
Department of Rehabilitation Medicine, Hannover Medical School, Hanover, Germany
Objective: A technical consultation to develop a National Disability, Health and Rehabilitation Plan (NDHRP) for Egypt was carried out in 2015. Its overall goal was to improve health, functioning, well-being, quality of life, and participation of persons with disability in Egypt by supporting the Ministry of Health and Population and other stakeholders to improve access to health services and strengthen health-related rehabilitation services for all persons in need.
Methods: The methodological steps of the technical consultation were as follows: collecting and reviewing accessible documents and data; site visits to state institutions, health and rehabilitation services; discussions with relevant stakeholders in rehabilitation, including persons with disability; drafting recommendations based on the principles of the World Report on Disability and the World Health Organization Global Disability Action Plan and the information collected; discussion with stakeholders in a workshop; and preparation of a final report.
Results and discussion: The development of a NDHRP was successful and led to recommendations with a good level of consensus among stakeholders in Egypt. The authors hope that the NDHRP will lead to improved rehabilitation service provision, and health and quality of life of persons with disability and chronic health conditions living in Egypt.
Key words: rehabilitation service situation analysis; rehabilitation advisory teams; National Disability, Health and Rehabilitation Plan; rehabilitation services; rehabilitation professions; Egypt.
Accepted Nov 17, 2017; Epub ahead of print Jan 31, 2018
J Rehabil Med 2018: 50: 00–00
Correspondence address: Christoph Gutenbrunner, Department of Rehabilitation Medicine, Hannover Medical School, Carl-Neuberg-Str. 1, DE-30625 Hannover, Germany. E-mail: gutenbrunner.christoph@mh-hannover.de
Egypt has a rapidly growing population. The estimated population in 2009 was 84 million, and in 2013 it exceeded 90 million. Approximately 31% of the population is under 15 years old and only 9% is over 60 years old (1). Life expectancy at birth is 70 years for males and 74 years for females. Healthy life expectancy is 59 and 74 years in males and in females, respectively. Egypt is classified by World Bank as a lower-middle income country. Health expenditure is 5.6% of gross domestic product (GDP) (2).
In 2015, a technical consultation was carried out to develop a National Disability, Health and Rehabilitation Plan (NDHRP) for Egypt. The overall goal of the technical consultation was to improve health, functioning, well-being, quality of life, and participation of persons with disability in Egypt by supporting the Ministry of Health and Population (MOHP) and other stakeholders to improve access to health services and to strengthen health-related rehabilitation services for all persons in need.
The NDHRP should be based on an analysis of the present life situation of persons with disability, existing services, and international standards. It should help the government of Egypt to respond to proposed action for World Health Organization (WHO) member states set out in the Global Disability Action Plan 2014–2021: Better Health for all People with Disability (GDAP; 3). The plan should analyse the existing situation, including epidemiological data, policies, health services, challenges, opportunities, gaps and other factors.
The technical consultation was performed as described by Gutenbrunner et al. (4). The stages of the consultation (5) were:
The highest cause of mortality in Egypt is cardiovascular diseases (46%), followed by non-communicable dieseases (NCDs) (11% communicable maternal, perinatal, and nutritional conditions and 19% other communicable diseases), cancer (14%) and injuries (5%) (6). The burden of disease in terms of disability-adjusted life years (DALYs) is highest in cardiovascular diseases and diabetes, followed by other NCDs, neuro-psychiatric conditions, cancer and unintended injuries (1).
Disability rates in Egypt are reported to be very low (0.7% of the total population). This is the second lowest value reported in the Arab region (range 0.6–4.9%) (7), are are much lower than the average from international comparative data (8). Thus, the figures seem unrealistic and the method of data collection should be further elucidated. The employment rate of persons with disabilities is half that of the healthy population (21% vs. 40%) (7). According to these statistics, the major causes of disability are congenital abnormalities (51.9%), followed by injuries/accidents (13.9%), old age (9.4%), epidemic and other diseases (6.9% and 6.8%), and birth-related conditions (5.4%). The disabilities related to neurological and mental health conditions are not mentioned in this survey.
The healthcare system in Egypt has been called “pluralistic”, as it includes many different public and private providers (9). The main service provider is the MOHP; however, some public health services are provided by private institutions, the armed forces and n-governmental organizations (NGOs).
The health insurance system in Egypt is also highly segmented. As determined through site visits, health insurance in Egypt is based on 7 different laws, and covers women with responsibility for their family, farmers, pre-school children, school children (approximately 60% of all children), governmental workers (some non-governmental workers are insured by their companies), pensioners and widows. The overall coverage of public health insurance in 2015 amounts to 58% of the total population. However, 72% of total health spending is still paid by induviduals (10). New law on health insurance drafted by MOHP states that coverage should reach 100%; however, due to the political situation, this law has not yet been adopted by the national parliament.
The workforce of rehabilitation professionals consists mainly of physical medicine, rheumatology and rehabilitation doctors, and physiotherapists. In addition, some speech and language therapists are available. Other rehabilitation professionals, such as occupational therapists, prosthetists and orthotists, are not regularly trained in Egypt.
There is scarce information about existing rehabilitation services. There are 2 main reasons for this: first, there is no clear definition of a rehabilitation service; and, secondly, there is no systematic statistical approach. Shafshak (11) reports that 195 MOHP hospitals and 18 university hospitals have special departments for Physical and Rehabilitation Medicine (PRM). In addition, it is mentioned that PRM departments exist in internal security and armed forces hospitals. However, their role in healthcare and its structure are not described in detail. Furthermore, the paper mentioned 60 physiotherapy and rehabilitation centres run by the Ministry of Social Affairs. These centres have at least one MD and a physiotherapist. Overall, these data are not sufficient to estimate whether the needs of persons with chronic health conditions experiencing disability are sufficiently covered.
