
From the 1Department of Rehabilitation Medicine, Royal Melbourne Hospital, Parkville, Victoria, Australia, 2Department of Medicine (Royal Melbourne Hospital) The University of Melbourne, Parkville, 3Australian Rehabilitation Research Centre, Royal Melbourne Hospital, Parkville, 4School of Public Health and Preventive Medicine, Monash University, Victoria, Australia and 5Department of Rehabilitation Medicine, First Affiliated Hospital of Nanjing Medical University, Nanjing, China
With increasing frequency of natural disasters, there has been greater focus recently on the importance and role of rehabilitation services in disaster management. In past disasters, rehabilitative needs were often neglected, with emphasis on acute response plans focused on saving lives and treating acute injuries. There was a lack of, or inadequate, rehabilitation-inclusive disaster response plans and rehabilitation services in many disaster-prone developing countries. The World Health Organization (WHO) Emergency Medical Team (EMT) initiative recognizes rehabilitation as an integral part of medical response and patient-centred care in disaster settings. Current developments under this initiative include: the development of minimum standards for rehabilitation in emergencies to allow rapid, professional, coordinated medical response by both national and international EMTs. These guidelines ensure that EMTs deliver effective and coordinated patient care during disasters and continuum of care beyond their departure. The aim is to strengthen national capacity, foster an environment of self-empowerment of EMTs and local health services, and work in rehabilitation within defined coordination mechanisms in disaster-affected areas. A brief overview of rehabilitation in natural disasters, highlighting current developments, challenges; and gaps in the implementation of WHO guidelines for Minimum Standards for Rehabilitation in Emergencies is discussed in order to improve care for victims of future disasters.
Key words: natural disaster; rehabilitation; emergency medical team; disability; disaster response.
Accepted May 11, 2017; Epub ahead of print Jun 30, 2017
J Rehabil Med 2017; 49: 00–00
Correspondence address: Bhasker Amatya, Department of Rehabilitation Medicine, Royal Melbourne Hospital, 34–54 Poplar Road Parkville, Melbourne VIC 3052, Australia. E-mail: bhasker.amatya@mh.org.au
Natural disasters (e.g. earthquakes, storms, drought, floods) often occur unexpectedly, precipitously and with great magnitude of destruction, resulting in mass casualties. As the frequency and amplitude of natural disasters has increased worldwide, human exposure to disaster risk is likewise escalating, mainly due to the combined effects of climate change, population growth, urbanization and poorly planned infrastructure and development (1). Recent advances in disaster response/rescue and field management, have significantly improved the survival rates of disaster victims worldwide. Current disaster data demonstrates a staggering number of persons with injuries relative to mortality (2, 3). This includes an upsurge in survivors with complex and long-term disabling injuries, such as brain and spinal cord injury, peripheral nerve and musculoskeletal injuries. Furthermore, there may be an increase in the number of victims with exacerbation of chronic medical conditions and psychological impairment. These problems necessitate comprehensive long-term interdisciplinary management, including rehabilitation (3, 4).
Medical rehabilitation is defined as: “a set of measures that assist individuals who experience (or are likely to experience) disability to achieve and maintain optimal physical, sensory, intellectual, psychological and social functioning in interaction with their environment” (5). Overall primary goals of medical rehabilitation include management of acute injury, prevention and management of related complications, optimization of functional capabilities (including physical, cognitive, neuropsychological functioning) and social re-integration (6). These goals are not different in disaster settings; however, they can be more complex and challenging, and may include: assessment of injury patterns and management, needs and resource requirements (including long-term); establishment of patient triage, discharge, referral, and tracking systems; collaboration with other healthcare service providers; coordination with emergency response systems, host health system and government managers; education of local healthcare providers and data collection/management (2, 6). The team is interdisciplinary and includes physical and rehabilitation medicine physicians, nurses and allied health professionals.
