
From the 1Department of Physical Medicine and Rehabilitation, Ankara Physical Medicine and Rehabilitation Training and Research Hospital and 2Department of Physical Medicine and Rehabilitation, Ankara University Faculty of Medicine, Ankara, Turkey
Objective: To evaluate the feasibility and safety of Xbox KinectTM training of the upper extremity in subacute stroke rehabilitation.
Design: A single-blind, randomized controlled, pilot study.
Patients: Twenty consecutive patients with stroke.
Methods: Participants were allocated randomly to 2 groups: the control group received conventional
therapy and the experimental group received additional Xbox KinectTM training for 20 sessions. Feasibility and safety were evaluated by treatment attendance rate, patient feedback, proportion of adverse events, and Borg Scale (Borg CR10).
Results: Twenty of 131 screened individuals were recruited. Data for 19 patients (73.7% male; mean age 62 years (range 38–79)) were analysed. Treatment attendance ratio for total training time and training time/session was 87% and 90%, respectively. All participants reported that training with the Xbox KinectTM was enjoyable and beneficial. No serious adverse events occurred. Fatigue was the most common adverse event. The mean Borg CR10 score was 7.80, reflecting a very high level of fatigue. The experimental group showed significantly greater improvement than the control group in the Box and Blocks Test, Wolf Motor Function Test and Brunnstrom motor recovery stages.
Conclusion: Xbox KinectTM training appears feasible and safe in upper extremity rehabilitation after stroke. It could enhance motor and functional recovery of the affected upper extremity as an adjunctive method.
Key words: stroke; rehabilitation; serious games; virtual reality; Xbox KinectTM.
Accepted Oct 19, 2017; Epub ahead of print Dec 14, 2016
J Rehabil Med 2017: 49: 22–29
Correspondence address: Tuba Alkan Türkbey, Physical Medicine and Rehabilitation Specialist, Department of Physical Medicine and Rehabilitation, Ankara Physical Medicine and Rehabilitation, Training and Research Hospital, Türkoca Sokak, No. 3, Samanpazar?, Alt?nda?, 06230, Ankara, Turkey. E-mail: tubaliskan@gmail.com
Stroke is a common cause of death and acquired adult disability that has been described as a catastrophic event for both patients and their families (1, 2). Traditional rehabilitation approaches have limited benefit in terms of the restoration of motor function and minimization of the level of disability (3). Intensive, repetitive and task-oriented exercises are useful for enhancing neuroplasticity followed by motor recovery (4, 5). However, attaining these features in treatment requires increased staffing levels, high levels of motivation of the patient during tedious training, and location of the patient at a specialized facility (6). For this purpose, virtual reality (VR) technology has emerged as a new technique in neurorehabilitation. VR is a novel technology that presents opportunities to users for interacting with 3-dimensional (3D) virtual environments, similar to real-world environments, generated by computer hardware and software (7). Interaction between the user and the virtual environment is provided by different mechanisms; either by simple hand-held devices such as a joystick, mouse, or by more complex and expensive systems composed of head-mounted devices, concave surfaces, and specialized data gloves (8). VR systems also provide the users with immediate visual, auditory or tactile feedback, which have been reported to optimize motor learning (9). The first studies in this field utilized complex and high-cost VR systems, which required specialized staff and appropriate facilities. On the other hand, commercial games consoles used in the entertainment sector have started to replace previously mentioned VR systems in recent years due to their low cost and high availability (8, 10).
Commercial interactive games consoles, including the Nintendo WiiTM and the Sony Playstation EyetoyTM, have been used in stroke rehabilitation with variable success and seemed to be safe, feasible and effective treatment options (10–14). However, motion capture controllers, such as the Nintendo WiimoteTM, are not sensitive enough to accurately track user’s movements due to the fact that patients can deceive the system by pretending to make the desired movement (6). In addition, holding a device during training can be uncomfortable for the user, and thus cause limitation in the range of the target patient population (15). The more recently released Xbox KinectTM (Microsoft Xbox 360, Redmond, Washington, USA) games console has advantages over other systems, such as not requiring any special controller and having a more sensitive sensor, which provides more accurate motion-capture (6, 15). However, there is limited evidence on the clinical utility of the Xbox KinectTM in stroke rehabilitation (10, 16–18). The current Xbox KinectTM has been designed for physically and mentally healthy people, as were previous consoles. Therefore, the safety and feasibility of the system should be evaluated before it is used as an alternative or adjunctive training method in patients after stroke. To the best of our knowledge, no studies have evaluated the clinical feasibility of use of the Xbox KinectTM in stroke rehabilitation.
