
From the 1Department of Medical and Health Sciences, 2Department of Behavioural Sciences and Learning, Linköping University, Linköping, 3Department of Community Medicine and Rehabilitation, Rehabilitation Medicine, 4Department of Community Medicine and Rehabilitation, Physiotherapy, Umeå University, Umeå, 5Department of Medical and Health Sciences, Faculty of Medicine and Health Sciences, Linköping University, Pain and Rehabilitation Centre, Anaesthetics, Operations and Specialty Surgery Centre, Region Östergotland, Linköping, and 6Department of Clinical Sciences, Karolinska Institutet and Department of Rehabilitation Medicine, Danderyd Hospital, Stockholm, Sweden
Objective: To determine whether self-reported pain measures are associated with selection for multimodal or multidisciplinary rehabilitation (MMR) and whether this selection is influenced by sex.
Design: Cross-sectional cohort study.
Subjects: A total of 1,226 women and 464 men with chronic pain conditions from 2 university hospitals.
Methods: Drawing from the Swedish Quality Registry for Pain Rehabilitation (SQRP), data on pain, psychological symptoms, function, health, and activity/participation were collected. Multiple logistic regression was used to investigate association of pain measures with selection for MMR (no/yes) after multidisciplinary assessment. Covariates were: age, educational level, anxiety, depression, working status, and several pain measures.
Results: High pain intensity in the previous week (odds ratio (OR) 0.92; 95% confidence interval (CI) 0.86–0.99) and high pain severity (Multidimensional Pain Inventory) (OR 0.83; 95% CI 0.74–0.95) were negatively associated with selection for MMR, whereas higher number of pain quadrants was positively associated with selection for MMR. Similar results were obtained for women, but none of the measures was predictive for men.
Conclusion: This practice-based study showed that higher scores on self-reported pain were not associated with selection for MMR, and in women there was a negative association for higher pain intensity and pain severity. Thus, other factors than pain determine whether patients are selected for MMR.
Key words: multimodal treatment; multidisciplinary; chronic pain; gender; rehabilitation; primary healthcare.
Accepted Sep 30, 2016; Epub ahead of print Jan 18, 2017
J Rehabil Med 2017; 49: 161–169
Correspondence address: Paul Enthoven, Department of Medical and Health Sciences, Faculty of Health Sciences, Entrance 78, Floor 15, Linköping University, SE-581 83 Linköping, Sweden. E-mail: paul.enthoven@liu.se
Chronic pain is common and constitutes a major public health problem in the general population (1–3). Women report chronic pain more often than men (4). Because chronic pain is a complex phenomenon associated with physical and psychosocial impairment, influenced by individual beliefs and perceptions as well as socioeconomic factors (5–8), clinical practice has increasingly applied a biopsychosocial framework (9). This informs multimodal or multidisciplinary rehabilitation (MMR) programmes. There is a growing body of evidence that supports the use of MMR for treatment of patients with chronic pain (10–15). MMR programmes target different dimensions, such as pain relief, regain of function, reduction in psychological distress, and improved work ability. Treatment goals and strategies are determined with the patient’s input. Treatment usually covers several weeks and most activities are group based. MMR programmes often include education about chronic pain, training in psychological techniques to better cope with pain, and interventions to improve the patient’s physical health (e.g. physical exercise) (10, 12).
In Sweden, patients often seek primary care as a way to receive treatment. Since chronic pain conditions are complex and highly heterogeneous primary care patients with chronic pain can be referred for assessment in specialist care. Before a patient is offered MMR, a multi-professional team assesses whether the patient is suited for the programme. Since 2009, a rehabilitation guarantee for evidence-based rehabilitation has been implemented nationwide in Sweden, which is an initiative by the government to increase the return-to-work rate and reduce sickness absence by offering prompt access to MMR for persons with non-specific chronic pain, through influencing practice behaviour. The rehabilitation guarantee ensures that care providers receive financial compensation for each patient with chronic pain who completes a MMR. However, little is known about the characteristics of the patients selected for MMR.
Although chronic pain is influenced by physical, emotional and social factors, factors related to pain might have an important impact on the selection of patients for MMR. To our knowledge, only one recent study has investigated these aspects in a Swedish context. This study concluded that different pain characteristics did not play a dominant role in selection for MMR (16). As previous studies in the field of social sciences have not been able to replicate one another’s results, more research is needed (17). Large clinical studies should be conducted that focus on a true, real-world sample of patients.