With increasing frequency of natural disasters and numbers of people injured, the critical importance of rehabilitation services for the survivors during and after a natural disaster is well-documented (3). There is still scarce research and a lack of robust, methodologically strong innervational studies in this area, and current evidence is based mainly on observational studies, personal and anecdotal experiences (3, 6). Evidence suggests that early provision of rehabilitation programmes reduces disability, leading to better clinical outcomes, and improved participation and quality of life for disaster survivors (3, 6, 7). Disaster survivors treated in services with rehabilitation facilities have reduced length of hospital stay, fewer complications and better clinical outcomes compared with patients in centres with no rehabilitation physician supervision (2). The significant roles of allied health professionals, such as occupational therapy, physiotherapists in disaster preparedness, response, and recovery, are well documented (8–10). There is strong consensus amongst global health authorities that medical rehabilitation should be initiated in the immediate emergency response phase and should be continued in the community over a longer term until treatment goals are achieved and survivors are successfully reintegrated into society (3, 6, 11). The World Health Organization (WHO) rehabilitation guidelines recommend implementation and access to rehabilitation during all phases of disaster response, and pinpoint rehabilitation as the longest and most expensive phase of disaster management (12, 13).
In recent years, many countries have recognized the importance of disaster planning, preparedness and management initiatives, and disaster management capacity (especially early warning systems, early evacuation and awareness) with improved collaboration (11). Unfortunately, major disparities and gaps amongst countries exist, and those with a high disaster-risk tend to have low coping capacity and a large population vulnerable to natural disasters living in more exposed areas (14, 15). Disaster response plans and services are generally inadequate or absent in many disaster-prone countries (16, 17), and few have access to appropriate services, such as rehabilitation, where fragmented healthcare systems are compromised by lack of financial and political support (7, 18). In large-scale disasters, existing local health service infrastructure and resources can be destroyed/severely disrupted and/or quickly overwhelmed by an influx of disaster victims, compromising the medical response and optimal management (6, 16). Furthermore, a shortage of, or lack of, trained healthcare (including rehabilitation) professionals and medical workforce can further hinder comprehensive management (18, 19). Hence, in disasters many countries are dependent on global humanitarian and medical assistance. This is reflected by the growing number of Emergency Medical Teams (EMTs) responding to many disasters worldwide (20). However, influx of EMTs during past disasters has presented immense challenges with regards to response coordination, management and evaluation. Furthermore, in many past disasters, deployment of medical teams has been decided by the individual countries or organizations, and on many occasions these teams worked on their own, with no accreditation and/or coordination mechanism. Deployment of these teams was not always based on the needs of the situation; and there was significant variation in capacities, competencies and professional ethics (21). This resulted in significant challenges and inadequate care delivery, particularly rehabilitation, with often devastating consequences for the affected individuals, families and communities (2, 6, 20). Furthermore, there is concern regarding the inadequacy of global organizational capacities and capabilities and mismatching of resources across the entire disaster cycle, such that prevention and preparedness have been consistently short-changed (12). For example, during the earthquake in Haiti in January 2010, the international humanitarian response was catastrophic, with the influx of a large number of EMTs, many unregistered, without standardized protocols, or coordination mechanisms in place (21, 22). There was poor coordination and communication, particularly between service providers including EMTs, with suboptimal adherence to national and/or international standards, which resulted in unsatisfactory outcomes (22–24). One study (17) showed significant proportion of deaths occurred days or weeks after the Haiti earthquake could have been prevented by improved patient care. Likewise, during the 2004 Indian Ocean tsunami the number of EMTs that arrived exceeded what was needed given the rapid mobilization of trauma teams from within the countries (21).
In the last decade, significant developments in international, regional and national collaboration and management capacities in disaster management have occurred, including quality and coordination mechanism of EMTs. Some key developments are discussed below:
1. The United Nations (UN) Office for Disaster Risk Reduction (UNISDR) leads the global response for international humanitarian crises. It initiates different programmes to improve community resilience and coordination of disaster-risk reduction activities worldwide. Following the 2004 Indian Ocean tsunami, under the leadership of UNISDR the Hyogo Framework for Action 2005–2015: Building the Resilience of Nations and Communities to Disasters, the first comprehensive global blueprint for disaster risk reduction, was adapted by representatives of 168 member states at the World Conference on Disaster Risk Reduction in Kobe, Japan, in 2005 (25). Over the last 10 years, although voluntary and non-binding, the Hyogo framework has been embraced by central and local governments, the private sector and civil society groups (25). Under this initiative, significant global progress has occurred in disaster risk management, including raising awareness, promoting prevention, preparedness and mitigation (26). As of 2015, there were Hyogo framework focal points in 191 countries and 85 platforms for disaster-risk reduction, and 141 countries have carried out at least 1 review of their efforts to implement this framework for action through advances in risk governance, stronger institutions, education and science, and addressing underlying drivers of risk and strengthening preparedness and response mechanisms (25).
