
From the 1Department of Health Sciences and the 2Department of Mathematics and Statistics, University of Jyväskylä, Jyväskylä, Finland
Objective: To determine the effectiveness of technology-based distance interventions for promoting physical activity, using systematic review and meta-analysis.
Methods: A literature search of studies published between 2000 and 2015 was conducted in the following databases: CENTRAL, EMBASE, Ovid MEDLINE, CINAHL, PsycINFO, OTseeker, WOS and PEDro. Studies were selected according to the PICOS framework, as follows: P (population): adults; I (intervention): technology-based distance intervention for promoting physical activity; C (comparison) similar distance intervention without technology, O (outcomes) physical activity; S (study design) randomized controlled trial. Physical activity outcomes were extracted and quality was assessed by 2 independent authors.
Results: Eight studies were included in the meta-analysis. The mean (standard deviation; range) me
thodological quality score of the studies was 6 (1.3; 4–8). Technology-based distance interventions were not more or less effective than conventional treatment whether measured as steps/day (mean difference 1,657; 95% confidence interval (95% CI) –1,861 to 5,176, p = 0.18), physical activity min/week (mean difference 0.34; 95% CI –146.3 to 146.9, p = 0.92), or as overall physical activity (response ratio 1.1; 95% CI 0.8–1.4, p = 0.65). No associations between the intervention duration or study quality and physical activity outcomes were found. Data were statistically and clinically heterogeneous.
Conclusion: The effectiveness of technology-based distance interventions for promoting physical activity is similar to that of conventional treatment.
Key words: technology; health promotion; rehabilitation; clinical trial; meta-analysis.
Accepted 23 Nov, 2016; Epub ahead of print Jan 23, 2017
J Rehabil Med 2017; 49: 97–105
Correspondence address: Tuulikki Sjögren, Department of Health Sciences, University of Jyväskylä, PO Box 35, FI-40014, Finland. E-mail: tuulikki.sjogren@jyu.fi
It is well documented that physical activity decreases the risk of several diseases (1) and physical inactivity, in turn, shortens life expectancy (2). At the societal level, inactivity imposes a heavy financial burden (3). It is therefore essential, at both individual and societal levels, to find ways to promote physical activity (1). The most effective method for achieving this objective remains unclear (4). Digitalization has given rise to the idea that physical activity could be promoted, among other means, through use of technology. This has led to increased interest in the potential of technological devices and applications as a component of distance rehabilitation interventions (5). In this systematic review, a distance intervention is defined as an intervention that is implemented in participants’ homes and or homelike conditions in their daily life, instead of via frequent face-to-face contacts. In distance rehabilitation, the participants play a very active role, performing self-contained rehabilitation without a healthcare professional being present. Distance interventions have emerged over the past few years, mainly owing to rapid technological development (6). The need to develop rehabilitation processes is driven by pressure on social and healthcare resources. Preventive interventions, especially, have occupied a minor role due to lack of resources; however, preventive care is a promising target and merits attention (7).
The technology that has been used in distance interventions to promote physical activity has included a broad range of software applications and services that can be used for collecting data and measuring and analysing physical activity performance (8). Examples of such distance technologies, which promote or motivate physical activity, are telephones, smartphones, computers, tablet computers, personal digital assistants, DVDs, videos, activity monitors and pedometers (9).
Evidence on the effectiveness of using technology to promote physical activity is conflicting (10–15). Telephone- (10), pedometer- (11) and internet-based interventions have been found promising compared with waitlist, placebo or minimal treatments. Insufficient information exists on the relative effectiveness of internet vs face-to-face interventions (12). Smartphone applications may be effective in increasing physical activity (13), although a systematic review with meta-analysis found the effect to be non-significant (14). Reviews have shown some degree of causality: the lighter the control treatment, the more the results seem to favour the intervention group. Overall, it is important to obtain statistically relevant, up-to-date and both scientifically and practically important information on the effect of technology-based distance promotion of physical activity.
To gain information about the effect of technology on increasing physical activity requires studies that are sufficiently comparable. The physical activity to be promoted should be the same in both the experimental and control groups, the only point of difference being the use of technology in the intervention (experimental) group. The objective of this systematic review and meta-analysis was to determine the effectiveness of technology-based distance interventions in promoting physical activity compared with similar interventions without the use of technology.
