
From the 1UKK Institute for Health Promotion Research and 2Tampere University Hospital, Department of Physical and Rehabilitation Medicine, Tampere, Finland
Objective: To investigate associations of various bio-psychosocial factors with bodily pain, physical func-tioning, and ability to work in low back pain.
Design: Cross-sectional study.
Subjects: A total of 219 female healthcare workers with recurrent non-specific low back pain.
Methods: Associations between several physical and psychosocial factors and: (i) bodily pain, (ii) physical functioning and (iii) ability to work were studied. Variables with statistically significant associations (p < 0.05) in bivariate analysis were set within a generalized linear model to analyse their relationship with each dependent variable.
Results: In generalized linear model analysis, perceived work-induced lumbar exertion (p < 0.001), multi-site pain (p < 0.001) and work-related fear-avoidance beliefs (FAB-W) (p = 0.02) best explained bodily pain. Multi-site pain (p < 0.001), lumbar exertion (p = 0.005), FAB-W (p = 0.01) and physical performance in figure-of-eight running (p = 0.01) and modified push-ups (p = 0.05) best explained physical functioning; FAB-W (p < 0.001), lumbar exertion (p = 0.003), depression (p = 0.01) and recovery after work (p = 0.03) best explained work ability. In bivariate analysis lumbar exertion was associated with poor physical performance.
Conclusion: FAB-W and work-induced lumbar exertion were associated with levels of pain, physical functioning and ability to work. Poor physical performance capacity was associated with work-induced lumbar exertion. Interventions that aim to reduce fear-avoidance and increase fitness capacity might be beneficial.
Key words: low back pain; psychosocial factor; physical fitness; work ability.
Accepted Jun 7, 2017; Epub ahead of print Aug 9, 2017
J Rehabil Med 2017; 49: 00–00
Correspondence address: Annika Taulaniemi, The UKK Institute for Health Promotion Research, Kaupinpuistonkatu 1, FI-33500 Tampere, Finland. E-mail: annika.taulaniemi@uta.fi
Low back pain (LBP) is a bio-psychosocial, multidimensional, complex and costly problem, and is a leading cause of years lived with disability (1). In the majority of people with LBP (85–90%) the pain is classified as non-specific low back pain (NSLBP). Most people recover after an acute pain episode, but in 50–70% the pain recurs within the following year, and in 10% it becomes chronic (2). LBP is often a long-term or recurrent condition wherein individuals experience repeated episodes of pain that are not independent of each other (3), and the majority of people with LBP experience back pain off and on over an extended span of time (4, 5).
The prevalence of LBP varies among occupational groups. Workers in physically demanding jobs are known to have increased risk (6). Among healthcare workers, the 1-year prevalence of LBP is 45–77% (7), which is high in comparison with other occupations. Nursing duties include large amounts of heavy physical work and psychosocial stress, which are known to be risk factors for LBP (8). Among newly qualified female healthcare workers, those with a high physical workload had high risk (78%) of developing LBP (9). Nurses who are engaged in patient-handling also have high risk of chronic LBP (10).
Risk factors for chronic disability from LBP are more closely related to psychosocial factors than to spine condition itself (11). Fear-avoidance beliefs (FABs), job satisfaction, and anxiety are known to be associated with chronicity (12). The concept of FAB refers to the fear-induced avoidance of activities or movements that are expected to be painful. Among healthcare workers with previous LBP, FABs have been shown to be a major risk factor for new episodes of LBP (8).
On the other hand, there is also increasing evidence that low performance levels for several components of physical fitness are risk factors for LBP (13, 14), although scientific evidence about those associations is still partly conflicting with respect to revealing whether physical inactivity and deconditioning cause LBP or, alternatively, LBP leads to decreased physical activity and deconditioning (15). Women with LBP have lower levels of aerobic fitness than healthy women (16). Even self-reported low rating of physical capacity is a strong predictor for future LBP in female healthcare workers (17). Imbalance between physically demanding nursing duties and physical capacity, i.e. demonstrating relatively low strength, aerobic fitness and balance, increases the risk of LBP (17).
