
From the 1Department of Physical Medicine and Rehabilitation, 2Department of Neurosurgery, Oslo University Hospital, 3Institute of Health and Society, Research Centre for Habilitation and Rehabilitation Models and Services (CHARM), Faculty of Medicine, 4Institute of Clinical Medicine, Faculty of Medicine, University of Oslo, Oslo, Norway, 5Department of Family Medicine and Population Health, Division of Epidemiology, Virginia Commonwealth University, Richmond, VA, USA, 6Division of Clinical Neurosciences, Department of Rehabilitation and Brain Trauma, Turku University Hospital, Turku, Finland, and 7Department of Neurology, University of Turku, Turku, Finland
Objectives: To describe the discharge process for patients with traumatic brain injury from a trauma hospital, and patient experience and satisfaction with care transition. Furthermore, to evaluate associations between discharge process and patient satisfaction and quality of care transition.
Design: Prospective-retrospective observational study.
Subjects/patients: Seventy-four patients admitted to ward or intensive care unit at a trauma referral hospital within 24 h of traumatic brain injury.
Methods: Baseline characteristics and discharge process variables were extracted from medical records. Patients were interviewed 6-months post-injury about their experience and satisfaction with care transition, using a visual analogue scale (VAS) and the Care Transition Measurement (CTM-3®) as outcome measures. Regression analyses were performed to investigate associations between discharge process and outcome.
Results: One-third of patients were not involved in the discharge process, and information in discharge summaries was often inadequate. Patients’ involvement in care transition and co-ordination of care were significantly associated with overall satisfaction (VAS, p = 0.002 and p = 0.001, respectively) and quality of care transition (CTM-3®, p = 0.003 and p = 0.007, respectively). Patients with more severe injuries reported lower satisfaction and quality of care transition.
Conclusion: Patient’s involvement in healthcare decision-making and co-ordination of care is important for self-reported satisfaction with transition and quality of care transition.
Key words: patient transfer; patient discharge; brain injury; craniocerebral trauma.
Accepted Feb 21, 2018; Epub ahead of print Apr 5, 2018
J Rehabil Med 2018; 50: 00–00
Correspondence address: Cathrine Buaas Tverdal, Department of Physical Medicine and Rehabilitation, Oslo University Hospital, PO Box 4950 Nydalen, NO-0424 Oslo, Norway. E-mail: cathrinebt@gmail.com
Discharge from a trauma hospital represents an important event, because that is when plans are made regarding further need for follow-up and healthcare services. However, we do not have sufficient information about how discharge is planned for people who have had a traumatic brain injury (TBI), how the patients perceive this process, or how satisfied they are with it. This study investigated to what degree the discharge was planned, by reviewing information in the medical records and by asking the patients about their experience and satisfaction with the discharge process. It was found that the degree to which the discharge was planned varied, and the main factors affecting how the patients perceived the quality of the discharge process and how they rated it, was the experience of being involved in the discharge process and how well-coordinated it was. Patients with more severe overall injury were less satisfied with discharge and its quality, suggesting that special consideration should be given to patients with more severe injuries.
Traumatic brain injury (TBI) is defined as a disruption of brain anatomy or function, caused by external force (1). Each year, approximately 1.4 million people in Europe are admitted to hospital with a TBI (2), including approximately 14,000 in Norway (3, 4). When acute treatment goals are accomplished at the trauma hospital, the discharge destination of inpatients with TBI depends on the patient’s functional level and need for further healthcare. The hospital discharge serves as an important transition of care because decisions and recommendations regarding further care are made at that point.
Coleman & Boult (5) defined transitional care as “a set of actions designed to ensure the coordination and continuity of healthcare as patients transfer between different locations or levels of care”. Care transition involves different healthcare professionals, and includes logistical arrangements and information for the patient and family members. For healthcare professionals it requires knowledge of acute and chronic care needs, and information about patients’ goals, preferences and clinical status (6). Transitions may be insufficiently planned, leading patients and family to be unprepared (7). Furthermore, care transitions can be associated with errors in communication of information and treatment plans. This may lead to poor clinical outcomes, medication errors, dissatisfaction and inappropriate use of healthcare resources (5, 6, 8–10). Discharge planning tailored to individual patients ensures that patient needs are evaluated, discussed and communicated, leading to increased satisfaction for patients and healthcare professionals (11). The discharge summary is not the only tool for discharge communications, but serves as an important resource (10). A systematic review by Kripalani et al. (12) found that discharge summaries varied in structure, are delayed and frequently incomplete.