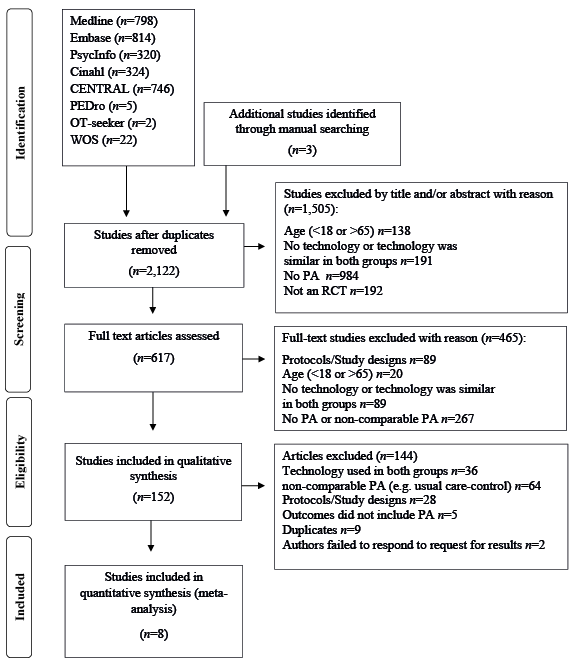
The following databases were searched from January 2000 to December 2015: Controlled Trials Register (CENTRAL), Excerpta Medica Database (Embase), The National Library of Medicine (Ovid MEDLINE), Cumulative Index to Nursing and Allied Health Literature (CINAHL), Psychological Information Database (PsycINFO), Occupational Therapy Systematic Evaluation of Evidence (OT-Seeker), Physiotherapy Evidence Database (PEDro) and Web of Science (WOS). Fig. 1 presents a flow chart of the study selection process. Two information specialists performed the data search using a wide range of terms on the topics of technology, physical activity and randomized or clinical trials. In addition, more comprehensive keywords describing physical activity interventions were used, e.g. exercise, exercise therapy, therapies, therapy modalities, rehabilitation, multidisciplinary therapy, motor activity, and participation. An example search strategy is shown in Appendix SI. A manual search for the literature using reference lists from the retrieved studies was also conducted.
Fig. 1. Search process flow chart.
Only studies investigating the effect of technology-based distance interventions in promoting physical activity were included in the review. The inclusion criteria, according to the PICOS framework (population, intervention, comparison, outcomes, study design), were as follows: P: adults aged 18–65 years; I: technology-based physical activity-promoting distance intervention; C: similar physical activity-promoting distance intervention as in the intervention group, but without technology; O: physical activity measured either subjectively (questionnaire, interview) or objectively (accelerometer, pedometer); S: randomized controlled trial. Studies published in English, Finnish, Swedish or German were eligible. To avoid developmental differences between the technologies used in the interventions as a result of recent advances in digitalization, only studies published in the 21st century were included.
Studies were screened independently by 2 authors (SH and AR) in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guidelines for systematic reviews (15). To achieve a consensus in the event of disagreement between the 2 screeners, a third reviewer (TS) also evaluated the study in question.
Methodological quality and risk of bias were assessed by 2 independent assessors (SH and AR), using the 12-point scale introduced in Guidelines for Systematic Reviews in the Cochrane Collaboration Back Review Group (16). All 12 items were rated as “yes”, “no” or “don’t know”. The main quality domains were assessed in the following sequences: A1: randomization; B2: concealed treatment allocation; C3: blinding of patients; C4: blinding of care providers; C5: blinding of outcome assessors; D6: drop-out rate; D7: analysis of participants in the groups to which they have been allocated; E8: selective outcome reporting; F9: similarity of groups at baseline; F10: similarity or absence of co-interventions; F11: compliance; and F12: timing of outcome assessments. A domain was considered “yes” and followed by a score, if the criterion was fulfilled. If it was not fulfilled, the domain was considered “no”, and if unclear “don’t know”. Neither the “no” nor “don’t know” conditions accrued scores. The overall quality of each included study was computed as the sum of “yes” scores out of theoretical maximum score of 12. The quality scores of the included studies are shown in Table I.