The aim of this study was to investigate whether self-reported pain measures are associated with selection for MMR and whether this selection is influenced by sex. We hypothesized that higher scores on pain measures would be associated with more frequent selection for MMR and that there would be no difference in selection based on sex. A further aim was to explore the role of working status in selection for MMR.
This cross-sectional cohort study investigated patients with chronic pain (mainly musculoskeletal pain), in the age range 18–65 years, between 2008 and 2012. These patients were referred to the Pain and Rehabilitation Centre, University Hospital of Linköping (Linköping, Sweden) and the Pain Rehabilitation Clinic, University Hospital of Umeå (Umeå, Sweden). All patients who provided data to the Swedish Quality Registry for Pain Rehabilitation (SQRP; www.ucr.uu.se/nrs/) were recruited to the study. The SQRP is a national registry recognised by the Swedish Association of Local Authorities and Regions (SALAR). All participants gave informed written consent before the first assessment. Ethical approval was obtained from the Umeå Region Ethics Committee (Dnr: 2013/192-31). The study was performed in accordance with the principles of the Declaration of Helsinki.
At the northern site (Umeå), referred patients were assessed by teams comprising a specialist physician in rehabilitation medicine or by specialists in training, a physiotherapist, and a social worker and, if needed, a psychologist and occupational therapist. If the team considered the patient needed MMR and fulfilled the inclusion criteria (disabling chronic pain, on sick leave, or experiencing major interference in daily life, or no further investigations needed), they were recommended/selected for participation in a MMR programme. Exclusion criteria were ongoing major somatic or psychiatric disease or a history of significant substance abuse. The MMR programme was conducted in groups of 6–9 participants for 4 consecutive weeks and was based on cognitive behavioural principles and included physiotherapy, training in ergonomics, training in coping strategies, and education in pain management. The patients were encouraged to take an active part in goal setting.
At the southern site (Linköping), medical assessments were performed by a senior physician, primarily from specialists in rehabilitation medicine or similar specialties, or by specialists in training. In the majority of cases, the patient was also assessed by a psychologist, an occupational therapist, and a physiotherapist.
Patient inclusion and exclusion criteria were the same at both sites. The programme followed the same protocol at both sites.
Before the first assessment, the patients completed a questionnaire on background and clinical characteristics. Most of the included instruments cover the Initiative on Methods, Measurement, and Pain Assessment in Clinical Trials (IMMPACT) core outcome domains for the treatment of patients with chronic pain (9). The answers to the questionnaires were gathered in the SQRP, where the following data were retrieved:
HADS comprises 14 items evenly divided between anxiety (HAD-A) and depression (HAD-D) (18). Subscale scores range from 0 to 21. A score of 7 or less indicates a non-case, a score of 8–10 indicates a possible case, and a score of 11 or more indicates a definite case (18). The HADS was then dichotomized into groups having, or not having, a definite case of anxiety or depression. HADS has satisfactory psychometric characteristics (18, 19).
The West Haven-Yale Multidimensional Pain Inventory (WHY-MPI) is a 61-item self-report questionnaire that measures psychosocial, cognitive, and behavioural effects of chronic pain (20, 21) and is frequently used to evaluate the effect of MMR. This study used the subscales pain severity (3 items) and pain interference with daily life (11 items) from the psychosocial dimension. The pain severity subscale assesses patients’ perception regarding how pain interferes with their lives, including interference with family and marital functioning, work, and social-recreational activities and satisfaction with current level of functioning. The patient responded on a 7-point scale (range 0–6), with higher scores indicating higher impact of pain severity (pain severity, MPI) and higher pain interference with daily life (pain interference, MPI).
The SF36 represents multi-dimensional health concepts and measurements of the full range of health states, including levels of well-being and personal evaluations of health (22). The instrument has 8 dimensions (reported using a standardized scale from 0 to 100): physical functioning, role limitations due to physical functioning, bodily pain, general health, vitality, social functioning, role limitations due to emotional problems, and mental health. Based on these 8 scales, the instrument calculates a physical component summary (PCS SF36) and a mental (psychological) component summary (MCS SF36) (23). The PCS and the MCS are reported in the current study. Higher scores indicate better health.
The EQ-5D, consisting of 2 parts, was used to measure health-related quality of life (HRQoL) (24, 25). The EQ-5D contains 5 dimensions: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. Each dimension has 3 levels: no problems, some problems, and extreme problems. The answers on the 5 dimensions are converted into a single EQ-5D index that ranges from −0.594 to 1, where 1 indicates optimal health. The EQ VAS records the respondent’s self-rated health on a vertical visual analogue scale that ranges from 0 (“worst possible health state”) to 100 (“best possible health state”).