Patient involvement and participation in transition of care is one way of improving the quality of care transitions for older patients (13). The World Health Organization (WHO) emphasizes the importance of patient participation concerning all levels of healthcare (14, 15). Studies on elderly people and patients with stroke show that participation and adequate information are important factors for a successful hospital discharge (7, 16, 17). Most of the transition literature on brain injuries focuses on elderly patients with stroke and rehabilitation needs (18). There is a lack of studies investigating the discharge process for patients with TBI, which is especially important because they often receive treatment from different professionals and wards. Based on observations in clinical practice, and feedback from patients, discharge from trauma hospital can sometimes be hasty, and patients may not receive enough information about their condition, prognosis and what to expect after discharge. One important strategy towards improving this is measuring patient satisfaction and quality of care transitions.
The objectives of this study are to describe the discharge process for patients with TBI from a trauma hospital and patient experience and overall satisfaction with care transition. We also wanted to evaluate associations between discharge process, patient satisfaction and quality of care transition.
We hypothesized that patients with more severe injuries would have lower satisfaction and quality of care transitions, as predicting the recovery and outcome is more difficult for these patients, potentially leading to inadequate decisions and suboptimal transitions.
This is a single-centre observational study, with a prospective design, performed as part of “Work Package 14: Transitions of care and post-acute care” of the European multicentre study, the CENTER-TBI project (Collaborative European Neuro Trauma Effectiveness Research in TBI) (19). Patients were interviewed at the 6-month study follow-up regarding their overall satisfaction and experience with care transition when they had been discharged from the acute trauma hospital.
Oslo University Hospital (OUH) is the Level 1 trauma referral centre for the South-Eastern region of Norway, with a population base of 2.9 million. OUH provides acute TBI care at the Neurosurgical and/or Neuro-intensive care departments (ICU). In addition, the early rehabilitation for patients with severe TBI is provided at the ICU, and the intermediary/subacute rehabilitation at the rehabilitation department. When acute care is completed at OUH it is the patients’ postal address in the national registry that determines which of approximately 20 local hospitals in the region is responsible for further treatment and rehabilitation and to where the patient is discharged. General practitioners are responsible for follow-up of patients discharged directly home.
Patients who were 16 years or older, admitted to OUH between June 2015 and March 2016, and enrolled in the CENTER-TBI study were included consecutively. The CENTER-TBI inclusion criteria were (19): (i) clinical diagnosis of TBI; (ii) clinical indication for a computed tomography (CT) scan (based on the standard clinical practice of the hospital); (iii) presentation within 24 h of injury; and (iv) informed consent obtained according to local and national requirements. Exclusion criteria were: severe pre-existing neurological disorders that would confound outcome assessments. Patients were stratified into 3 groups upon enrolment, according to the clinical care they received: emergency room (ER) stratum (patients evaluated in the ER, then discharged); admission stratum (patients admitted into hospital, but not to the ICU) ICU stratum (patients admitted directly to the ICU, from the ER or other hospital) (19).
Because the focus of this sub-study was on the discharge process, following inpatient admission to a trauma hospital, and the consent form was only in Norwegian, patients in the ER stratum and those unable to speak Norwegian were excluded.
The main outcomes of interest were measures of overall satisfaction with care transitions and quality of care transition during hospital discharge from the patient’s perspective. In the literature, satisfaction is often assessed as a global measure, whereas experience relates more specifically to quality of healthcare services.
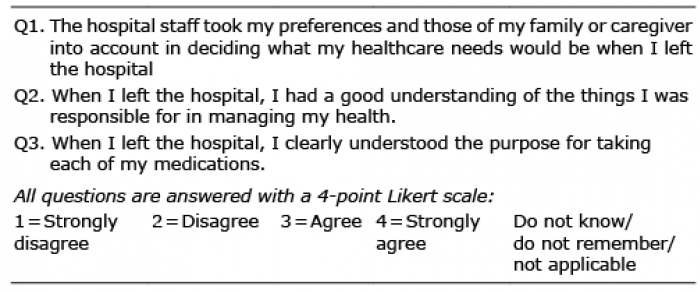
The instruments used were “Patient’s overall satisfaction with care transition”, measured by visual analogue scale (VAS) and “Quality of care transition”, measured with the sum score of the Care Transition Measure-3® (CTM-3®). Both outcome measures are scaled from 0 to 100 (worst-to-best), where a higher score indicates greater satisfaction and experience. The CTM® was developed as a tool to assess the quality of care transitions across healthcare settings from the patient perspective (20). The original CTM® had 15 items (CTM-15®), later decreased to 3 (CTM-3®) to reduce the response burden, each being recorded on a 4-point Likert scale, so a linear transformation could be performed to obtain a score on a scale from 0 to 100 (21, 22). Table I shows the questionnaire. The CTM® has been tested and found to have acceptable reliability and validity (20–23).