The aim of this pilot study was to evaluate the feasibility and safety of Xbox KinectTM training of the upper extremity in subacute stroke rehabilitation. The secondary aim was to evaluate its efficacy on upper extremity motor and functional recovery.
Reporting of this trial was conducted according to the CONSORT (Consolidated Standards Of Reporting Trials) checklist on pilot studies (19, 20).
The study is a single-blind, randomized controlled, pilot trial. It was approved by the Ankara University Faculty of Medicine Ethics Committee (10 December 2012, number 20-645-12 resolution) conducted in accordance with the Declaration of Helsinki. The study was registered at ClinicalTrials.gov; study number NCT02759328. The full trial protocol is available at https://clinicaltrials.gov/ct2/show/NCT02759328?term=Xbox+Kinect&rank=2.
Patients after stroke who were hospitalized for inpatient rehabilitation at the Ankara University Faculty of Medicine, Cebeci Research and Application Hospital, Physical Medicine and Rehabilitation Clinic from December 2012 to March 2014, were assessed to determine their eligibility for the study. All patients were diagnosed with stroke by a neurologist according to World Health Organization (WHO) stroke definition and confirmed by neuroimaging (computed tomography or magnetic resonance imaging). Patients after stroke who met the following criteria were recruited; first-time ischaemic or haemorrhagic stroke occurring in the last 9 months, between 18 and 80 years of age, Brunnstrom motor recovery stage (BMRS) (21) in the affected upper extremity ≥ 3, ability to understand and follow simple explanations and commands, Mini-Mental State Examination (22) score ≥ 24. Patients were excluded if they had a history of epilepsy or seizure (except childhood febrile seizures), arthritis or pain restricting the repetitive training of the affected upper extremity, severe aphasia, neglect phenomena, cognitive or psychiatric disorders, ≥ grade 3 spasticity in the affected upper extremity according to Modified Ashworth Scale (MAS) (23, 24), medical conditions that may affect physical performance or the physical activity may become unsafe (unstable angina, myocardial infarction within the last 3 months, uncontrolled blood pressure, pulmonary disease, etc.), or participation in another clinical trial.
All patients who fulfilled the inclusion criteria received a detailed explanation of the study. Written informed consent was obtained from all participants prior to enrollment.
Patient’s characteristics were collected at baseline, including socio-demographic features (age, sex, marital status, educational level, vocation), stroke type, time from stroke onset to enrollment, affected side, handedness, comorbid conditions, spasticity grade (according to MAS) and motor recovery stages (according to BMRS). Affected upper extremity was examined using the Box and Blocks Test (BBT) (25, 26) and the Wolf Motor Function Test (WMFT) (27, 28). Baseline level of functional independence was assessed using the Functional Independence Measure (FIM) (29).
Participants were randomly allocated to 2 groups: an experimental group and a control group. Block randomization was preferred to ensure equal numbers of patients between the 2 groups and a block size of 4 was chosen. Sequentially numbered, opaque, sealed envelopes were used for the allocation concealment. Each block was placed in one of these envelopes and the envelopes were opened according to a computer-generated random-number table.
The study was conducted as a single-blind trial and only the assessor was blinded to patient randomization. Because of the nature of the intervention, neither the patients participating in the study nor the supervising occupational therapist (OT) was blinded. The study coordinator who was responsible for the randomization and allocation concealment was also not blinded. To protect blindness of the assessor, the OT gave information only to the study coordinator when an adverse event occurred during the intervention period.
Both the experimental group and the control group received a conventional rehabilitation programme for 4 weeks (60 min/day, 5 days/week). The experimental group underwent additional training with the Xbox KinectTM for 4 weeks (60 min/day, 5 days/week) in parallel with the conventional rehabilitation programme.
Conventional rehabilitation programme. The conventional rehabilitation programme consisted of passive and active range of motion exercises, therapeutic stretching, muscle strengthening, neurophysiological exercises, sitting, standing, balance and gait exercises, occupational therapy and activities of daily living training, such as eating, grooming, dressing, toileting and transfer. The treatment protocol was individualized according to the goals, which were determined depending on each patient’s needs and functional level.