The TSK measures fear of movement and re-injury (26, 27). The questionnaire comprises 17 items. Each item has a 4-point Likert scale, ranging from “strongly disagree” to “strongly agree”. The total score ranges from 17 to 68; scores higher than 38 for men and higher than 36 for women indicate high pain-related fear (28). The TSK has shown to be a reliable assessment tool in chronic pain populations (27, 29, 30).
At assessment, the team members had information from the patient and access to the answers to the above-mentioned questionnaires. The final selection for the MMR programme was made in agreement with the patient. Outcome was defined as selection for MMR (no/yes).
The statistical package IBM SPSS 23.0 was used in all analyses. Differences in patient characteristics between men and women were investigated with unpaired t-test, χ2 test, or Wilcoxon signed-rank test. Patients with missing value for working status were excluded from the analyses.
Multiple logistic regression was used to investigate the association of pain measures with selection for MMR (no/yes, dependent variable). Odds ratios (OR), together with the 95% confidence intervals (95% CI), were calculated to reflect the strength of the association. Nagelkerke R2 was reported as a pseudo-measure of the proportion of variance explained by the predictors.
The following pain measures (independent variables) were investigated separately: pain intensity in the previous week NRS (0–10); pain severity (MPI); pain interference (MPI); number of pain sites (0–36); pain location varies (ref = localized pain); and number of body quadrants with pain (0–4).
Two models were investigated: Model 1 – adjusted for age + education; Model 2 – pain intensity, pain severity, and pain interference in the previous week adjusted for age, education + pain sites; pain sites, varying location, and number of quadrants adjusted for age, education + pain intensity in the previous week. Based on Model 2, we tested whether anxiety and depression, separately and together, influenced the association between pain measures and selection for MMR (31). Preliminary analysis indicated that working status was significantly associated with selection for MMR and the decision was made to perform Model 1–2 separately using the selection employed/student/jobseeker (thereby excluding the patients who were not gainfully employed).
The main results, limited to the data that are unique for this study (i.e. no overlap with Haukenes et al.), are presented in Table SI and Table SII to enable future systematic review or meta-analysis.
In total, 1,692 patients answered a questionnaire before the assessment, of whom 108 (6.4%) had missing values on working status, resulting in a study population of 1,584 patients. Table I shows patient characteristics and a comparison between men and women. In addition to the results for all patients, the results for the selection employed/student/jobseeker are shown.
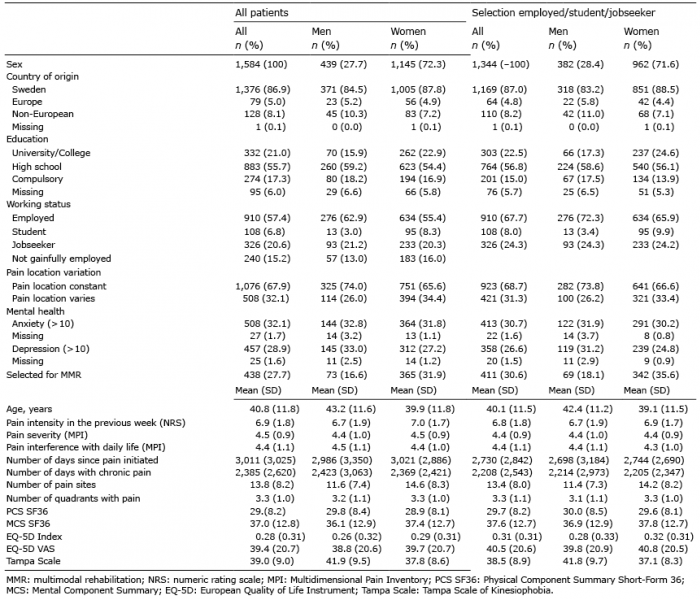
Table I. Patient characteristics for all patients and for the selection employed/student/jobseeker. Values for men and women are reported separately
More women than men had a university/college education (p = 0.012) and women had a lower mean age (p < 0.001) (Table I). Women more often had a varying localization of the pain (p = 0.001), less depressive symptoms (p = 0.015), higher pain intensity during the previous week (p = 0.021), a higher number of pain sites (p < 0.001), and a higher number of body quadrants with pain (p = 0.002). Compared with men, women had higher general health, as measured by the EQ-5D Index (p = 0.046), and a lower level of kinesiophobia, as measured by the TSK (p < 0.001) (Table I). In total, 438 (27.7%) patients were selected for MMR. Patients selected for MMR were younger (mean age) 37.6 ((standard deviation (SD) 10.4) years vs 42.1 (12.1) years) (not shown in Table) and more often women (p < 0.001) (Table I).