2. More recently, the third UNISDR World Conference in Sendai Japan (2015) adopted a new 15-year global framework for disaster risk reduction, the Sendai Framework for Disaster Risk Reduction 2015–2030 (SFDRR) (Table I) (27). The SFDRR is built on elements that ensure continuity with the work done by states and other stakeholders under the Hyogo framework and introduces a number of innovations. It emphasizes disaster-risk management as opposed to disaster management. It broadens disaster-risk reduction significantly to focus on both natural and man-made hazards and related environmental, technological and biological hazards and risks (27). It provides a strong foundation for governments to take on a greater role at all levels and an agenda for all sectors of society for collaborative effort for successful future disaster planning and management (27). The SFDRR, specified “rehabilitation” as a component of 1 of the key priorities (Priority 4, Table I) (27). The term “rehabilitation”, however, is more inclined towards the rehabilitation infrastructure processes, rather than medical rehabilitative care of patients. Unfortunately, in this document, the medical rehabilitation of victims and the establishment of emergency relief and healthcare stakeholders for disaster management (including EMTs) are rarely mentioned. This highlights the low priority attributed to medical rehabilitation services in disaster settings, not only by many developing countries, where rehabilitation services are underdeveloped, but also by developed countries with a strong medical rehabilitation workforce (28). Similar to the “Hyogo Framework”, the “Sendai Framework” is also voluntary commitment of member states and depends on the capacity and willingness of countries to take concrete action (17, 29).
Table I. Sendai Framework for Disaster Risk Reduction 2015–2030. Adapted from: UNISDR 2015 (27)
3. The World Bank’s Global Facility for Disaster Reduction and Recovery (GFDRR) is another key initiative committed to assisting developing countries to reduce their vulnerability to natural hazards, with a global partnership of over 45 countries and international organizations (30). This initiative conducts post-disaster needs assessments worldwide and supports national governments in recovery and reconstruction, to reduce the costs of future disasters. It implements programmes in partnership with national, regional and other international agencies, in accordance with the SFDRR, the Paris Agreement on Climate Change, and the UN Sustainable Development Goals (30). The GFDRR programme, including rehabilitation and reconstruction, aligns with the SFDRR priorities and disaster-risk management activities identified as priorities by communities; however, there are no details of programmes focused on building capacity in rehabilitation medicine in its work plan for 2017 (31).
4. Emergency Medical Team (EMT) Initiative. Lessons from past disasters highlight the need for better coordination and cooperation, and evaluation of professionalism and accountability of national and international disaster responders. This prompted the global community of international medical responders to work towards the establishment of the Foreign Medical Teams (now termed EMTs) Working Group (FMT-WG) in a post-Haiti meeting in Cuba in 2010. This resolution recommended “a flexible mechanism for registration and accreditation of rapid-response foreign medical teams with the goal of improving the quality of medical response in coordination with WHO”, which was passed at the Pan American Health Organisation (PAHO) in 2012 (21). This is the precursor of the current WHO EMT unit and initiative. This EMT programme has demonstrated a more systematic approach to medical team deployment and organized deployment responses to recent natural disasters, such as typhoon Haiyan in the Philippines in 2013, tropical cyclone Pam in the Pacific region in 2015 and the Nepal earthquakes in 2015 (22). The first guideline, the Classification and Minimum Standards for Foreign Medical Teams in sudden onset disasters, was published in September 2013 (24). The EMT Initiative comprises 11 working groups, including a rehabilitation group. This guideline provided the benchmark requirements for medical teams seeking to respond to emergencies and coordinating their deployment by classifying teams according to their capability (24). Table II lists the types of EMTs.
