivors at a higher risk of obesity-related diseases, breast cancer recurrence, frailty and fractures (11). Previous findings suggest that physical activity during and after breast cancer treatment can not only reduce side-effects (8, 12–15), but also improve clinical outcome (9, 10, 12, 14–16).
In the past, intense physical activity of the upper extremity has not been recommended after ALND and/or radiation to the axilla. As there is a lack of recommendations or guidelines on physical activity for patients with lymphoedema of the arm after breast cancer therapy, women with this postoperative complication are uncertain about exercising. Recent studies have reported that progressive weight-lifting did not have any preventative effect on development of breast/arm swelling (or lymphoedema). Nonetheless, there are only a small number of randomized controlled trials on this topic (16–25).
This clinical interventional trial investigates the feasibility of arm crank ergometer (ACE) training after ALND for primary breast cancer. Safety, efficacy and the influence on prevention or improvement of existing lymphoedema of the arm are the main study endpoints.
In this prospective, controlled, randomized intervention trial 12-week supervised ACE-training was compared with usual care (UC) in breast cancer patients after ALND. Patients were recruited at a major, academic, breast oncology unit in Germany. Participating women had to meet the following eligibility criteria: primary breast cancer; within 3 years after axillary lymph node dissection; age range 18–75 years. Exclusion criteria were: intended radiotherapy or chemotherapy during the study period; acute infectious disease; severe cardiac disease (New York Heart Association functional class III; myocardial infarction < 3 months); severe pulmonary or renal insufficiency (glomerular filtration rate < 30%); serious neurological disorders; fewer than 10,000 platelets/ml; and haemoglobin < 8g/dl.
The study was approved by the local ethics committee (registration number: AZ A 104/14). All participants were included in the study after providing written informed consent, as required by the Declaration of Helsinki (1975).
After baseline assessments the patients were assigned randomly (1:1) to supervised ACE-training or UC using a computer-generated programme. The allocation sequence was executed by the clinical research unit and concealed from the project team. To prevent a possible bias, research physicians did not have access to the randomization files.
The analysis included data for patients who attended at least 70% of the scheduled training sessions. Performance was assessed at baseline (T1) and 12 weeks after initiation of physical intervention (T2). Primary endpoints of this trial were change in body composition of the upper extremity, measured by bioelectrical impedance analysis (BIA), arm volume (arm circumference), muscular strength (NM), QoL (European Organization for Research and Treatment of Cancer (EORTC) QLQ C30+BR23) and fatigue (Multidimensional Fatigue Inventory; MFI 20) before training and after 12 weeks of training.
For the within-group changes, a dependent t-test (body composition of the upper extremity and the trunk, arm volume (arm circumference) and muscular strength) and the Wilcoxon-test (EORTC and fatigue questionnaire) were used. Comparisons of the ACE group with the UC group for changes from baseline to 12-week assessment (T2–T1) were performed using independent t-test. Statistical significance for the t-test at T1 and T2 was set at a probability level of p < 0.05. The effects are expressed with mean and standard deviations. Analysis was performed using the SPSS system for windows (Version: PASW 21).
Body mass index (BMI) was calculated and body composition was determined by anthropometry and bioelectrical impedance analysis (BIA) (InBody, Modell 520, Germany). The body composition of the upper extremity and the trunk were measured under constant conditions (e.g. time of day and good hydration). BIA determined values (in %) for lean body mass (LBM), skeletal muscle mass, and body fat. The participant was positioned in an orthostatic position on a platform with lower electrodes for the feet and upper electrodes for the hands, enabling evaluation of the impedance of each body segment.
Arm circumference was measured in all randomized patients at defined anatomical regions (armpit, 15 cm above the lateral epicondyles of the elbow, elbow, and wrist). This measurement was performed on the arm (after ALND) and, for comparison, on the contralateral arm (non-ALND arm). Measurements were performed at time-points T1 and T2 (before and after study-related training). The impact of the training type (ACE vs UC) on changes in arm circumferences was statistically analysed. Lymphoedema was defined as a difference of the arm circumference > 5% between the time of measurement.