The selection employed/student/jobseeker contained 1,344 patients. They were younger (mean 40.1 (SD 11.5) vs 45.2 (SD 12.6) years) and had a higher education (p < 0.001) compared with those not gainfully employed. They also had significantly better values on all health-related variables (p = < 0.001 –0.006) (Table I). However, the proportion of women and of men was similar. Of those not gainfully employed, 27 (11.3%) were selected for MMR. In the selection employed/student/jobseeker, a higher proportion of the women compared with the men had Sweden as country of origin (p = 0.028) (Table I). More women than men had a university/college education (p = 0.010) and women had a lower mean age (p < 0.001). Women more often had a varying localization of the pain (p = 0.010), less depressive symptoms (p = 0.010), a higher number of pain sites (p < 0.001), and a higher number of body quadrants with pain (p = 0.008). Compared with men, women had higher general health, as measured with the EQ-5D Index (p = 0.017), and lower level of kinesiophobia, as measured with the TSK (p < 0.001) (Table I).
In the selection employed/student/jobseeker, 411 (30.6%) patients were selected for MMR. Patients selected for MMR were younger (mean age 37.6 years (SD 10.5) vs 41.1 years (SD 11.8)) (not shown in Table), and more often women (p < 0.001) (Table I). In this selection, the differences between women and men were similar to differences found in the selection all patients, except for the above-mentioned difference in country of origin, and for the selection employed/student/jobseeker the mean pain intensity in the previous week was not significantly different between women and men (Table I). The pain measures that were associated with selection for MMR are shown in Table II.
Table II. Logistic regression between pain-related measures (independent variables) at baseline and selection for multimodal rehabilitation (no/yes, dependent variable); odds ratio (OR) and 95% confidence intervals (95% CI). Results for all patients and for the selection employed/student/jobseeker
High pain severity (MPI) (OR 0.874; 95% CI 0.768–0.993) was negatively associated with selection for MMR, and higher numbers of body quadrants with pain (OR 1.163; 95% CI 1.034–1.308) was positively associated with selection for MMR, whereas pain intensity in the previous week, pain interference with daily activities and number of pain sites were not (Table II). In Model 2, adjusted for pain sites, even higher pain intensity in the previous week (OR 0.923; 95% CI 0.863–0.988) and higher number of pain sites (OR 1.016; 95% CI 1.001–1.031) were associated with selection. For all calculations, the Nagelkerke R2 value varied from 0.042 to 0.054.
For men, none of the pain-related measures were associated with selection for MMR. The Nagelkerke R2 value varied from 0.052 to 0.067. For women, high pain intensity (VAS) during the previous week (OR 0.925; 95% CI 0.858–0.998) and high pain severity (MPI) (OR 0.827; 95% CI 0.713–0.959) were negatively associated with selection for MMR, and higher numbers of body quadrants with pain (OR 1.184; 95% CI 1.036–1.352) was positively associated with higher selection for MMR (Table II). The Nagelkerke R2 value varied from 0.035 to 0.052.
Adjustment for different pain measures (Model 2; Table II) did not change which measures were significant for selection for MMR, except for the above-mentioned change in association for all patients regarding pain intensity in the previous week and higher number of pain sites in Model 1. Adjustment for anxiety and depression, separately and together, did not influence the association between pain measures and selection for MMR (not shown in Table).
A higher proportion of those employed/student/jobseeker were selected for MMR compared with those not gainfully employed (411 (30.6%) vs 27 (11.3), χ2 = 38.035, p < 0.001). Selecting only those employed/student/jobseeker influenced the association between pain measures and selection for MMR (Table II); for all patients, high pain intensity in the previous week and high pain severity (MPI) were no longer associated with selection for MMR. High pain interference (MPI) (OR 1.169; 95% CI 1.039–1.315) and higher numbers of pain sites (OR 1.019; 95% CI 1.003–1.034) were now positively associated with selection for MMR. Higher number of quadrants with pain was still positively associated with selection for MMR (OR 1.201; 95% CI 1.064–1.355). For all calculations, the Nagelkerke R2 value varied from 0.026 to 0.038.