Xbox KinectTM based virtual reality training. Virtual reality training was administered using the Xbox KinectTM games console. The system comprised 3 components; KinectTM sensor, Xbox 360TM games console, and 42-inch LCD television. KinectTM was first introduced in November 2010 by Microsoft as a motion-sensing input device for the Xbox 360TM games console. This low-cost motion-capture device has an infrared-based depth-sensing technology, which provides full-body 3D motion data to the games console without any need for hand-held interface controllers, markers, etc. The user can follow his/her real world movements and interact with the games console through a virtual avatar on the screen created by the system. In addition, the system assists the user with audio and visual feedback.
The games console was placed in a separate room in order to avoid the effects of external factors to the patients. The training was performed in a sitting position 2.25–2.75 m from the television screen. As the training software, commercially available Bowling from the Kinect Sports package and Mouse Mayhem from the Dr Kawashima’s Body and Brain Exercises package, both of which require use of the upper extremities, were chosen and each game was played for 30 min. Detailed information and motion patterns related to these games are shown in Table I.
Table I. Features of the selected Xbox 360 KinectTM games
Primary outcome measures. The primary outcome measures of this pilot study are related to the feasibility and safety of the Xbox KinectTM in subacute stroke rehabilitation. Treatment attendance ratio, which is the proportion of the completed training time to the planned training time, was used as the primary feasibility outcome. The treatment attendance ratios were calculated for 3 different measurements: total training time, training time per session and number of sessions. Training time of each session was measured by means of a stopwatch by the OT who supervised the experimental intervention. Training time per session was calculated by dividing the total training time by the number of treatment sessions attended by each patient. In addition, the results of the patient feedback survey was used as a feasibility outcome. A patient feedback survey has been developed to determine participant’s opinions related to safety, ease-of-use and enjoyment of the game system, pain or fatigue during or after the training, duration of sessions, contribution to recovery, using as a treatment approach and suggestion to the other patients. After completion of all treatment sessions, all participants filled the patient feedback survey through a face-to-face interview with the OT.
The ratio of patients who had adverse events related to the intervention or any serious adverse event during the study was defined as the primary safety outcome. Rating of perceived exertion measured according to the Borg Category-Ratio 10 (Borg CR10) scale (30) was also used as a safety outcome. The Borg CR10 scale ranges from 0 (no exertion at all) to 10 (maximal exertion) and it was used to measure the perceived exertion, degree of fatigue or level of effort required to perform tasks during the training. After each session, patients were asked to report their perceived exertion according to the Borg CR10 scale.
Assessments of all primary outcome measures were performed by the same OT who supervised the experimental intervention.
Secondary outcome measures. To determine the efficacy of the intervention, BBT for gross manual dexterity, WMFT for the motor function of the upper extremity, self-care subscale of FIM for upper extremity related functional independence level, and upper extremity BMRS for motor recovery were used.
BBT is a test assessing gross manual dexterity, during which a patient is required to move as many blocks as possible (1 at a time) from one side to the other side of a separator placed in a box for a period of 1 min. The total number of transferred blocks was defined as the score of BBT (25, 26).
The current version of the WMFT, which contains 17 tasks (15 timed and 2 strength tasks), assesses motor functions of the upper extremity. The 2 strength tasks were not included in this study because performance of these tasks is not counted in the total performance time or functional ability score of the test. Therefore, a shorter version of the WMFT, which contains 15 timed tasks, was used. Patients were instructed to perform each task as fast and accurately as possible. For each task, accomplishment time was measured and quality of movement was assessed according to functional ability scale of the test. The median value of the measured durations was defined as the WMFT performance time score (WMFT-PTS). The mean value of the functional ability scale scores was defined as the WMFT functional ability score (WMFT-FAS) (27, 28).
The FIM was used to assess patient’s level of functional independence. It consists of 18 items grouped under 2 major domains of physical/motor function (13 items) and cognitive function (5 items), and 6 subscales (self-care performance, sphincter control, transfers, locomotion, communication and social–cognition). FIM is scored from 1 (total assistance) to 7 (complete independence) for each item. The reliability and validity of the Turkish adaptation of the FIM has been documented previously (29). Total score obtained from 6 items in the self-care performance subscale was defined as the FIM self-care score in the study.