Data were extracted from the randomized controlled trials included in the studies following the recommendations of the Cochrane handbook for Systematic Reviews of Interventions Version 5.1.0, part 7.3.a (17). All the studies included in the qualitative analysis were accepted for the meta-analysis. Three meta-analyses were performed separately for each of the 3 physical activity outcome groups. The first analysis contained 3 studies, in which the number of steps/day was the outcome measure. The second analysis contained the other 5 studies, in which the duration of physical activity was the outcome measure. The mean difference (MD), i.e. the absolute difference in the mean values between 2 groups (17), was calculated in these 2 analyses. The third analysis comprised all 8 studies and thus included their different physical activity outcome variables. The fourth analysis, which included meta-regression for subgroups, focused on the health status of the participants, duration of the intervention and quality of the study. The outcome variables of the third and fourth analyses were expressed as response ratios (RR) calculated as the mean outcome of the intervention group divided by the mean outcome of the control group (18). The use of response ratios enabled the analysis of different combinations of the variables measuring physical activity. The meta-analysis model used the logarithm of the response ratio, and its variance was estimated by the approximation given in Borestein et al. (18). For interpretation purposes, the results of the meta-analyses were transformed back into response ratios by exponentiation. It should be noted that the boundary for significance in response ratios is 1 (not 0). The analysis did not take baseline values into account, owing to the inclusion criterion of a randomized controlled trial (RCT) design. Randomization decreases the systematic risk of the experimental and control groups differing at baseline with respect to the most important prognostic indicators.
A random effects model was used in the meta-analyses. The impact of the moderator variables was studied using a mixed effects model, also known as a meta-regression model. The models were estimated using restricted maximum likelihood (REML). The analysis was carried out in R with the metafor package (19). Knapp and Hartung adjustment was used to test the significance of the regression coefficients and form the confidence intervals (20). To examine statistical heterogeneity in the meta-analysis, both the Q statistic and I2 (21) were used along with a visual inspection of the forest plots. I2 describes the percentage of the total variation across studies that is due to heterogeneity rather than chance. An I2 of over 75% was interpreted as high heterogeneity and an I2 over 50% as moderate (22).
The search strategy identified 3,031 potentially relevant studies. After excluding 909 duplicates, 2,122 studies were assessed for eligibility based on their title and abstract. After further exclusions, 617 studies were assessed for eligibility based on their full text and 152 were included in the qualitative synthesis. Finally, a total of 8 studies fulfilled the inclusion criteria and were included in the meta-analysis (Fig. 1). The mean (standard deviation (SD)) methodological quality of the included studies was 6 (SD 1.3, range 4–8). The 2 quality assessors were in full agreement on the results. The method of randomization was adequate in all the included studies. In 2 studies (23, 24) the reasons for dropouts were not given. The most frequent source of bias was an inadequate or insufficiently reported blinding procedure and insufficiently reported compliance with the treatment.
Data were extracted for a total of 1,591 participants from 8 RCT studies. The mean number of participants was 199 (SD 208; range 32–655). The mean (SD; range) number of participants in the experimental group was 103 (SD 104; range 16–327) and in the control group 96 (105; 16–328). Females accounted for 46% of the participants in the experimental group and 47% in the control group. The mean age of the participants in the experimental and control groups combined was 47 (SD 7). Two studies comprised participants with cardiovascular diseases (25, 26) and 4 studies participants with obesity or a sedentary lifestyle (23, 27–29). In 2 studies, the participants’ health status was unspecified (i.e. participants were described as university staff (30) or men (24)). A detailed description of the studies included in the review is given in Table I.
The mean intervention duration was 4.5 (SD 4.3; range 0.25–12) months. The interventions also varied in content. Three studies (25–27) utilized supervised self-monitoring without feedback from caregivers or peer support. In Greene et al. (23), the intervention included a health-oriented online social network with peer support for accelerometer-based self-monitoring. Websites (23, 24, 30) enabled self-monitoring of physical activity behaviours, provided peer-support, or motivational messages. In one intervention, physical activity promotion was implemented via telephone with the support of a DVD (28). Only one intervention (29) was based wholly on phone calls, through which physical activity materials were obtained from a health educator. The content of physical activity was similar in both the intervention and control groups, except that instead of technology the control group received instructions on paper (23, 24, 29, 30) or in face-to-face meetings (25–28).