Table II. World Health Organization (WHO) classification of Emergency Medical Teams (EMTs). Adapted from WHO 2016 (20)
5. WHO global registration process of EMTs. A new WHO registration system for all EMTs was initiated in July 2015 (Fig. 1), which enables establishment of a global register of emergency medical response teams for deployment in emergencies (22). As of 2016, 4 acute medical teams (from Australia, China, Israel, Japan and the Russian Federation) have progressed to full verification and 75 teams from different part of the world have commenced a mentorship process and seeking quality assurance (22). By the end of 2017, an expected 50 additional teams will have been verified for quality assurance, and over 100 will be in the mentorship programme (22). However, currently no Rehabilitation specialized cells are included in this list.
Fig. 1. Global Emergency Medical Team (EMT) classification process. Adapted from World Health Organization (WHO) EMT initiative (22).
6. Rehabilitation guidelines for disasters.As aforementioned, the WHO EMT initiative acknowledges rehabilitation as an integral aspect of medical response and patient-centred care in disaster settings in the guidelines: Classification and Minimum Standards for Foreign Medical Teams in Sudden Onset Disasters (24). It recognizes that “rehabilitation is one of the core functions of trauma care systems in regular health care and, as such, EMTs should have specific plans for the provision of rehabilitation services to their patients post sudden onset disaster” (20, 24). The guidelines emphasize importance of early rehabilitation for positive functional outcomes by ensuring a rapid, professional, coordinated medical response that includes rehabilitation professionals by both national and international teams (20). Reports from past emergency responses demonstrated a lack of integration of rehabilitation professionals into EMTs and lack of coordination with other EMT members (surgical and medical), which detract from patient-centred care (20). This prompted the Rehabilitation Working Group under the EMT initiative, to develop the first guideline for rehabilitation teams in sudden onset disasters: “Emergency Medical Teams: Minimum Technical Standards and Recommendations for Rehabilitation”. This guideline, launched at the EMT Global Meeting 2016 in Hong Kong, was developed with collaboration between WHO and global experts from the rehabilitation field including the International Society of Physical and Rehabilitation Medicine (ISPRM) (20). It sets out the core standards for rehabilitation and provides guidance on building or strengthening the capacity of EMTs for rehabilitation within defined coordination mechanisms in this area. The recommendations require that both national and international EMTs must ensure improved patient care and a continuum of care beyond their departure from the affected area. The guidelines provide the minimum standards for all EMTs regarding workforce, field hospital environment, rehabilitation equipment/consumables and information management. The key standards for EMTs within these guidelines are listed in Box 1.