BMRS assesses motor recovery after stroke and is ranged from 1 (flaccidity, no voluntary or reflex activity is present) to 7 (return to normal function, return of fine motor skills) according to the spasticity degree and the presence of voluntary movements (21). BMRS of the affected upper extremity was evaluated in the current study.
Assessments of all secondary outcome measurements were performed by the same assessor, who was blinded to patient randomization and was not involved in administration of study interventions. These assessments were carried out at baseline and at the end of the training.
Data obtained were analysed using R Software. Mean, standard deviation, median, min–max and percentile values were calculated for the socio-demographic and clinical features, primary and secondary outcome measures. The Wilcoxon signed-rank test was used to evaluate differences within groups. The Mann–Whitney U test was used to evaluate differences between groups. p-values less than 0.05 were considered statistically significant.
A total of 131 patients were assessed for participation in the study. Of these, 111 patients were excluded as they did not meet the inclusion criteria. No patients refused consent. A total of 20 patients were enrolled in the study and 10 were randomized to each group. All participants in the experimental group completed their treatments. One participant in the control group withdrew from the study prior to completing the treatment; he requested to be discharged. The remaining 9 participants in the control group completed their treatments. The flow diagram of patients based on CONSORT (31) is shown in Fig. 1.
Fig. 1. Flow diagram of patients based on CONSORT (Consolidated Standards Of Reporting Trials).
Participants had a mean age of 62 years (range 38–79 years) and the mean time since stroke was 47 days (range 13–125 days). None of the participants had received rehabilitation before recruitment to the study. Baseline characteristics of the participants are shown in Table II. There were no significant differences between the 2 groups for baseline socio-demographic and clinical features. In addition, no significant differences between groups were found at baseline with respect to the secondary outcome measurements (motor and functional levels of the participants).
Table II. Baseline characteristics of the patients
The primary outcomes are shown in Table III. The mean total training time was 1,048 min, which was equal to 87% of planned total training time. Participants attended a mean of 19.2 sessions (96% of planned) with a mean session time of 54.1 min. Seven of 10 patients in the experimental group completed all their treatment sessions. Among the remaining 3 patients, one patient attended 18 sessions, the other one attended 19 sessions and the last one attended 15 sessions. The reasons for the missing treatment sessions were attending tests and consultations for their medical problems and days off for personal requirements. Seven of 9 patients in the control group completed their all treatment sessions. The reasons for the missing treatment sessions were the same as those in the experimental group.
Table III. Feasibility and safety of the Xbox KinectTM training (experimental group, n = 10)
According to the patient feedback survey, all participants agreed that training with the Xbox KinectTM was enjoyable and had contributed to his/her recovery. Ninety percent of the patients noted that the intervention could be used as a treatment approach and that they would suggest it to other patients. Seventy percent of the participants expressed that the training was safe, but 60% of the patients said that it was not easy and 80% stated that they felt tired after the intervention. Eighty percent of the participants found the session duration sufficient and 90% of the patients indicated that there was no need to prolong the duration.
During the study period there were no serious adverse events or medical issues that led to drop-outs (Table III). The most common symptom was fatigue. All the symptoms disappeared with rest and none of them interfered with the training of patients. The mean Borg CR10 scale score was 7.8, which corresponds to “very hard” according to the scale description. The only adverse symptom was fatigue in the control group during or after the conventional rehabilitation programme. Two of 9 patients in this group reported fatigue that did not require ending the therapy session.
The secondary outcomes for both groups are shown in Table IV. There were significant improvements in all parameters in the experimental group as well as the control group (p < 0.05). When the 2 groups were compared with respect to changes from baseline to post-intervention, the experimental group had significantly more improvement in the BBT, WMFT functional ability scale and upper extremity BMRS than the control group. A post-hoc power analysis was then performed and the power of the current sample size to detect a difference of 8.9 blocks in the BBT scores was calculated as 0.89 when α = 0.05.