The muscular strength of the upper extremities (latissimus dorsi muscle and pectoralis muscle) was assessed by measuring their isometric muscular capacity with M3 Diagnos (Schnell, Germany) combined with “Diagnos Professional 2000” software. To test the maximum strength of the upper extremities the patients were encouraged to stretch their arms against the fixed bar for approximately 5 s (pectoralis muscle), followed by pulling the fixed bar for approximately 5 s (latissimus dorsi muscle). Every test was repeated twice, with appropriate breaks in between.
The EORTC has developed several validated questionnaires to assess the QoL of patients with cancer in a multidimensional approach. The questionnaire used was EORTC QLQ C30, version 3 BR23, which was especially developed for patients with breast cancer. The results section of the questionnaire focuses on QoL and fatigue (26, 27). Fatigue symptoms were assessed with the Multidimensional Fatigue Inventory with 20 questions (MFI-20). The MFI-20 is an internationally frequently used questionnaire (28, 29).
The ACE training included strength and endurance training with an arm crank ergometer (MOTOmed®, Reck, Betzenweiler) for 60 min twice weekly for 12 weeks. Every training session was supervised and documented by experienced exercise therapists. Before each training session, the intensity levels were checked according to the exercise guidelines for cancer survivors of the American College of Sports Medicine (30). The training principle consists of 3 possible training components: 1.step, a passive completely motorized training; 2.step, a motor-supported self-training; and 3.step, a training by patient-generated power. Depending on the patient-reported performance status, patients participated in the different training modalities. In case of a reduced performance status they enhanced their performance gradually and proceeded stepwise from training steps 1 to 3. When they reported a good performance status, they entered training steps 2 or 3.
The Borg scale was used as a subjective reference point for self-reported performance status during training. Patients were encouraged to be active at Borg levels 11–14 (31, 32). The 45-min training included a 10-min warm-up, 25–30 min of exercise (in training steps 1–3) and a 5-min cool-down period. When a lymphoedema occurred the training intensity was reduced and carried out either motorized or motor-supported. A lymphoedema was defined as a 5% increase in the volume of the affected limb. Participants in the usual care group were informed about the feasibility of physical activity and the impact of physical activity for breast cancer-related lymphoedema, but did not receive supervised training.
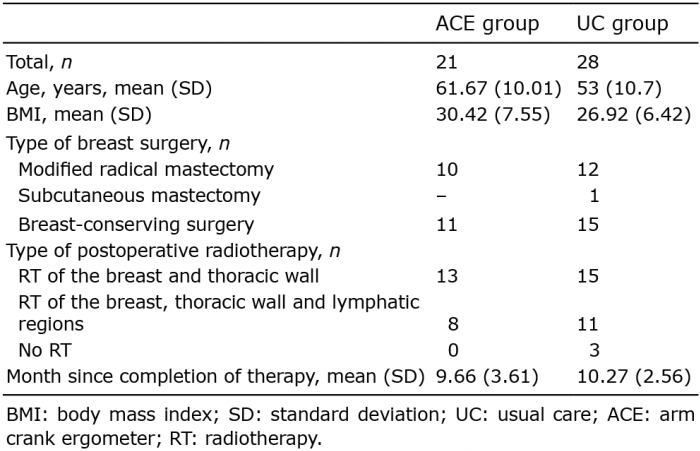
A total of 120 patients were identified retrospectively and contacted between May and December 2014. Sixty-two patients fulfilled the inclusion criteria and were enrolled and randomized into the ACE group or UC group. Fifty-eight of the identified patients were unable to participate; of these, 46 declined to participate due to the distance to the study centre, 8 had died, and 4 were not interested. Due to timing issues, family problems, or withdrawal of consent, 13 out of 62 enrolled and randomized patients dropped out: 6 withdrew from the ACE group and 7 from the UC group. Data for 49 patients were fully evaluable (21 patients in the ACE group, 28 in the UC group). An overview of the patient cohort is shown in Table I and Fig. 1.
Table I. Patient characteristics
Fig. 1. Study flowchart. ACE: arm crank ergometer; UC: usual care.
During the course of the study a significant increase in lean body mass (LBM) of the patients in the ACE group was detected (ALND-arm, p = 0.017; non-ALND-arm, p = 0.004). Furthermore, a significant increase in skeletal muscle mass (ACE group, p = 0.049) and decrease in body fat in the ACE group (ACE group, p = 0.009) could be observed. In the UC group there was a trend towards improvement, but no significant change, in LBM (ALND-arm, p = 0.679; non-ALND-arm, p = 0.354), skeletal muscle mass (UC group, p = 0.385) or body fat (UC group, p = 0.393) (Table II).