Box 1. Key minimum standards for EMTs. Source: WHO 2016 (20).
All teams on the WHO EMT Global Classification List will now be required to use these minimum technical standards for rehabilitation in the future, and demonstrate adherence to standards (20). Table III provides an overview of rehabilitation input by EMT type, and specific discharge considerations.
Table III. Overview of rehabilitation input by Emergency Medical Team (EMT) type. Adapted from WHO 2016 (20)
The minimum standards for rehabilitation clearly set out the standards for rehabilitation and provide guidance on strengthening EMT capacity. However, they are yet to be implemented and, to our knowledge, many specialized teams (such as rehabilitation) are yet to receive any mentorship, or to be considered for full verification at this time. There are still immense challenges in putting these standards into practice in disaster settings, these include:
There is a clear mandate for all EMTs (including rehabilitation) to act quickly, efficiently and effectively during disasters (24). There is also strong consensus amongst disaster relief professionals that rehabilitation is an integral component of disaster management and rehabilitation professionals can add considerable value to patient care during response, acute and post-disaster phases (3, 6, 16). Regrettably, although there have been significant improvements in the organization of emergency responses/care and services, this has often not extended to include rehabilitation services (2). The WHO EMT initiative, including publication of the rehabilitation guideline provides a paradigm shift in rehabilitation-inclusive disaster management, to deliver timely, cost-effective, patient-centred, coordinated and transparent services in future disasters (24). The successful implementation of a minimum standard framework will require increased resilience of the rehabilitation community with multi-stakeholder partnerships. There is still much progress to be made in tackling the underlying drivers of disaster risk, such as poverty, climate change, rapid urbanization; and factors such as poor local governance, population growth, economic development patterns, to establish rehabilitation-inclusive disaster management model for future catastrophes. Some perspectives need to be considered, including:
Medical rehabilitation of disaster victims is essential, not only to improve their functional capabilities (including cognitive, neuropsychological function), but also their activity and participation within contextual factors (personal and environmental) for social reintegration. Learning from past catastrophes, inclusion of rehabilitation in the global disaster response initiative is a significant development and improvement in this area. The WHO EMT initiative Rehabilitation Guidelines (20) provides structure and standardization, aligned with a set of overarching principles, to prepare, plan and provide clinical care during disasters for future deployments. However, there are many challenges in implementing these standards. Rehabilitation is the most expensive phase of any patient care, particularly for those with severe and multiple impairments requiring long-term care (13, 39). Sustained efforts from the WHO EMT Secretariat are needed to establish and maintain the EMT workforce (including rehabilitation) that possesses the knowledge, skill and ability to support all health-related aspects of disaster management (40). The role of the WHO Liaison Sub-Committee the Disaster Rehabilitation Committee (DRC) of the ISPRM, should be recognized in future disasters to facilitate coordination among major rehabilitation providers to minimize delay and duplication in deployment and deliver timely and effective rehabilitative care to victims. All countries prone to natural disasters should focus on planning and invest more in rehabilitation infrastructure and workforce. The challenge ahead is to develop a comprehensive, targeted and integrated rehabilitation-inclusive approach to disaster planning and management, targeting vulnerable communities at risk in future disasters. Future successful and effective disaster management will depend on the proficient leadership of the governing bodies (both international and national), and the willingness and commitment of countries to build systematic advance planning and preparedness to ensure that effective services (including rehabilitation) are available when needed.
This review was supported from internal resources of the Rehabilitation Department, Royal Melbourne Hospital, Royal Park Campus, Melbourne, Australia. The authors acknowledge the Disaster Rehabilitation Committee (DRC), of the International Society of Physical and Rehabilitation Medicine (ISPRM) and the WHO – Liaison Committee of the ISPRM. The views express in this article are not of the above-mentioned ISPRM committees.


 Click to show fullsize
Click to show fullsize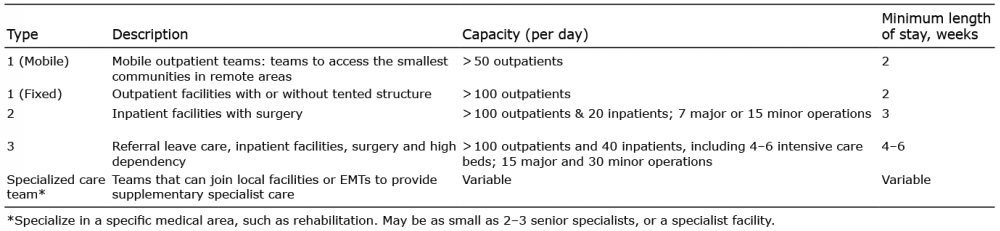 Click to show fullsize
Click to show fullsize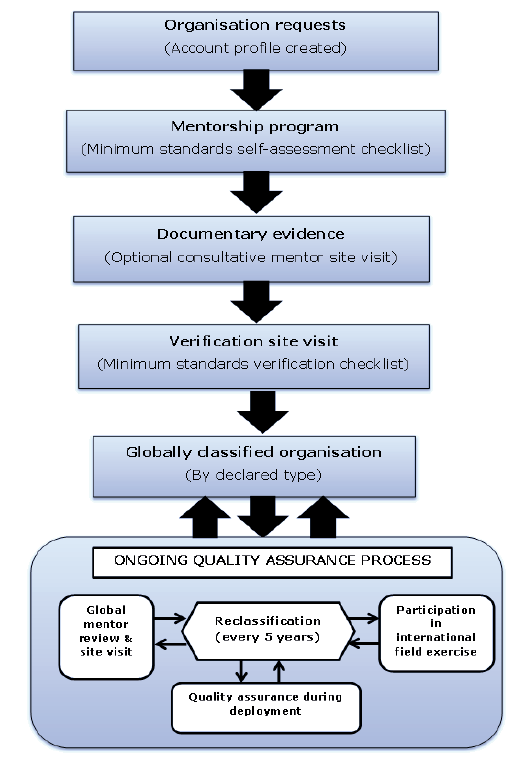 Click to show fullsize
Click to show fullsize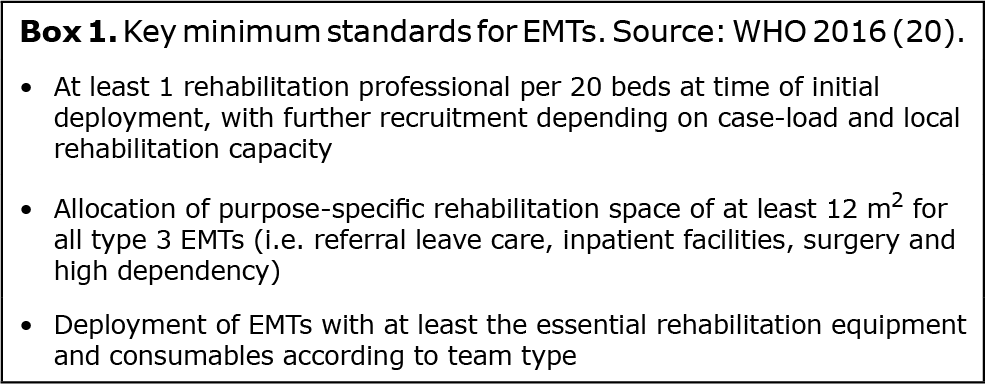 Click to show fullsize
Click to show fullsize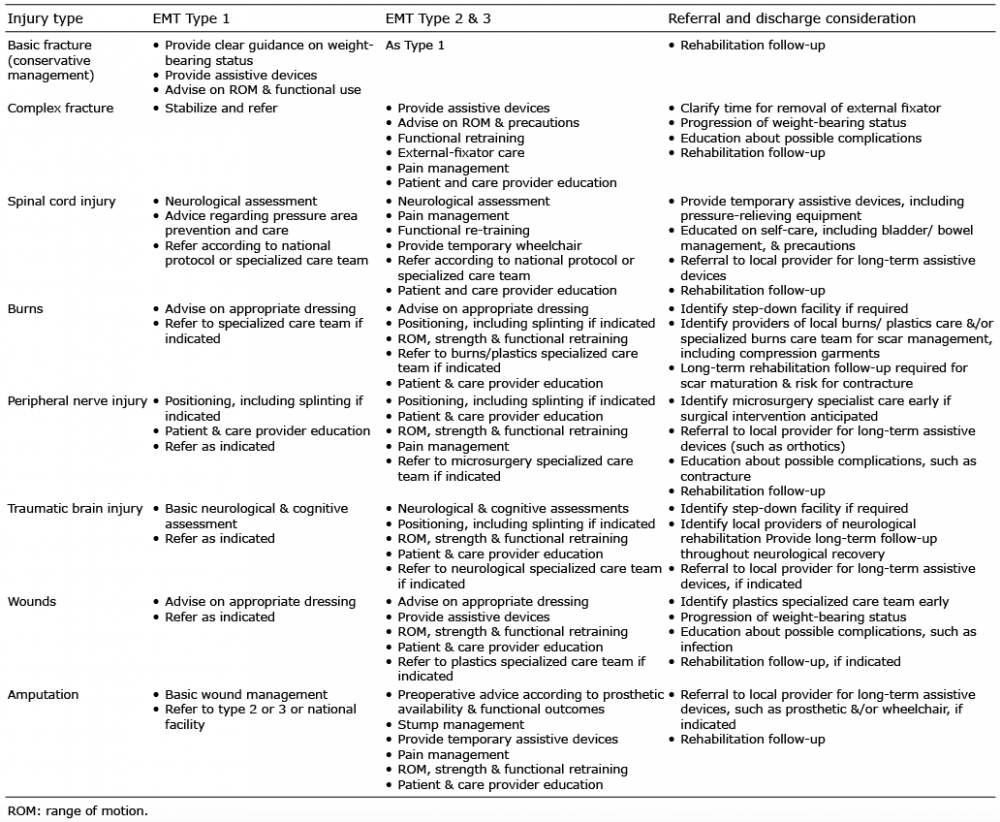 Click to show fullsize
Click to show fullsize