Preventing new episodes of LBP is considered to be important for the prevention of persistent pain. Thus, it is essential to understand links between several biological and psychosocial risk factors influencing the early stages of LBP, before chronicity, especially in a population performing physically demanding work.
The aim of this cross-sectional study was to investigate associations between several bio-psychosocial factors and: (i) bodily pain, (ii) physical functioning, and (iii) perceived ability to work in a sample of female healthcare workers with recurrent NSLBP. Furthermore, we examined the relationship between physical fitness and work-induced lumbar exertion among the study population.
This cross-sectional study was part of a randomized controlled trial (the NURSE RCT, clinical trial registration NCT01465698) aimed at reducing pain, movement-control impairment, and fear-avoidance beliefs in working female healthcare personnel with recurrent NSLBP. The study was approved by the Ethics Committee of Pirkanmaa Hospital District, Finland (ETL code R08157).
The target population was female healthcare personnel engaged in lifting and transferring patients and other tasks that are demanding for the lower back. To be eligible for the NURSE RCT, individuals had to meet the following criteria: (i) being a woman aged 30–55 years who (ii) had worked in her current job for at least 12 months, and (iii) experienced LBP of intensity 2 or above within the preceding 4 weeks, measured on the numeric rating scale (NRS; 0–10) (18). The exclusion criteria for the study were: (i) a serious earlier back injury (fracture, surgery, or disc protrusion), (ii) chronic LBP as diagnosed by a physician or self-reporting of continuous LBP over the past 7 months or longer, (iii) a serious other disease or symptoms limiting participation in moderate-intensity neuromuscular exercise, (iv) engaging in neuromuscular-type exercise more than once a week, and (v) pregnancy or recent delivery (< 12 months).
The NURSE- RCT was conducted in the form of 3 identical, consecutive sub-studies. The participants were workers in geriatric wards and old people’s homes (in the first sub-study in 2011, n = 56), in community hospital wards, public healthcare units, and home service (in the second sub-study in 2012; n=80) and in university-hospital wards (in the third sub-study in 2013; n = 83) in the city of Tampere, Finland. Data-sets from the baseline measurements in these sub-studies were combined and analysed in the study reported here. The total sample consisted of 219 healthcare workers. Information about the NURSE RCT was disseminated through information sessions for head nurses and other personnel, hand-outs, posters, and intranet posts. The sample size (at least 160 subjects) was estimated for the primary outcome of pain intensity in the RCT (19). More precise information on recruitment is available in the protocol article on the NURSE RCT (19). Fig. 1 summarizes the recruitment process.
The measurements were conducted at the UKK Institute for Health Promotion Research, in Tampere. Informed consent was obtained in writing from all participants on the first visit. Specially educated personnel with a long work history conducted all measurements. Health screening was performed before fitness testing, in accordance with the safety model of the Health-related Fitness Test Battery for Middle-aged Adults (20). The measurement battery, measured in a single 2-h session, consisted of questionnaires, assessment of physical fitness test results, and guidance in using the accelerometer for objectively measuring physical activity/sedentary time over one week.
1. Bodily pain interfering with normal work during the preceding 4 weeks was assessed by a sum score from 2 questions in the validated Finnish version (21) of the RAND-36 Health Survey (22), which measures quality of life in 8 distinct domains. For the bodily pain –domain, there is 1 rating on 5point-scale (intensity of bodily pain) and 1 6-point-scale rating (pain interfering with normal work). Respondent-reported scores were converted into scores ranging from 0 (very severe pain and extreme difficulties) to 100 (no pain and no difficulties) in accordance with the conversion equation presented by Ware & Sherbourne (23). The briefer expression “bodily pain” is used in this article to describe this measurement.
