
From the Rehabilitation Medicine, Memorial Rehabilitation Institute, Hollywood, FL, USA
Case report: A 56-year-old man presented with advanced heart failure requiring implantation of a left ventricular assist device and was discharged home. after implantation He returned to the hospital with right posterior putamen stroke and after a comprehensive rehabilitation programme was discharged home with the ability to be independent. The patient later underwent heart transplantation and subsequently required readmission to inpatient rehabilitation. He again completed a comprehensive rehabilitation programme and returned home with the ability to be independent with use of a single-point cane for ambulation.
Conclusion: Patients with advanced heart failure present a challenge to the rehabilitation team, but with a multidisciplinary approach and physiatrist leadership patients can return home and achieve improved quality of life.
Key words: stroke; heart transplantation; rehabilitation; left ventricular assist device.
Accepted Sep 30, 2016: Epub ahead of print Nov 30, 2016
J Rehabil Med 2017; 49: 91–93
Correspondence address: Keith J. Foster, Rehabilitation Medicine, Memorial Rehabilitation Institute, 33021 Hollywood, FL, USA. E-mail: kefoster@mhs.net
Left ventricular assist devices (LVADs) and cardiac transplantations are rapidly becoming standard care for advanced heart failure. With the increase in procedures to improve quality of life for patients with heart disease comes an increasing need for rehabilitation services throughout the continuum of care. Patients with LVAD and transplant present a challenge to rehabilitation professionals as they are at higher risk for multiple complications, including rejection of transplanted organs, increased rate of infections, depression and anxiety, as well as embolic events, and require significant coordination of care and services.
Physical and occupational therapy intervention begins with early mobilization in the acute care setting, including low-level physical activity, self-care, reinforcement of cardiac precautions, implementing energy conservation techniques and graded activities. Early intervention in the acute care setting allows patients to engage in monitored levels of activity to prevent prolonged periods of inactivity. Patients will then transition into inpatient rehabilitation programmes to further implement cardiopulmonary rehabilitation techniques (i.e. diaphragmatic breathing, pursed lip breathing, energy conservation), upgrade their performance activities of daily living (ADL), increase standing/sitting balance, assess durable medical equipment needs, evaluate patient’s homes for barrier-free design, and increase independence in instrumental activities of daily living (IADL) to promote safe discharge home.
The patient is a 56-year-old man with past medical history of class IV stage D chronic systolic and diastolic heart disease with a 10% ejection fraction. He was evaluated by the advanced heart failure team at the Memorial Regional Hospital, Hollywood, FL, USA, and on 15 June 2015 underwent implantation of a HeartMate-II LVAD manufactured by Thoratec. The patient was doing well at home; however, on 28 June 2015 he developed left-sided weakness and was admitted to the hospital with a right posterior putamen infarct. The patient underwent a ten day comprehensive inpatient rehabilitation programme including rehabilitation nursing, physical therapy, occupational therapy, speech therapy and neuropsychology at the Memorial Rehabilitation Institute, Hollywood, FL, USA.
Physical therapists have a vital role in inpatient rehabilitation, with their plan of care focused on strength training, gait management, balance training, lower extremity coordination, and cardiopulmonary endurance training. Occupational therapists assisted the patient achieve improved independence in showering and donning street clothes, cooking, exercise, and coping groups. Therapists in this stage of recovery prepare the patient to go home, by challenging them with higher level tasks such as laundry management, meal preparation, household mobility, and morning ADLs. Subsequently, following inpatient care, cardiac patients are discharged home and may resume outpatient therapies.
The patient was admitted to the Memorial Regional Hospital on 28 June 2015, 2 weeks after LVAD placement with left-sided weakness and emesis, computerized axial tomography (CAT) scan of the brain showed right subarachnoid haemorrhage and right middle cerebral artery territory infarct.