The most commonly used technology was a mobile phone. Two studies (28, 29) used phone calls to promote physical activity. In another 2 studies (24, 25), healthcare professionals used text message feedback with a computer or mobile phone without the possibility of participant response. Three studies used self-monitoring devices (i.e. accelerometer or pedometer) (25–27). A website was used as a medium in 3 studies (23, 25, 30). Combinations of technologies were used in 4 studies (24, 25, 28, 30), i.e. mobile phones and website, mobile phone as a feedback device and activity monitor, website and e-mails or mobile phone and DVD. Studies that used a smartphone application (24) or online social network (23) allowed participants to contact each other, thereby enabling peer-support. E-mail and text messaging (25, 30) was used as one-way communication from supervisor to participants.
Physical activity was measured using the same methods in the experimental and control groups. Four studies (25–28) used an accelerometer or activity monitor, except that in control group the screen was obscured. Four studies used self-reported questionnaires: Short Questionnaire to Assess Health (23), Active Australia Survey (24), International Physical Activity Questionnaire (30) and 7-day Physical Activity Recall (29). The outcomes are shown in detail in Table I.
The results for physical activity, measured as steps/day, and as either kcal/day, min/week, min/day or metabolic equivalent (MET) h/week are shown in Fig. 2. The results of a single study are shown in Table II.
Fig. 2. Forest plots describing: (A) physical activity steps/day, (B) physical activity min/week, and (C) response ratio of overall physical activity (measured either as steps/day, min/week or metabolic equivalent (MET)-min/week).
Table II. Main results of the studies included in the meta-analysis
Compared with the control interventions, the participants in the technology-based distance intervention performed, a mean of 1,657 more steps/day; however, the effect was not statistically significant (MD 1,657.4; 95% CI –1,861.5 to 5,176.2, p = 0.18). The homogeneity test indicated heterogeneity of the studies included in the analyses of steps/day (Q = 8.23, p = 0.016). The I2 value also indicated moderate heterogeneity (I2 = 72.64%).
In addition, the technology-based distance interventions did not increase physical activity duration, measured as min/week compared with the control interventions (MD 0.34; 95% CI –146.3–146.9, p = 0.92). The homogeneity test indicated heterogeneity of the studies included in the analyses of physical activity min/week (Q = 14.9631, p = 0.0048). The I2 value also indicated moderate heterogeneity (I2 = 74.72%).
Similarly, the technology-based physical activity-promoting distance interventions had no increasing effect on overall physical activity (i.e. MET h/day, kcal/day or min/week), compared with the control intervention (RR 1.06; 95% CI 0.8–1.4, p = 0.65). The homogeneity test indicated heterogeneity of the studies included in the overall physical activity analyses (Q = 27.82, p < 0.001). The I2 value indicated high heterogeneity (I2 = 86.26%).
Study quality had no effect on physical activity (RR 0.91; 95% CI 0.7–1.2, p = 0.96). When used for rehabilitation, the technology-based distance intervention was not more effective in increasing physical activity than when used for prevention (RR 1.5; 95% CI 0.9–2.5). No association was observed between the duration of the intervention and changes in physical activity when the technology-based distance intervention was compared with the control intervention (RR 0.95; 95% CI 0.9–1.0, p = 0.12). The homogeneity test indicated heterogeneity of the studies included in the covariate analysis of the intervention duration (Q = 22.04, p = 0.0012). The I2 value also indicated high heterogeneity (I2 = 82.47%).
This systematic review found that the use of technology in promoting physical activity was as effective as similar conventional promotions in which technology was not used. These findings indicate that a technology-based distance intervention has potential for increasing motivation providing counselling, and facilitating communication between healthcare professionals and patients. However, the cost-effectiveness of technology-based distance interventions should first be proven before their adoption in rehabilitation or healthcare settings.