2. Current limitations in physical functioning (sum score from 10 questions from the Finnish version of the RAND-36 survey) (21). The item consists of 10 ratings (for vigorous activity, such as strenuous sport; moderate intensity activity, such as vacuuming or bowling; lifting and carrying groceries; climbing several flights of stairs; climbing 1 flight of stairs; bending, kneeling or stooping; walking approximately 2 km; walking approximately 500 m; walking 1 block; and bathing or dressing) on a 3-point scale (limited a lot, limited a little, not limited at all). The respondent-reported scores were converted into scores ranging from 0=limited a lot to 100 = not limited at all (23).
3. Work ability index (WAI), short form (24). Sum score from 4 questions, 3–27 scale (from 3 = poor to 27 = the best possible), cover current work ability (0–10; where 0 = unable to work and 10 = the best possible), work ability in relation to physical work demands (1–5; 1 = very poor, 5 = very good), and in relation to mental work demands (1–5; 1 = very poor, 5 = very good), and personal prognosis for work ability in 2 years’ time (1 = hardly able to work, 4 = ”not sure”, 7 = almost certain work ability).
1. Performance tests for physical fitness.
2. Physical activity.
3. Self-reported physical measures.
4. Self-reported psychosocial factors.
Depression. Beck Depression Inventory (BDI), short form (sum score from 9 questions with a 1–4 rating scale) (33), where high values indicate higher levels of depression.
Psychosocial factors at work (such as work stress) were assessed via a Finnish work satisfaction questionnaire (34). Those factors were used only for adjustments. Variables used for adjustments represented factors that might have an association with the outcome measurements, but that had no influence on later interventions (neuromuscular exercise and/or counselling) carried out in the NURSE-RCT.
For the descriptive analyses, the mean and standard deviation (SD), and medians (Md) and quartiles (Q1,Q3) were calculated. Identification of skewed distributions was performed through visual inspection of the histograms, by comparison of means and medians, and by calculation of skewness divided by standard error. Correlations between at least ordinal scale measurements were analysed via Spearman’s rank correlation coefficient (rs).
Associations between categorical variables and normally distributed continuous variables were analysed via 1-way analysis of variance (ANOVA) and independent-samples t-test. The corresponding statistical tests for non-normal distributions were the Kruskal–Wallis test and the Mann–Whitney test.
When statistically significant associations (p < 0.05) between bio-psychosocial factors and dependent variables were found in bivariate analysis, generalized linear models (GLMs) were used to determine which independent factors best explain the dependent variables: bodily pain, physical functioning, and work ability. After calculation of crude β-coefficients, the analyses were adjusted first for age, BMI, and work type (shift work/regular work), and subsequently also for sick leave due to LBP in the preceding 6 months, hormonal status and work satisfaction.
To enable comparison of the strength of associations between various covariates and dependent variables, standardized β values were calculated for continuous variables (by multiplying the crude β by the SD of the covariate, then dividing the result by the SD for the outcome measurement) (35).
All analyses were conducted with the SPSS statistical analysis package, version 22.