Table IV. Efficacy of the Xbox KinectTM training in upper extremity rehabilitation
As a new trend in stroke rehabilitation, high-intensity, repetitive and task-oriented exercises are used to improve motor and functional recovery (3–5). The Xbox KinectTM games console appears to be a good option to achieve these strategies due to its commercial high-availability, low-cost, ease of use with no need for holding or wearing any device, high-sensitivity to accurately capture the movements of the user, feedback on performance, advanced level of enjoyment and interest through enriched environments to encourage a higher number of repetitions and to increase patient’s motivation (6, 8, 10, 15). This pilot study represents the first trial evaluating the clinical feasibility of the Xbox KinectTM training in subacute stroke rehabilitation.
The possible range of stroke survivors for whom an intervention may be appropriate is an important applicability criterion of the intervention. Reported eligibility rate, defined as the proportion of the recruited participants to screened ones, was 26% in a recent Cochrane Review on VR in stroke rehabilitation (8). This value was 15.3% in our study (Fig. 1). In addition to excluding patients with visual or communication deficits or cognitive impairments similar to the other studies (8), having a chronic stroke or a BMRS in the affected upper extremity < 3 were the common reasons for exclusion in the current study, which may explain the lower eligibility rate in this study. Unlike the time since stroke criterion, the BMRS criterion was dictated by the necessity of attaining the calibration pose of the game system. To achieve the skeletal system calibration by KinectTM, the patient has to abduct his/her arms approximately 90° and hold this position for a few seconds without moving. Because of patients with BMRS in the affected upper extremity < 3 would not be able to complete this calibration procedure, we did not include these patients in the study. The difficulty in the calibration method of the KinectTM has also been reported previously (15). On the other hand, it should be kept in mind that limited applicability is not specific to this intervention. It might also be a problem with other treatment approaches, such as constraint-induced movement therapy and occupational therapy, which are used for selected patient groups (5).
Xbox KinectTM training had a high time-related feasibility, reflected by considerably high treatment attendance ratios in the current study. In other studies using the Xbox KinectTM it was planned that patients after stroke would receive 1–40 sessions in total, 30–60 min per session, but none of these studies reported the completed training time (16–18). In a clinical feasibility study using a customized interactive game system with a 3D sensor of the same technology as used in the KinectTM the treatment attendance ratio was 91% (32). The completed total training time was 76% in a VR study using Nintendo WiiTM (33). Considering these high ratios, it can be said that the use of interactive games consoles including the Xbox KinectTM is feasible for an appropriate group of patients after stroke.
A recent review suggests that researchers should also evaluate patients’ motivation, engagement and level of enjoyment in studies using video games consoles (8). In our study, there was a consensus among the patients that the training was enjoyable and helpful. In a study where the Xbox KinectTM and Nintendo WiiTM were compared, the patients found the former more enjoyable (34). It should be remembered that patients’ enjoyment and belief in benefits of a treatment may improve engagement in a therapy and intensity of training as a reflection of increased motivation. The patient feedback survey showed that training with the Xbox KinectTM is a user-friendly treatment approach.
The system was proven to be safe with only mild adverse events reported during and after the intervention. Fatigue and arm pain caused some patients to stop an intervention session earlier than planned. However, these patients continued to participate in the following sessions. Although 3 patients reported arm pain, there was no tendinitis underlying this. Video games related tendinitis cases (named as “Nintendinitis” and “Wiitis”) have been reported previously (35, 36). This situation may be explained by Xbox KinectTM not having any need for holding or wearing a device. Among the other reported symptoms, nausea, dizziness and headache might be related to “cybersickness”, which was reported before as a disadvantage of virtual reality systems (37).
High perceived rates of exertion were reported according to the Borg CR10 scale in the current study. Although the patients noted a high level of fatigue, none of them dropped out of the training sessions, and the treatment attendance ratios were also high. Perceived exertion rates may be affected by a number of factors, including individual features, training duration, console and game selection. According to a previous study, lower exercise capacities of the patients after stroke might be the reason for the reported disproportionally high perceived rates of exertion due to reaching higher percentages of their maximal exercise capacity (34). On the other hand, patients after stroke have been shown to overestimate the exercise effort and this can be related to stroke-induced impairments, physiological, pharmacological and psychological factors (38). The session duration in the current study was relatively longer than the other studies using the Xbox KinectTM in patients after stroke (16, 17). This might be a reason for the high perceived exertion rates observed. Kafri et al. (34) measured the amount of energy expenditure (EE) of the participants while playing the same game (“boxing”) with 2 different games consoles. Results showed that EE with the Xbox KinectTM was higher than that of the Nintendo WiiTM. This difference was explained by the highly sensitive motion capture capabilities of the KinectTM. The occupational therapist (OT) who supervised the intervention in the current study noticed that patients were getting tired particularly while playing the Mouse Mayhem game. In contrast to the other selected game (“bowling”), Mouse Mayhem is a time-dependent game that requires playing at high speed. As mentioned in a previous report (34), features of the selected games may affect the perceived exertion rates. In accordance with the Borg CR10 scale scores, the results obtained from the patient feedback survey showed that 80% of the patients felt tired after the intervention. In addition, reporting of difficulty by some patients may be related to high degrees of fatigue. As an advantage to a previous feasibility study, which used a customized interactive game system with a similar technology used in the KinectTM (32), our study represents longer-term feasibility and safety of the Xbox KinectTM.