The results of this meta-analysis do not allow firm conclusions to be drawn on the differences between these 2 types of physical activity-promoting interventions. This systematic review focused strictly on examining the effect of technology in distance use, and to our knowledge no similar systematic review yet exists. We included all the technologies that were used in the selected distance interventions to gain an overall picture of whether digitalization has benefits when used as a tool in healthcare or rehabilitation. To be included in the review, control interventions were not permitted to utilize any forms of technological mediation, including phone calls or self-monitoring devices. This review was strictly limited to study settings that compared 2 similar physical activity-promoting interventions, 1 of which (experimental) used technology, while the other (control) did not. In addition, the physical activity outcomes were required to be measured in the same way in the experimental and control groups.
Clinical heterogeneity between studies, such as differences between the participants (i.e. health status), differences in the content or technologies used in the interventions, and differences in the physical activity outcome measures, could affect application of the findings in clinical practice. Statistical heterogeneity was also present across all analyses. Despite this heterogeneity, the meta-analysis contained a total of 1,592 participants, which permits some general conclusions to be drawn.
The technology-based distance interventions showed a mean of 1,657 more steps/day than the control interventions (mean steps/day 7,221 and 5,687, respectively). Tudor-Locke & Bassett (31) categorized 5,000–7,499 steps/day as “low activity”, and 7,500–9,999 steps/day as “somewhat active”. Following this categorization, the technology-based distance intervention, while close to the threshold of somewhat active, remained within the low active category. For life expectancy, our findings are clinically meaningful, as it has previously been found that taking over 5,550 steps/day reduces all-cause mortality by 9% (32). Previous studies have also shown that 7,000–10,000 steps/day is the equivalent of 30 min of daily moderate-to-vigorous physical activity (33), which is enough to gain substantial health benefits (34). Based on the low number (i.e. 3 studies) and heterogeneity (i.e. duration and content of the interventions, diagnosis and age of the participants) of the studies investigating steps/day, our study may not have yielded robust clinically meaningful findings.
This systematic review found no association between the methodological quality of a study and its results. The relationships between methodological quality and outcome have been investigated in only a few physical activity reviews (34, 35). Young et al. (35) found that higher methodological quality explained more of the variance in physical activity, while Baxter et al. (36) found a relationship between high methodological quality and the cost-effectiveness of workplace health promotion programmes. It should be noted that quality scores do not take into account differences in the intervention content between the experimental and control group. The fact that in our study methodical quality was not related to the results may be explained by the similarity of the intervention treatments and/or low range of the quality scores. However, it has been reported previously that poor methodological quality, particularly in studies with inadequate blinding, is related to bias (37). In the present review, the most frequent source of bias was a poorly designed or insufficiently reported blinding procedure and insufficiently reported compliance with treatment.
In this review, technology included software, applications or devices that are suitable for outpatient interventions and can be used in distance rehabilitation. Physical activity-promoting technology can be roughly divided into 3 categories: electronic gauges or devices, telephones and mass media. Electronic gauges or devices are different from the other 2 categories as they only enable the measuring and self-monitoring of physical activity, whereas telephones and mass media can be used as mediating devices, which also allows feedback from a caregiver and peer support (38). The technology-mediated distance interventions in this meta-analysis delivered the treatment protocol via mobile phones, e-mails, text messages or websites (23, 24, 28, 29, 30). The electronic gauges used for self-monitoring were accelerometers and pedometers, and a self-monitoring approach was also present in the use of web-based exercise logs (23, 25–27). Peer-support was usually facilitated via web-based software or online social networks (23, 24). The results of the study by Greene et al. (23) indicate that the combination of an electronic gauge or device and a peer-support enabling platform can be as effective in promoting physical activity as a paper-based intervention. The use of a peer support-enabling website (24) or electronic gauges or devices (25, 27) also yielded positive results. However, the meta-analysis did not find the technology-based distance interventions more effective than the control interventions.