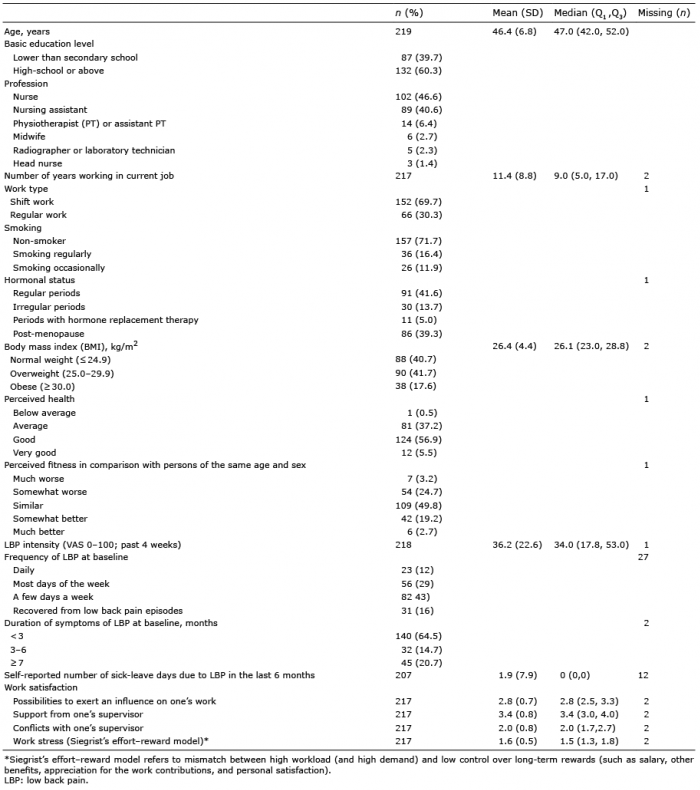
Baseline characteristics of the study sample are reported in Table I. The study subjects had worked in their current position in a mean of 11.4 years. More than 85% of them were nurses or nursing assistants, and 70% had irregular working hours. Most perceived their health to be average or good, but 28% perceived their fitness to be poor in comparison with that of persons of the same age and sex. Only approximately 40% were of normal body weight, and 60% were considered to be overweight or obese.
At the pre-study screening, the pain intensity for all subjects included in the study was 2 or more (mean 4.7, SD 1.8), measured on the NRS (0–10). Most of the study subjects (82%) experienced LBP on a few or most days of the week, but not daily, and 18% had daily LBP. The corresponding percentages at the baseline measurement were 72% and 12%, and 16% had recovered from pain. Duration of the LBP symptoms was less than 3 months for 65%, 3–6 months for 15% and more than 6 months for 21% of the study population at baseline. For 45 persons, the duration of symptoms of LBP exceeded 6 months during the waiting time between pre-study screening and baseline measurements. The majority of them (84%) experienced LBP on a few or most days of the week, but not daily, and 7 persons had daily pain. The selected study population can be described as nursing personnel with acute or sub-acute NSLBP with recurring pain behaviour. Only 15% (33 subjects) had been on sick leave due to LBP within the previous 6 months (36).
Table I. Baseline characteristics of the study sample (n = 219)
Descriptive data for the measurements (independent and dependent variables) are shown in Table II. Participants perceived themselves as having moderate bodily pain: mean 63.1 (SD 19.0) on a 0–100 scale (from 0 = very severe pain/extreme difficulties to 100 = no pain/no difficulties). The median for physical functioning was 90 (Q1 = 80, Q3 = 95, scale 0–100), and the median for self-assessed current and future work ability was 23 (Q1 = 21, Q = 24, scale 3–27).
Table II. Descriptive data for the dependent and independent variables (n = 219)
The association between physical and psychosocial factors and (i) bodily pain, (ii) physical functioning, and (iii) work ability were calculated. The results are shown in Table III for continuous independent variables and in Table IV for categorical independent variables.
Table III. Correlations between various physical and psycho-social factors and (i) bodily pain, (ii) physical functioning, and (iii) work ability (statistically significant correlations in bold)
Table IV. Associations between physical factors, all categorical variables and (i) bodily pain and pain interfering with normal work, (ii) physical functioning, and (iii) perceived current and future ability to work (statistically significant p-values in bold)
Higher values for physical functioning were detected in those who met recommendations for aerobic exercise (p = 0.05) and strength training (p = 0.02) than in those who did not meet the recommendations (Table IV).
Post-work recovery was associated with physical functioning (p = 0.003) and ability to work (p < 0.001). Subjects who were recovering well had higher scores for physical functioning and work ability than those who had some difficulties in recovering or who did not recover after work.