Table II. Body composition of the upper extremity of the intervention group and the usual care group at baseline (T1) vs 12 weeks after the initiation of intervention (T2)
A decrease in circumference of the ALND-arm could be detected at the measuring point’s wrist joint, 15 cm above the lateral epicondylus of the elbow and the elbow in patients in both study groups. Also, a significant increase in the circumference of the armpit of the ALND-arm could be seen in both groups, whereby the increase was stronger in the UC group (ACE group: +4.29%, UC group: 10.66%) (Table III). In comparison with the ALND-arm, the non-ALND-arm showed no major difference in both groups.
Table III. Circumference of the upper extremity of the intervention group and the usual care group at baseline (T1) vs 12 weeks after the initiation of intervention (T2)
Muscular strength improved in both groups from T1 to T2. Compared with the control group, the ACE group had a greater improvement in muscular strength of the upper extremity (non-significant) (Table IV).
Table IV. Muscular strength of the upper extremity of the intervention group and the usual care group at baseline (T1) vs 12 weeks after initiation of the intervention (T2)
In both groups a non-significant trend towards improvement in QoL was observed (ACE group, p = 0.101; UC group, p = 0.202). The ACE group significantly improved in terms of physical functioning (ACE group, p = 0.038; UC group, p = 0.428); general fatigue (ACE group, p = 0.032; UC group, p = 0.483) and physical fatigue (ACE group, p = 0.002; UC group, p = 0.42). In the UC group only minor non-significant changes were detected. Other scales of the EORTC and the BR23 questionnaire module showed no changes in the ACE group and UC group (Table V).
Table V. Psychology parameters, quality of life (EORTC QLQ C30) fatigue (MFI20) and total activity score (IPAG) of the intervention group and the usual care group
A comparison of the mean differences between the ACE group and the UC group showed no significant differences between the 2 groups. In both groups the range of the circumference of the upper extremity decreased at the measuring points wrist joint, 15 cm above the lateral epicondylus of the elbow and the elbow. In both groups an increased mean difference in the circumference of the armpit of the ALND-arm was seen (Table VI)
Table VI. Mean difference (T2–T1) in the circumference of the upper extremity of the intervention group and the usual care group
A similar picture emerged for the data regarding body composition and muscular strength, whereby, in comparison with the UC group, the ACE group showed a major improvement (Tables VII and VIII).
Table VII. Mean difference in body composition of the upper extremity of the intervention group and the usual care group
Table VIII. Mean difference (T2–T1) in the muscular strength of the upper extremity of the intervention group and the usual care group
Until recently it was not recommended that patients undertake physical activity of the upper extremity after axillary lymph node dissection and/or radiation to the axilla. There was unsubstantiated concern that physical activity could initiate or lead to deterioration of a lymphoedema. A small number of publications showed that physical activity and upper-body exercise does not have an influence on the development or worsening of lymphoedema (20). The majority of publications investigated the impact of resistance training, whereas upper-body endurance training was under-represented. The primary objective of our study was to determine the impact of arm crank ergometer training as a strength and endurance training on the development or worsening of lymphoedema in breast cancer patients who have undergone axillary lymph node dissection. Based on the inclusion criteria comparison with the few published randomized controlled trials is difficult. Sagen et al. included women after an axillary dissection (18), Schmitz et al. (23) included women who had had a sentinel node biopsy or an axillary dissection (19). Blommquist et al. did not report any details about the type of surgery. Furthermore, different definitions for lymphoedema were used. Schmitz et al. defined a lymphoedema as an increase in the volume of the affected limb of 5% or more, accompanied by an increase of 5% or more in the difference in the volume or circumference of the affected and unaffected limbs (19). In the study by Bloomquist et al. a lymphoedema is defined as a difference of ≤ 2 cm at 2 or more measures (23).
Similar to the results of previous studies, strength and endurance training with an arm crank ergometer did not have a detrimental effect on breast cancer-associated lymphoedema compared with usual care. A decrease in arm circumference was seen in both groups and potential lymphoedema exacerbations were found in the UC group. Furthermore, muscle strength improved in both groups, whereas the improvement in the ACE group was more pronounced. A possible explanation for the decrease in arm circumference and the improvement in muscle strength in the UC group is that participants in the UC group were more confident to exercise their upper limb due to education about the impact of physical activity on breast cancer-related lymphoedema. Furthermore, physical activity is known to improve the flow of lymphatic fluid and protein resorption (20).