The participants in the studies included in this review were either healthy or diagnosed adults. Obese and sedentary participants were considered healthy, in the absence of a medical diagnosis as a reason for of their participation in the intervention. In 2 studies (25, 26), the intervention was targeted to patients with haemophilia and cardiovascular diseases, and obtained positive results using solely electronic gauges or devices, without peer support. These results suggest that the effect of technology in increasing physical activity and the cost-effectiveness of technology-based distance interventions for diagnosed patients should be investigated further. Technology may also make it possible to develop preventive care in the face of constraints on resources, as preventive interventions have been effective, for example, in reducing cardiovascular risk by encouraging patients to adopt a more active lifestyle (7).
The major concern in this review was the lack of research on the effect of physical activity-promoting technology in comparable settings. Insufficient data have also previously complicated the implementation of systematic reviews (39). Previous reviews (10–14) have compared technology-based interventions with other-treatment or waitlist control groups, which may have resulted in additional confounding factors masking the benefits obtained from the use of technology, while at the same time the interventions have differed in their physical activity content. This systematic review applied strict inclusion criteria: the physical activity treatment in both the intervention and control groups had to be similar, and no technology was to have been used in the control group setting; this meant that many studies were excluded. Technology was accepted as a component of the control intervention only in cases where physical activity was measured with an obscured screen. We also highlighted physical activity as the primary content of the intervention. The decision to restrict the review to studies where the physical activity promotion content was similar for both the experimental and control groups, was taken in response to the fact that effective ways of promoting physical activity have not been sufficiently investigated, and therefore, despite its limitations, this study design was reasonable.
Valid measurement of physical activity is challenging (40). The outcomes of the studies included in this review were measured both objectively (25–27, 28) and/or subjectively (23, 24, 29, 30). The outcomes most often used were moderate to vigorous physical activity, measured as min/week, METh, steps/day and energy expenditure (kcal/kg)/day. Other differences between the studies were the duration of the intervention and differing intensities of physical activity. The wide variation in the technology used also increased the heterogeneity of the interventions, further complicating comparison between studies. Statistical analysis confirmed that the heterogeneity of the included studies was significant. In addition, 2 studies (41, 42) were excluded owing to missing data of relevance to the meta-analysis. It is possible that this has influenced our results.
Physical activity should be measured with a valid and objective method using an accelerometer, a pedometer or some other activity monitor. Physical activity outcomes should be reported separately with both baseline and final outcome measures instead of only reporting changes between baseline and final measures. To improve the quality of RCT studies, and to demonstrate the absence of selective reporting, future studies should publish the protocol used, try to blind at least the outcome assessors and report compliance with the intervention. Another important factor to consider is cost-effectiveness, which has not generally been investigated in the domain of technology and physical activity.
Research using different physical activity devices, such as activity monitors or mobile applications, has increased along with the rapid advances in technology. Data therefore need to be constantly updated to enable comparison of the effectiveness of different features between products. However, while valid information on the effect of technology requires studies with comparable settings, is also important to learn whether a specific technology is more effective or acceptable in usual care or in a rehabilitation setting. Future studies should compare the effectiveness of different technologies according to their features, such as interactivity.
In conclusion, insufficient evidence has been adduced to draw firm conclusions on the differences between the effect of technology-based physical activity-promoting distance interventions and interventions similar in content, but administered using paper or face-to-face counselling. However, the results suggest that the differences, if any, are likely to be small. Our findings indicate that technology was approximately as effective as similar care without the use of technology. Thus, technology-based interventions have development potential as an alternative to conventional care. Before recommendations on the use of technology can confidently be made, additional studies, particularly on cost-effectiveness, are required.
The main strength of this systematic review is the restriction to studies in which the target physical activity to be promoted was sufficiently similar between the intervention and control intervention groups to capture the effect of the distant use of technology on increasing physical activity. Another strength is the use of carefully implemented statistical analysis. The search process was comprehensive and included all the essential databases. The search process also followed the guidelines of the Cochrane Handbook for Systematic Review of Interventions (17) and included quality assessments. The primary limitation of this systematic review is the low number of studies that could be included in it, which may have affected the overall variance of the meta-regression results. Nevertheless, the meta-analysis was justifiable given the overall large number of participants. The data were also both statistically and clinically heterogeneous. Clinical heterogeneity was observed between participants (i.e. health status), the interventions studied, the technologies used and the diversity of the physical activity outcomes measured.