Perceived work-induced lumbar exertion was associated with bodily pain (p < 0.001). Those who perceived themselves very exerted had more pain than did those who perceived little exertion (mean difference 17.4, 95% confidence interval (95% CI) 9.9, 24.9, p < 0.001) or moderate exertion (mean difference 13.3, 95% CI 6.3, 24.4, p < 0.001). Work-induced lumbar exertion was also associated with levels of physical functioning (p < 0.001) and ability to work (p < 0.001); little exertion was linked to higher scores for physical functioning and ability to work.
Physical fitness and work-induced lumbar exertion: results of the physical fitness tests were consistently lower in those who perceived more work-induced lumbar exhaustion in comparison with subjects who were less exhausted (p < 0.05). The results are shown in Table V.
Table V. Associations between fitness-test results and perceived work-induced lumbar exertion, analysed by analysis of variance (ANOVA) and adjusted for age (p–values reflecting statistically significant differences in bold)
Factors with statistically significant (p < 0.05) associations with dependent variables in bivariate analysis (see Tables III and IV) were included in GLM analysis. Factors showing a statistically non-significant association with dependent variables were eliminated 1 by 1 in the GLM analysis. The results of the GLM-based analysis with statistically significant associations are presented in Table VI and depicted graphically in Fig. 2.
Table VI. Statistically significant associations between different biological and psychosocial factors and (i) bodily pain and pain interfering work, (ii) physical functioning, and (iii) perceived current and future ability to work, analysed via generalized linear models
Fig. 2. Associations of: (i) physical factors and (ii) psychosocial factors with 3 dependent variables: bodily pain, physical functioning, and perceived current and future ability to work, analysed via generalized linear models. A solid line indicates factors that were associated with all 3 dependent variables.
The factors associated with having bodily pain were perceived post-work lumbar exertion (high exertion vs. little exertion, β = –13.95, p < 0.001, n = 206), FABs related to work (β = –0.44, p = 0.02, n = 206), and number of musculoskeletal pain sites (β = –3.06, p < 0.001, n = 206). Negative β coefficients are explained by coding of bodily pain with descending values: a high score indicates no pain.
When the analyses were adjusted for age, BMI, work type (shift work/regular work), hormonal status, work satisfaction (including work-related stress), and previous sick leave due to LBP, statistically significant associations were found also between work type (β = –10.72, p < 0.001), previous sick leave (β = 0.35, p = 0.02) and bodily pain.
Lower work-induced lumbar exertion (β = –0.075, p = 0.005, n = 174), lower values for FAB-W (β = –0.004, p = 0.01, n = 174), a higher number of modified push-ups (β = 0.008, p = 0.045, n = 174), and shorter times for running a figure-of-eight (β = –0.033, p = 0.01, n = 174) were associated with better physical functioning. No significant changes were detected after adjustments.
Lower work-induced lumbar exertion (β = –0.052, p = 0.003, n = 192), lower FAB-W (β = –0.004, p < 0.001, n = 192), lower scores for depression (β = –0.003, p = 0.045, n = 192), and higher scores for perceived recovery after work (β = –0.03, p = 0.03, n = 192) were associated with higher scores for work ability. No significant changes were detected after adjustments.
The results of the final regression model indicate that perceived work-induced lumbar exertion and work-related FAB best explained the levels of pain, physical functioning, and work ability. Multi-site musculoskeletal pain was associated with higher levels of pain and lower physical functioning. Higher musculoskeletal performance level (assessed by modified push-ups and figure-of-eight running) was associated with better physical functioning.
The first dependent variable was bodily pain interfering with normal work. We chose a sub-scale for bodily pain from RAND-36 (22) in preference to a visual analogue scale (VAS) (1–100) (37), because we considered it more informative than VAS in a population performing physically demanding work. Work-induced lumbar exertion, multi-site pain, and FAB-W were all associated with perceived pain in GLM analysis.