Physical and occupational therapy evaluation was conducted on the acute care unit on 30 June 2015. Initial physical therapy examination findings included decreased sensation to light touch on the left foot, difficulty with dorsi-flexion and closed chain activities, and motor apraxia when ambulating short distances with a rolling walker. Initial occupational therapy findings included difficulty managing buttons and electronics with the left hand, ADL decline, and decreased left upper extremity coordination, sensation, and dysmetria in finger-to-nose testing. The patient was evaluated by physiatry and was admitted to inpatient rehabilitation for a comprehensive rehabilitation programme.
Physical and occupational therapy evaluations conducted on admission to rehabilitation were significant for generalized deconditioning with subsequent limitations in activity tolerance, impaired balance and left lower extremity coordination, left lower extremity weakness, and impaired problem-solving and memory, limiting safety awareness, which limited his functional mobility as well as functional ADL deficits (total assist for lower body dressing and minimal assistance for upper body dressing), decreased balance with toilet transfers, poor safety awareness, and decreased attention to left side, decreased fine motor control and problem-solving skills when managing the LVAD wires, and decreased bilateral hand integration during grooming tasks.
After completion of inpatient rehabilitation programme the patient was able to complete all ADLs at the independent level, with adaptive equipment with demonstrated increased safety awareness and sequencing when managing the LVAD wires and a shower bag. The patient ambulated 50 m using a cane at the modified independent level, completed 21 steps with one rail on the right side at the modified independent level, completed bed to wheelchair transfer, car transfer, and bed mobility at the independent level, with safety considerations secondary to occasional loss of balance with independent recovery and mild cognitive deficits limiting safety awareness.
The patient was discharged home and was doing well in the community when a heart became available for transplantation. He underwent a heart transplant in 9 October 2015. Initial physical therapy evaluation on 18 October 2015 in the intensive care setting showed findings including acute decline in overall function and ability to mobilize self. The patient required moderate to maximum assistance for bed mobility, dependent/poor sitting (leaning to left side) and standing balance (less than 1 min), and required maximum assistance to ambulate 1 m (ataxic, slow cadence, reports fatigue). Initial occupational therapy evaluation showed generalized weakness, functional decline, impaired balance, increased time to follow 1-step commands and generate simple solutions. The patient presented with increased left upper extremity oedema, limiting passive range of motion to the bilateral upper extremities, decreased sensation, and minimal active movement. His right upper extremity had a decreased active range and he was unable to complete the opposition sequence with the right hand due to decreased strength. The treating therapist had determined that the patient required total assistance for ADLs, transfers, and feeding/grooming tasks. The patient was once again evaluated by physiatry and admitted to a comprehensive rehabilitation programme.
The patient was admitted to the Memorial Rehabilitation Institute on 10 December 2015 for an interdisciplinary comprehensive rehabilitation programme. He was noted on evaluation to have increased resting tremors, severe deconditioning, decreased ability to follow multi-step commands, required reinforcement of sternal precautions during functional tasks, and demonstrated decreased grip strength, which was worse on the left than the right side. He required maximum assistance to put on his trousers and minimal assistance to put on a T-shirt, was able to complete functional transfers with minimal assistance using a single-point cane, and demonstrated inability to propel himself in the wheelchair. He demonstrated decreased lower extremity coordination, decreased hip flexion, fair dynamic standing balance, and good sitting balance. The patient improved and on discharge was able to complete bathing and dressing ADLs, grooming tasks and toilet transfers at the modified independent level of assist. The patient required supervision for household mobility, IADLs (meal preparation and laundry tasks) and bath/shower transfers to decrease risk of falling. The patient completed car transfers, bed mobility, and bed to wheelchair transfers at the independent level with extra time for safety. At the time of discharge the patient could ambulate 120 m with a single-point cane at the independent level.