The study has been financially supported by the Social Insurance Institution of Finland. The authors declare no financial relationships with any organizations that might have an interest in the submitted work in the previous 3 years; and no other relationships or activities that could appear to have influenced the submitted work. The study sponsor did not have any role in the study design, collection, analysis or interpretation of data, in the writing of the report, or in the decision to submit the report for publication. No financial disclosures were reported by the authors of this paper.


 Click to show fullsize
Click to show fullsize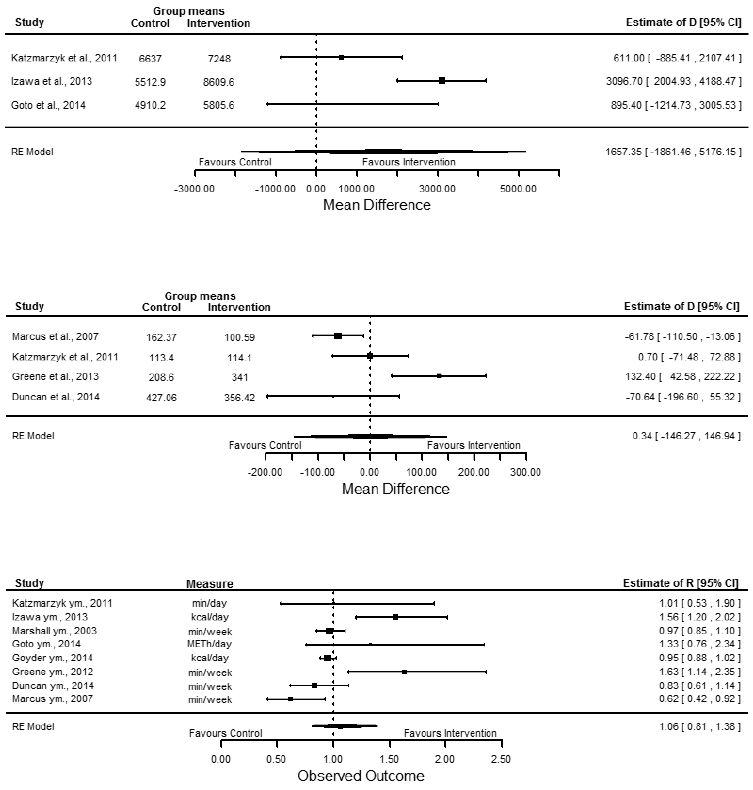 Click to show fullsize
Click to show fullsize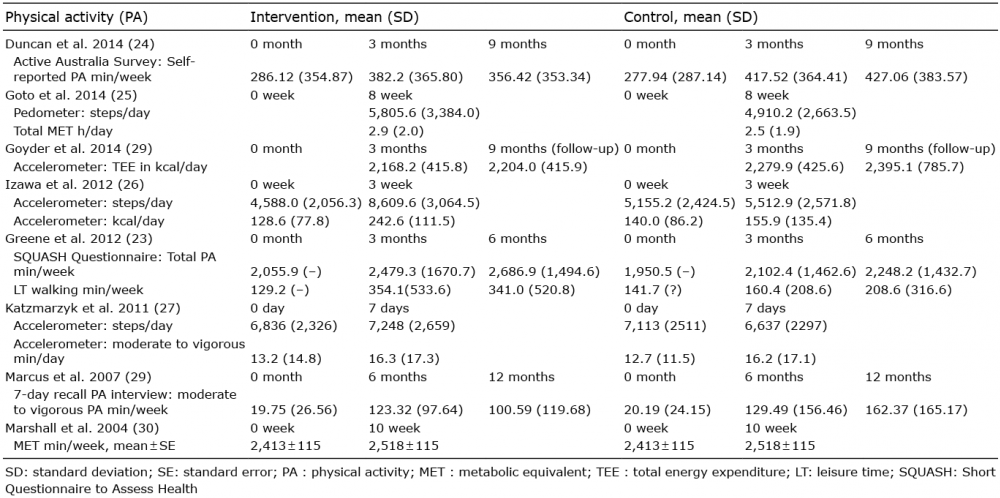 Click to show fullsize
Click to show fullsize