The average number of musculoskeletal pain sites was 3.2 in the study sample. Multi-site pain seems quite common in nursing personnel, with 1-year prevalence of 60% among Estonian nurses (38). Multi-site pain is a strong predictor of sickness-related absences (39) and early retirement (40). In a recent cross-sectional study conducted among healthcare providers (41), multi-site musculoskeletal pain was associated with perceived ability to work, with the magnitude of association likely to increase with the number of pain sites.
In the study reported here, shift work was associated with more bodily pain in the GLM analysis. Most of the study subjects performed shift work, which is often associated with sleep disturbances and poor recovery. These, in turn, can affect perceptions of pain (42).
Higher fitness level in the modified push-up test was associated with better physical functioning in GLM analysis, and lower work-induced lumbar exertion in bivariate analysis. The modified push-up test requires both upper-body muscular strength and trunk stabilization, and low performance levels in this test have been associated with low-back dysfunction and pain in middle-aged subjects (43). In a study reported on by Kolu et al. (36), conducted with the same participants as the study reported here, the highest third with regard to aerobic and musculoskeletal performance capacity (measured by 6MWT and by modified push-ups) had lower sickness-related absence rates for the 6 months prior to baseline measurements than did those whose performance capacity was poor (specifically the lowest tertile). Our results are in line with earlier findings indicating that impaired physical functioning predicts development of persisting, disabling LBP (44).
This study indicated that poor results in running a figure-of-eight (which requires agility and power in the lower extremities) were associated with poor physical functioning in GLM analysis, and number of 1leg squats was strongly linked with perceived levels of work-induced lumbar exertion. Previous scientific evidence of this finding is limited. However, it can be assumed that nursing personnel with poor strength and power in the lower extremities are more prone to use their back musculature in lifting and transferring patients, and they might perceive lumbar exertion for this reason.
In the bivariate analysis we found that performance levels in aerobic, motor, and musculoskeletal fitness tests were systematically lower in those who perceived more work-induced lumbar exhaustion in comparison with those who were less exhausted. Poor endurance leads to exhaustion and fatigue at the end of a work shift, and fatigue, in turn, is known to decrease perception and motor control (45), thereby intrinsically raising the risk of injury in physically demanding tasks.
Work ability in cases of musculoskeletal disease is affected by several physical, psychosocial, individual-level, and environmental factors (46). In our study, the strongest associations with better work ability were detected in GLM analysis with lower work-induced lumbar exertion, better perceived recovery from work, lower depression, and lower FAB-W.
Managing physically demanding work and having low-back troubles is a challenging combination. Perceived work-induced lumbar exertion depends on exposure to physical loads, the length of the work shift, and personal physical capacities. Handling physically demanding work without incidents of LBP probably requires sufficient physical capacities, but exact cut-off points in fitness-test results are unknown. Therefore, further research is needed.
Depression was associated with levels of perceived current and future ability to work. If one is having negative thoughts about the present, perceived prognosis regarding work ability may also be bleak. In a recent systematic review (47), Pinheiro et al. suggested that depression might also have an effect on LBP prognosis in the acute or sub-acute phase.
Only 15% of the study sample had been on sick leave due to LBP within the previous 6 months. This percentage is surprisingly low, in light of the fact that the mean for pain intensity was 4.7 (on a 0–10 scale) at the point of screening. Perhaps either the participants’ perception of minor pain was high on account of difficulties in physically heavy work, or they did not want to go on sick leave in economically hard times, when substitutes cannot be hired.
In our study, FAB-W was associated with all 3 dependent variables in GLM analysis. All of the participants in the study worked with bedridden patients or carried out other physically demanding nursing tasks, such as lifting and transferring patients. Those tasks are heavy and cause seriously harmful load on the back structures (48). Therefore, it is understandable that nursing personnel’s attitudes to some work duties are filled with trepidation.
FABs play a central role in chronic LBP when organic pathology is not evident (49). The role of FABs in non-chronic populations is unclear, but it seems that it is linked to the transition of pain to the chronic stage (50) and plays a key role in recovery (44). For nursing personnel with previous LBP, both FABs and physical work load are associated with new episodes of LBP (8, 51).