For men, none of the pain-related measures were associated with selection for MMR. The Nagelkerke R2 value varied from 0.044 to 0.053. For women, a similar pattern was seen as for the whole selection employed/student/jobseeker, except that a higher number of pain sites was no longer associated with selection for MMR (Table II). The Nagelkerke R2 value varied from 0.020 to 0.036.
Adjustment for different pain measures (Model 2; Table II) did not change which measures were significant for selection for MMR. Adjustment for anxiety and depression, separately and together, did not influence the association between pain measures and selection for MMR (not shown in the Table). Variables measuring duration of pain were not included in the analyses due to a high number of missing values.
The results limited to the data that were unique for this study (i.e. no overlap with Haukenes et al. (16), see Table SI and Table SII) were quite similar; In the unique women patients, higher pain intensity in the previous week was no longer associated with selection for MMR. In the selection employed/student/jobseeker, higher pain interference (MPI) was no longer associated with selection for MMR in all patients; in men, having a pain location that varied was negatively associated with selection, and in women, having a higher number of pain sites was associated with selection for MMR.
This study showed that higher scores on different measures of self-reported pain did not lead to selection for MMR, and that for women there was a negative association for some pain measures. In general, the associations between the pain measures and selection for MMR were low. Twice as many women than men were selected for MMR and fewer women than men reported depressive symptoms. Women reported somewhat higher pain intensity during the previous week and had more spreading of the pain (number of pain sites and number of quadrants with pain). Women reported somewhat higher general health (EQ-5D index) and had somewhat lower kinesiophobia (Tampa Scale).
Only a minority of the patients referred by primary care were selected for MMR. The assessment and selection process for MMR takes substantial (human and other) resources. However, the MMR selection process is necessary to ensure that only patients who may benefit from the intervention are selected and to exclude patients in need of further investigation or unimodal rehabilitation by a single profession. A number of factors might play a role, such as physical ability, mental capability, and expectations about the future. The patients were referred by general practitioners to specialist clinics, so they represent a selected group of patients with more severe consequences of pain than patients being treated in primary care.
Our results confirm the results reported by Haukenes et al. (16) Since the patients in our study were included between 2008 and 2012 and the patients in the study by Haukenes et al. were included between November 2007 and December 2010, more than half of the included subjects from the northern centre were the same (n = 452, 28.5% of the total sample). However, even after limiting the data for unique patients (i.e. no overlap with Haukenes et al. (16), see Table SI1 and Table SII1), the results were quite similar. As with previous studies (12), the majority of patients who participated in MMR were women. The fact that more women than men experience chronic pain (4, 32) might partly explain the larger proportion of women participating in MMR. Jensen et al. (33), in a long-term study of outcomes for women and men, reported that women benefit more than men from MMR. There were some differences between our study and the study by Haukenes et al. (16): our study was performed at 2 specialist pain rehabilitation clinics rather than one and the number of included patients was approximately twice as high (16). Furthermore, we included some additional pain measures that showed that higher pain intensity during the previous week was associated with a less likely selection for MMR, and a higher number of quadrants with pain was associated with a more likely selection for MMR. As in the study by Haukenes et al. (16), adjustment for anxiety and depression did not influence the association between pain measures and selection for MMR.
Surprisingly, for the selection “all patients”, higher scores on pain intensity, and interference with daily life did not increase selection for MMR. An important aspect of healthcare in modern societies is the principle of equity, e.g. prioritization of healthcare is based on the needs of the patient. Patients with higher self-reported pain may have greater suffering, which might indicate a higher need for healthcare. Previous studies have shown that MMR has a beneficial effect on pain severity (34, 35), pain interference, and other measures of pain (8, 9, 35). Some studies have shown no difference regarding pain intensity between MMR and less extensive treatment (12). However, these studies did not define pain intensity as an outcome, as they focused more on behavioural change and long-term consequences, such as sick leave and coping. For women, some of the pain measures were predictive for selection for MMR; for men, none of the pain measures were predictive for selection for MMR, results that generally agree with Haukenes et al.’s results(16). Fewer men were included in the study, which might explain why associations between pain measures and selection for MMR did not reach statistical significance for men.
In contrast to the study by Haukenes et al. (16), working status did influence which pain measures were significant for selection for MMR. The patients able to work (the selection employed/student/jobseeker) were somewhat younger and had better health in most dimensions compared with all patients. Because the main goals of the national rehabilitation guarantee were to increase the return-to-work rate and reduce sickness absence, it was not surprising that a higher proportion of those employed/student/jobseeker were selected for MMR compared with those not gainfully employed (individuals who probably would not return to work). Separate analyses showed that employed/student/jobseeker patients had higher pain interference, and a higher number of pain sites was positively associated with selection for MMR, but higher pain intensity in the previous week was not. This finding suggests that for those either working or with the potential to return to work interference with activities of daily living and a larger number of pain sites became more important for selection for MMR, whereas the severity of the pain became less important, which might inform the MMR team on what kind of treatment that should be incorporated in the MMR programme to improve management of these patients. Although somewhat larger than for all patients, the associations between the pain measures and selection for MMR were small (i.e. low Nagelkerke R2 values).