Although this pilot study was designed as a feasibility study, we also evaluated the efficacy of the Xbox KinectTM on motor and functional recovery of upper extremity. There were significant improvements in all efficacy outcomes in the experimental group. Previous studies had similar results (16–18). Because of the more intensive therapy in the experimental group, the efficacy results should be interpreted with care. The measured effect might indeed be related to the Xbox KinectTM games console training, or alternatively to the longer therapy session only. When reporting outcomes, it is important to consider that whether the amount of change between scores indicates a clinically significant difference (39). The observed 6.44-s benefit in the WMFT-PTS and 1.02-point benefit in the WMFT-FAS in the experimental group appears clinically meaningful according to a previous study, which reported the minimal clinically important differences for WMFT-PTS and WMFT-FAS as 1.5–2 s and 0.2–0.4 points, respectively (40). In the current study, training with the Xbox KinectTM provided a better improvement in the WMFT-FAS, but not the WMFT-PTS. This may be related to the statement that the WMFT-FAS appears to be more responsive to detect changes than the WMFT-PTS as suggested by the researchers in the previously mentioned study (40).
The present study has several limitations, mainly due to its pilot nature and the consequent tiny sample size. First, because a limited range of stroke survivors were recruited, these results should not be generalized to all patients after stroke. Secondly, longer total intervention time in the experimental group might have created a bias in favour of the game system. Finally, as a general limitation for all commercially available games consoles, both the Xbox KinectTM and the selected games have not been designed specifically for patients after stroke.
Training with the Xbox KinectTM is a feasible, safe and potentially effective intervention for the upper extremity in subacute stroke rehabilitation. As a promising new approach, it can be implemented as an adjuvant therapy to conventional neurorehabilitation practice. However, further studies are needed to confirm the efficacy and to reveal the long-term effects, the optimum duration and intensity of training. Finally, modifications could be made to this game system in order to extend the range of the targeted stroke survivors.
The authors thank the staff and patients at Ankara University Faculty of Medicine, Cebeci Research and Application Hospital, Physical Medicine and Rehabilitation Clinic. We also would like to offer our special thanks to Umut Kurban Coskun, PT, OT for her assistance with the training.
The authors declare no conflicts of interest.