In this study psychosocial factors and physical performance level were strongly associated with pain, physical functioning and work ability in female nursing personnel with recurrent LBP and physically burdensome work. This association has been widely documented in chronic LBP populations (11, 12, 15), but hardly in people with sub-acute NSLBP with recurring pain behaviour.
Level of work-induced lumbar exertion was assessed with a simple question offering 5 alternatives. This measurement showed strong associations with pain, physical functioning, work ability and level of physical fitness. Therefore, it could be used as a screening tool in assessment of risks for prolonged disability and possible reduced work ability. Those who perceive high work-induced lumbar exertion could benefit from fitness tests and exercise counselling.
Measurement methods to screen people who have a physically demanding job and may be at risk of persistent LBP are needed in occupational health services. The findings of the study reported here might be useful in development of practical tools for screening. For the most part, we used measurements whose reliability and validity have been tested previously. Nevertheless, some limitations of the measurements can be cited: (i) the Finnish version of the short form of Beck Depression Inventory has not yet been validated, (ii) no reliability studies have been carried out for questionnaires on the site quantity in cases of multiple musculoskeletal pain sites, and (iii) interpretations of cut-off-points for several measurements are unclear among people with a physically demanding job.
Another limitation of the study is its cross-sectional design. Interpretations of causality cannot be made. Hence, a prospective study is needed, to explore the causality of the elements propose to be factors in perceived pain, physical functioning, and work ability. In the NURSE RCT, LBP intensity and sick leave due to LBP are asked about at the 12- and 24-month follow-up.
In conclusion, perceived work-induced lumbar exertion and work-related FABs were factors that were associated with bodily pain, physical functioning, and work ability in a sample of nursing personnel with recurrent LBP. Level of physical fitness was related to work-induced lumbar exertion. Therefore, interventions designed to increase levels of fitness capacity and preventive efforts, such as back-related counselling to reduce levels of fear-avoidance, might be of importance for maintaining ability to work in nursing duties.
The authors wish to thank the Social Insurance Institution of Finland and the Tampere University Hospital for financial support for the NURSE RCT, and researchers from Finnish Institute of Occupational Health; Sirpa Lusa, PhD, and Harri Lindholm, PhD, for contributing to the study design and measurement selection.
The authors declare no conflicts of interest.


 Click to show fullsize
Click to show fullsize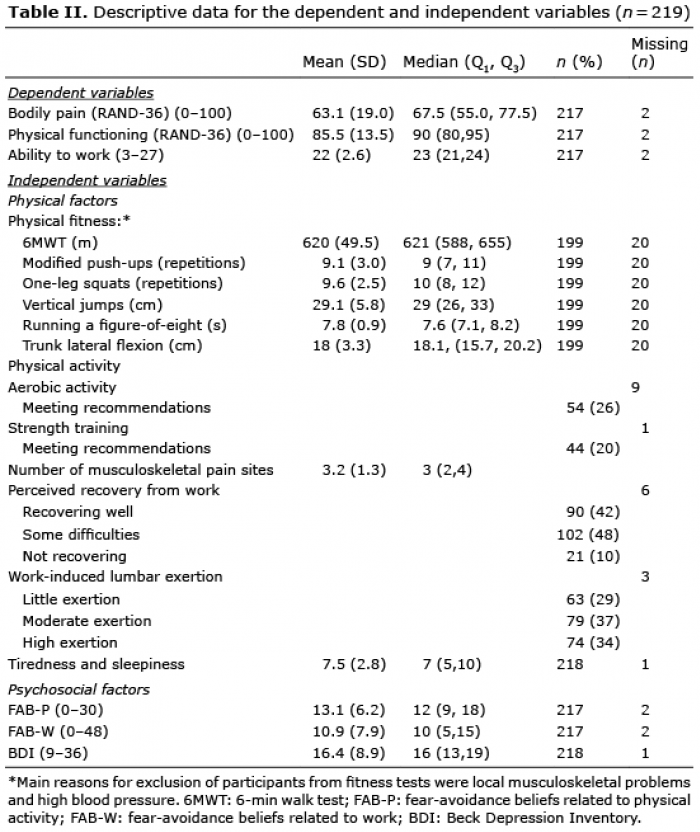 Click to show fullsize
Click to show fullsize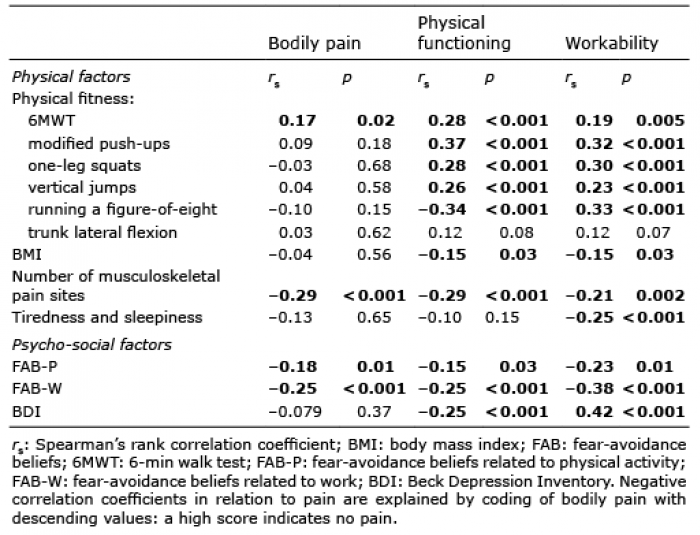 Click to show fullsize
Click to show fullsize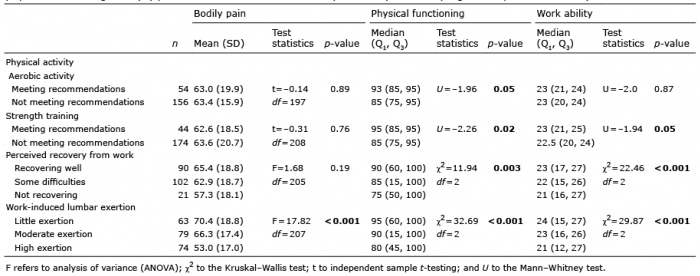 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize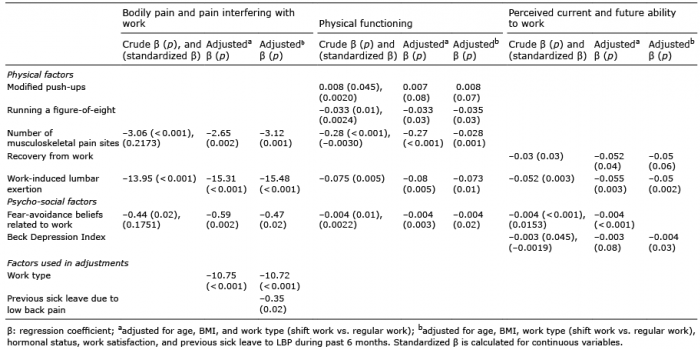 Click to show fullsize
Click to show fullsize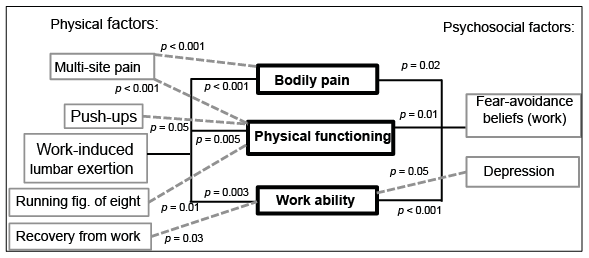 Click to show fullsize
Click to show fullsize