Women were more often selected for MMR compared with men, a finding that was also found in a previous study (16). The reasons for this difference between men and women are unknown. Preconceptions about which patients fit into a certain MMR programme (36) and attitudes of healthcare personnel about which patients might benefit from MMR might play a role (36, 37). Studies suggest that age, sex, education level, place of origin, ethnicity, verbal skills and social class might play a role in how a patient’s needs are viewed and who is offered rehabilitation (38–40), and increasing awareness about these matters should be integrated in professional education if not already present, to help professionals offer equal care to patients with chronic pain (40). It should also be noted that selection for MMR does not depend only on the opinion of the healthcare professionals; even if offered, the patient could choose not to participate in MMR.
A strength of the present study is the relatively high number of patients included. Furthermore, the generalizability of data to the national level was enhanced since recruitment was done at 2 clinic departments for pain rehabilitation; 1 in northern Sweden and 1 in southern Sweden, with experienced professionals and a high level of staff continuity. When assessing the patients, standardized procedures were used. Moreover, the data were retrieved from the SQRP, the national quality register for pain rehabilitation, and includes approximately 80% of pain management programmes in Sweden (34).
The low Nagelkerke R2 values found in this study suggest that only a small part of the selection for MMR could be explained by the different pain variables. Logistic regression does not have an equivalent to the R2 that is found in linear regression. There are a wide variety of pseudo-R-square statistics (e.g. the Nagelkerke R2) (9). Because this statistic does not mean what R2 means in linear regression (the proportion of variance explained by the predictors), the Nagelkerke R2 values should be interpreted with caution.
The pain measures included in the current study are validated and frequently used in clinical practice for assessment of pain conditions that are relevant for MMR. Because the procedures used for selection for MMR are similar throughout Sweden and relatively similar across countries that offer MMR (34), we assume that generalizability is good on a national level and that the external validity is relatively good. Further studies are needed to investigate which factors influence selection for MMR.
This practice-based study showed that higher scores on self-reported pain did not lead to selection for MMR, and that for women there was a negative association for higher pain intensity and pain severity. Factors other than pain influence which patients are selected for MMR.
This study was supported by the Swedish Social Insurance Agency, the research programme REHSAM and AFA Insurance. The funders had no role in study design, data collection, data analysis, preparation of the manuscript, or decision to publish.
The authors declare no conflicts of interest.


 Click to show fullsize
Click to show fullsize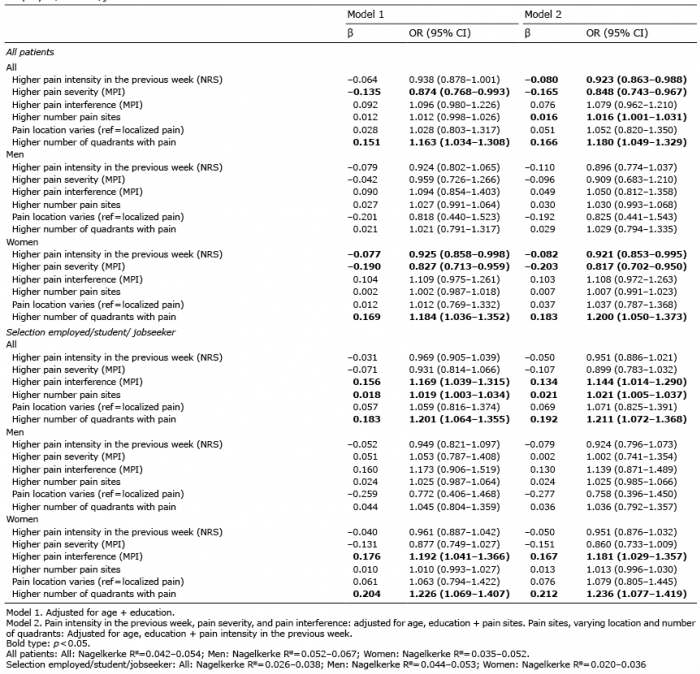 Click to show fullsize
Click to show fullsize