The improvement in QoL and physical functioning detected in the ACE group is confirmed by other study results. In a population-based cohort study Chen et al. evaluated the effect of regular exercise on QoL during the first 3 years after breast cancer diagnosis. It was observed that women with a higher exercise score were more likely to have higher scores for total QoL and specific subscales, compared with women taking non-regular exercise after breast cancer diagnosis (33). Gautam et al. confirmed the results in a pre-post intervention study with breast cancer patients who had undergone mastectomy and had completed medical therapy. After an 8-week home-based programme the participants’ QoL had improved (25). The improvement in QoL in the UC group was the same as that in the ACE group. In comparison with the literature the evidence grade is high for physical factors and low for mental health data (QoL, fatigue, anxiety, depression), as published trials differ substantially in design and the study populations and cannot be compared head to head. The current literature in the field of QoL of breast cancer patients after medical treatment confirmed our data (34, 35). The ACE group improved significantly in terms of general fatigue and physical fatigue, whereas non-significant changes could be detected in the UC. In fact, there are limited studies investigating the impact of physical activity on fatigue.
This is one of the first clinical trials to investigate the safety and efficacy of arm crank ergometry for endurance and strength training.
A limitation of this study is that the results are limited by the large amount of parallel statistical testing performed. The probability of occurrence of false-positive results was thereby increased. Furthermore, the small sample size limited the power of the results. It is therefore our intention to verify the results in a follow-up study with increased sample size and subgroup analysis.
In conclusion, the results of the present study, supported by the current literature, show a positive development of strength, endurance, QoL and fatigue and no influence of the onset or worsening of lymphoedema. These positive results suggest that strength and endurance training with an arm crank ergometer should be implemented in the regular aftercare of patients with breast cancer.
The author would like to acknowledge Wiebke Kaczmarek and Katrin Dehn of the Institute of Sport Science, Kiel, Germany for their support in patient care.
This trial was supported by Reck, Betzweiler, Germany with financial support. The Supporter had no role in the study design, data collection and analysis, preparation of the manuscript or decision to publish.
The authors declare no conflicts of interest.


 Click to show fullsize
Click to show fullsize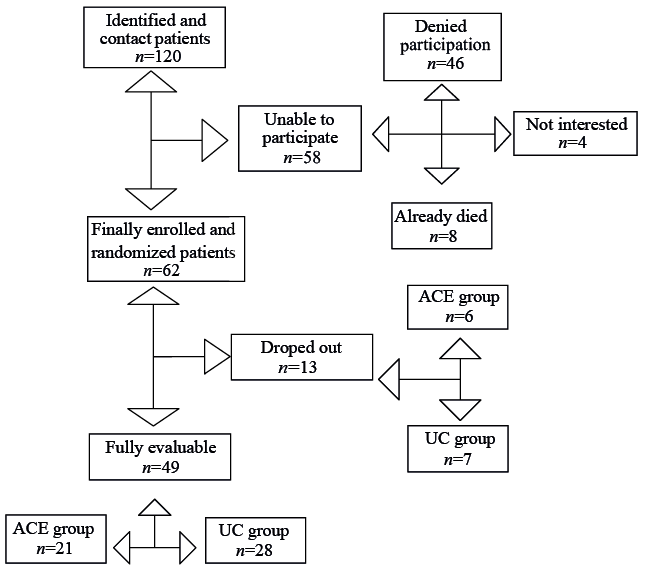 Click to show fullsize
Click to show fullsize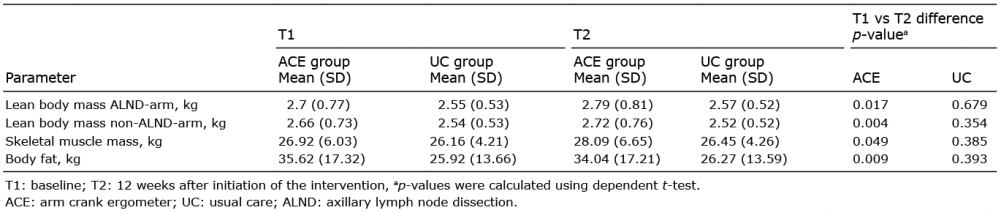 Click to show fullsize
Click to show fullsize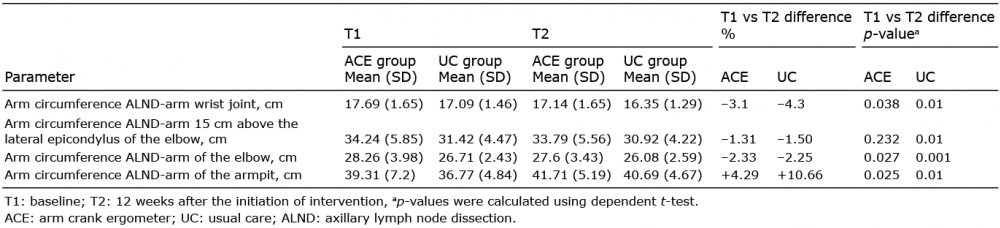 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize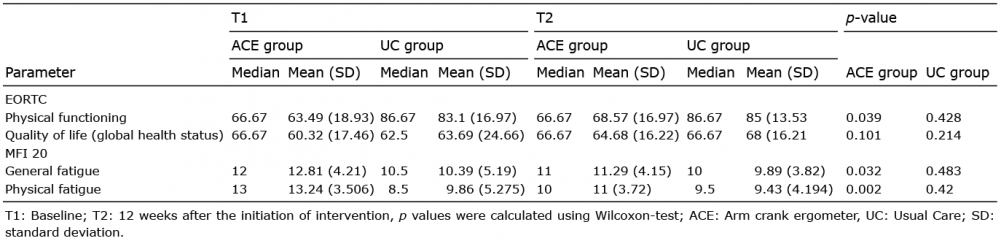 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize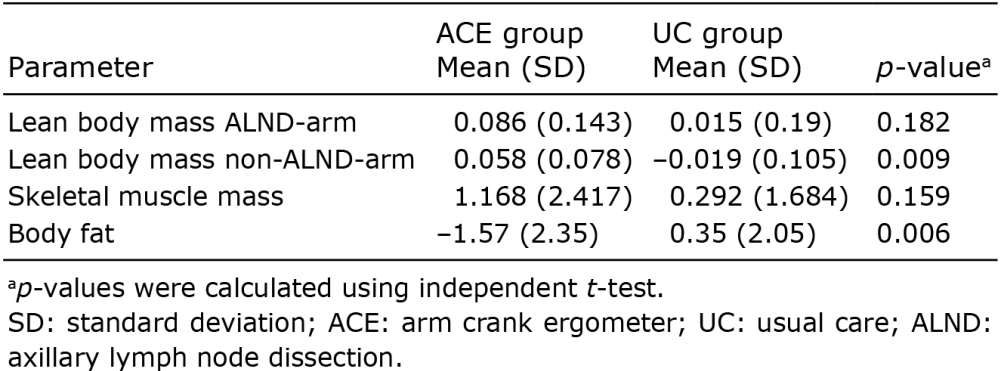 Click to show fullsize
Click to show fullsize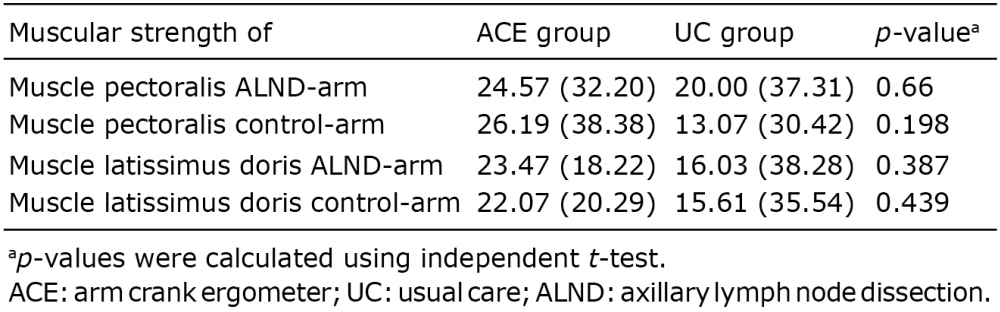 Click to show fullsize
Click to show fullsize