 Click to show fullsize
Click to show fullsize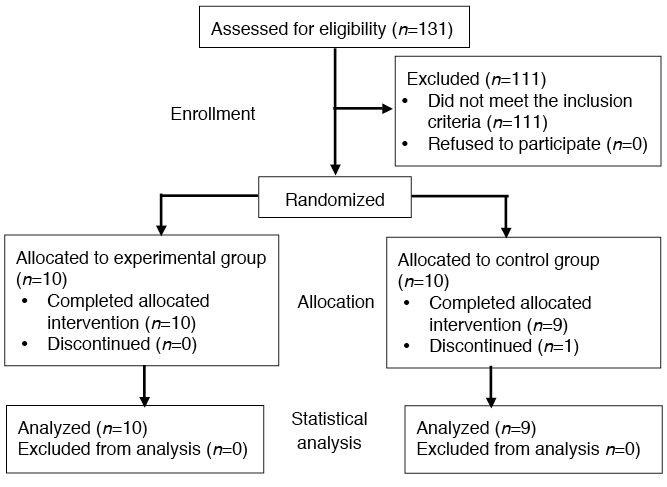 Click to show fullsize
Click to show fullsize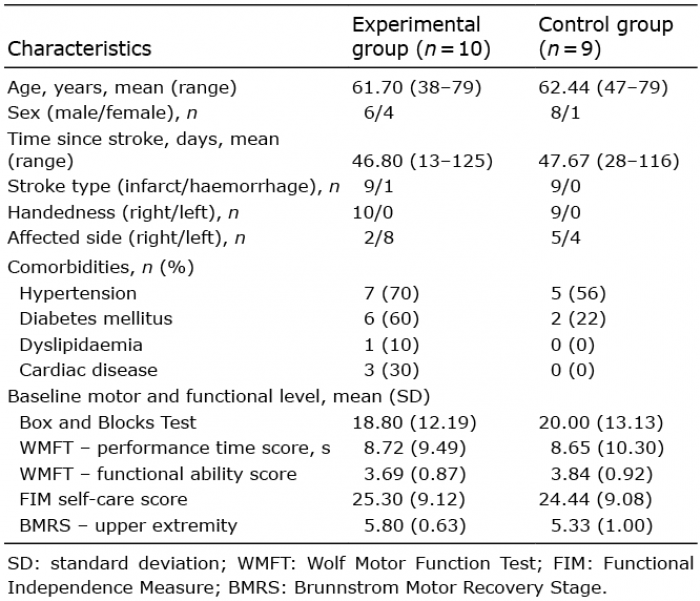 Click to show fullsize
Click to show fullsize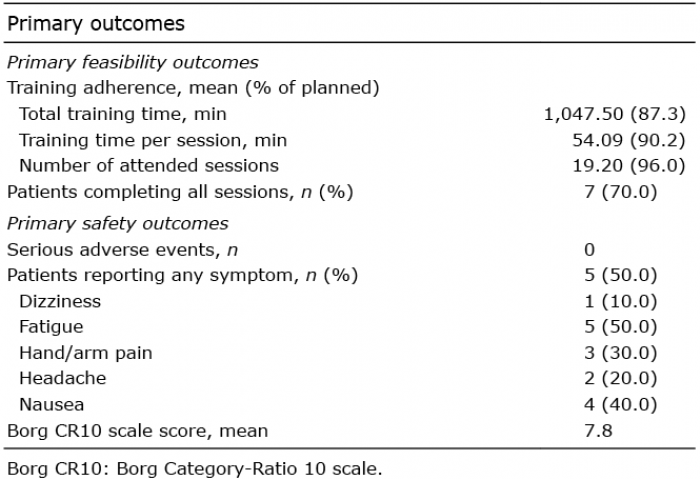 Click to show fullsize
Click to show fullsize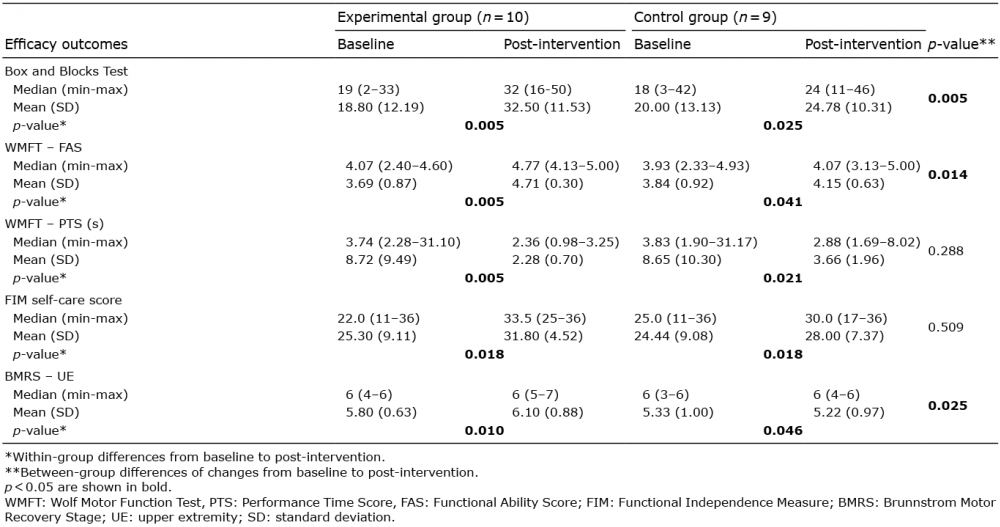 Click to show fullsize
Click to show fullsize