Recently, a Health Sector Reform Program has been started by Egyptian government, with the aims of expanding the social insurance coverage from 47% in 2003 up to universal coverage, reorganizing services aiming at service provision through a holistic family health approach to strengthen management systems, and developing a domestic pharmaceutical industry (10).
The new constitution of the Arab Republic of Egypt places health at a high level of priority on the national agenda (10). In Article 18 of the constitution the right to health, among others, is guaranteed as follows:
In order to achieve these goals, health expenditure should be doubled and increase to 3% of GDP.
The rights of persons with disability are guaranteed in Article 81 of the constitution: “The state is committed to ensuring the rights of persons with disabilities and dwarves [sic], in all aspects; health, economic, social, cultural, entertainment, sports and education, and provide job opportunities for them, with the allocation of a percentage of jobs to persons with disability, and also is committed to the creation of enabling public facilities and environment surrounding them (…)”.
In summary, the main findings from site visits were:
Preliminary recommendations were developed following evaluation of the information collected. These recommendations were discussed in a stakeholder dialogue (12) with 20 representatives of the following organizations: Hannover Medical School (technical advisor), Ministry of Public Health, Ministry of Social Solidarity, the Health Insurance Head Office, the National Council of Disability Affairs, National Society of Rheumatology and Ain Shams University, Physiotherapy Faculty of Cairo University, Speech Faculty of Medicine of Cairo University, Physiotherapy Department of Cairo Governate, Caritas Egypt, as well as specialists in Neurology and Disability and Physiotherapy, and the mother of an autistic child. After a consensus-oriented discussion of each recommendation the participants could vote on the relevance of each recommendation.
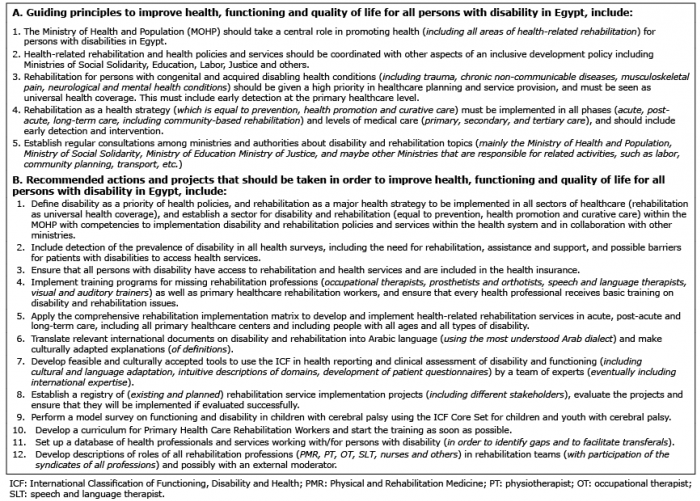
The resulting recommendations are summarized in Box 1.
Box 1. Guiding principles and recommendations of the National Disability, Health and Rehabilitation Plan for Egypt
Although this was the first time a technical consultation for the development of a National Disability, Health and Rehabilitation Plan had been carried out, overall the consultation was successful and led to recommendations with a good level of consensus among stakeholders in the country.
Methodologically, the consultant (CG) used open source data on Egypt, its health system, epidemiology, and other factors. During the site visits he held open discussions with stakeholders, including ministries, external experts, service providers, rehabilitation professionals, the National Council of Disability Affairs, and others. As a framework, the consultant used the recommendations of the World Report on Disability, bearing in mind the more extensive list of actions from the GDAP. In parallel, the consultant developed a comprehensive list of relevant information to be assessed beforehand (e.g. by using a Rehabilitation Service Assessment Tool (RSAT)) (5).
An important aspect of the site visits was discussion of the draft recommendations with the most relevant stakeholders. During the single meetings and site visits, some points of controversy among stakeholders became obvious, e.g. the role of health professionals in rehabilitation services. There was a high level of agreement following careful examination of each point of the recommendations and projects list. Critical points were discussed openly and additional proposals were integrated into the final version. Agreement was documented according to each participant’s scores. The overall scores were high; however, they were also useful for identifying difficult points, e.g. implementation of the International Classification of Functioning, Disability and Health (ICF) in health reporting and rehabilitation quality management.
The results of this technical consultation show that many factors need to be considered in order to achieve the goal of implementing rehabilitation services for all persons in need. This includes governance and (political) leadership, financing, service delivery, rehabilitation workforce, access to essential services, and health information which is coincidence with health system building blocks (reference: World Health Organization. Monitoring the building blocks of health systems: a handbook of indicators and their measurement strategies. Geneva: World Health Organization; 2010). Experience of such activity is available from the Ukraine (13). However, a more systematic approach to service implementation strategies is needed (including description of prototype rehabilitation services) (see also (4)).
Although the recommendations and projects reached a high level of agreement among stakeholders, including ministries, persons with disabilities, health professionals and service providers, the success of the mission is difficult to predict. Some barriers may come from the political situation in a country (e.g. changes in ministries, parliamentary elections, etc.) and the huge effort needed towards implementation of rehabilitation as universal health coverage. The authors hope that the NDHRP leads to improvements in rehabilitation service provision and in the health and quality of life of persons with disability and chronic health conditions living in Egypt.


 Click to show fullsize
Click to show fullsize