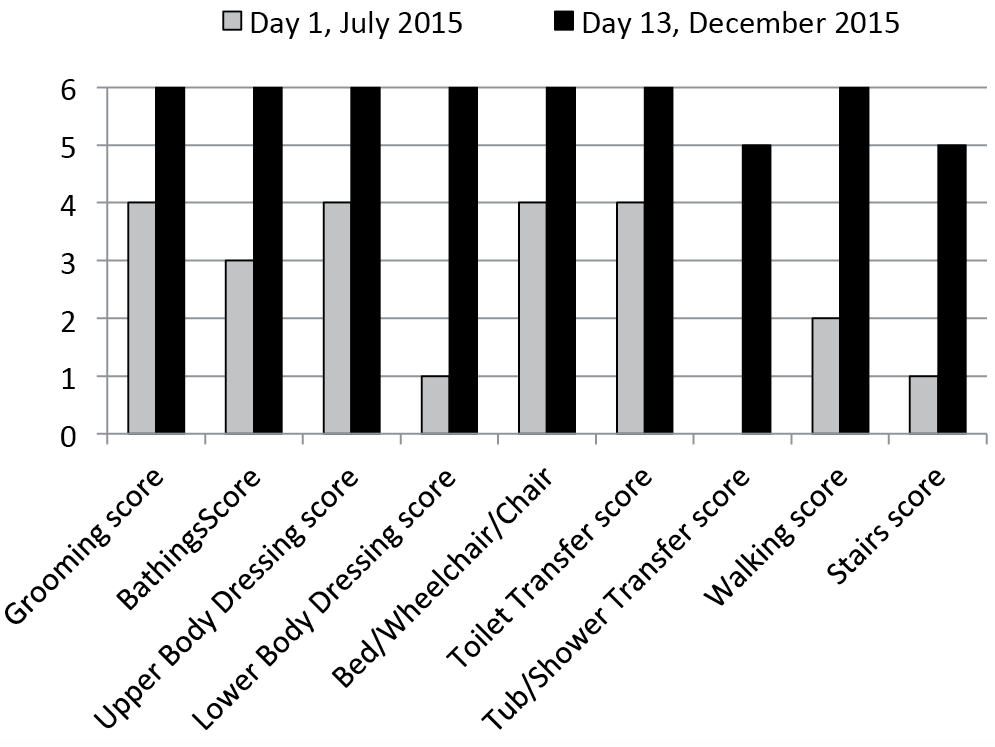
The patient was followed by physical and occupational therapy from the acute care setting to inpatient care in order to promote safe discharge home. The continuum of care for this patient allowed him to maximize his independence, promoting quality of life, so that he could resume his roles, habits, and everyday routines, including returning to driving. During the 2 inpatient rehabilitation admissions the patient made significant gains in functional Independence Measure (FIM) (Fig. 1) and returned home at the independent level with improved endurance, safety and quality of life.
Fig. 1. Patient scores at his 2 admissions (day 1 and day 13).
Patients with advanced heart failure present new challenges for rehabilitation professionals. Typically, prolonged hospitalizations leave these patients with severe deconditioning and poor cardiac reserve to improve muscle strength and functional independence. The Memorial Rehabilitation Institute provides cutting edge rehabilitation and a collaborative approach with an advanced heart failure team to maximize quality of life for patients undergoing LVAD and cardiac transplantation.
By using a team-orientated approach with physical, occupational and speech therapy as well as rehabilitation nursing, neuropsychology, recreational therapy including adaptive sports and music therapy with daily supervision from a physiatrist, the patient had significant improvement in independence and quality of life. The rehabilitation team saw him improve from an LVAD s/p cerebrovascular accident (CVA) patient requiring assistance for gait and all ADL with severe deconditioning to a cardiac transplant patient leaving the rehabilitation centre at a modified independent level.
This case is of interest due to the patient’s medical complexity, as many patients who undergo cardiac procedures may develop further complications. As rehabilitation physicians it is important to highlight certain cases where there is a prolonged continuum of care to establish best practices on how to manage these patients to maximize functional gains and improvement in quality of life.
The authors would like to thank the advanced heart failure team at Memorial Regional Hospital for their collaboration on this and all our medically complex cardiac patients.


 Click to show fullsize
Click to show fullsize