Table I. Care Transitions Measure® (CTM-3®)
Discharge process variables. The main aim of the discharge planning process is to ensure safe and effective discharges and access to the right service at the right time. Assessment of patient needs, appropriate referrals, continuity of care and involvement of patient/family are of major importance in this process (10, 11, 14, 24). Variables are listed below, and are further presented in Tables II and III as part of the results.
Table II. Demographics, injury characteristics and discharge information
Table III. Discharge planning process
Patients were asked at follow-up if they were involved in the discharge process from trauma hospital (no/yes), and if they experienced continuity in healthcare (no/yes).
Variables describing the discharge process used in this study were: discharge planning noted in medical records (no/yes; “yes” if noted by doctor/nurse in medical records at latest day prior to discharge), discharge destination (home, other hospital, rehabilitation unit, nursing home, other; dichotomized to home/institution), discharge weekday (Monday–Friday/Saturday–Sunday), discharge delayed (no/yes; “yes” if patient is clinically ready for transfer but there are no available beds at the receiving unit, or other logistic reasons), physician’s discharge summary present at day of discharge (no/yes), communication between sending and receiving team noted in medical records (no/yes).
Content of the physician’s discharge summary was assessed, based on key points of what a discharge summary should include (12), with 7 dichotomous (no/yes) quality indicators chosen, including: (i) pending tests/examinations indicated; (ii) discharge medications recorded; (iii) patient’s capacity for self-care and needs for healthcare services described; (iv) patient’s cognitive status and ability to communicate described; (v) patient’s goals and preferences incorporated into the care plan; (vi) need for co-ordinated healthcare services indicated; and (vii) timing of follow-up with appropriate health professionals indicated.
Demographic variables. Age (in years), sex (male/female), highest educational level (dichotomized to lower/higher, higher representing university/college degree), living situation (dichotomized to living alone or with other(s)) and employment status (dichotomized to working/student or not working).
Injury-related variables. Patient stratum (admission/ICU), lowest Glasgow Coma Scale score (GCS) on day of injury (before sedation) (3 = worst, 15 = best) (25), Injury Severity Score (ISS) (0 = no trauma, 75 = not survivable) (26, 27), length of stay at trauma hospital (in days), isolated TBI or TBI with associated injuries, intracranial surgery (no/yes), number of in-hospital transitions, Glasgow outcome scale at day of discharge (GOS 1 = dead, GOS 2 = persistent vegetative state, GOS 3 = severely disabled, GOS 4 = moderately disabled, GOS 5 = good recovery) (28).
Demographic data and injury characteristics are registered in the core database of CENTER-TBI. The patients’ electronic medical records were accessed for the discharge planning process, and the evaluation was conducted by the study nurse (CBT) and physician (NA), using a data collection chart to extract relevant data. The same persons performed the 6-month follow-up interviews. Questionnaires describing patients’ experience and satisfaction with care transition were administered to patients at the follow-up interview, or to their family if the patient had little or no recollection of the discharge (for example if they had GCS < 15 or post-traumatic amnesia phase at discharge).
SPSS version 24 was used for all analyses. Descriptive statistics were used to summarize the characteristics of patients, injuries and the discharge planning process. To compare group differences between admission and ICU stratum, we used Pearson χ2, or Fisher’s exact test for categorical variables, and independent t-test, or Mann–Whitney U test, for continuous variables. Two-sided p-values of 0.05 were considered for statistical significance.
Simple linear regression was applied to assess the univariate relationship between each independent variables and VAS and CTM-3®. Independent variables that reached statistical significance was further included in the subsequent multiple regression analysis. The variable patient stratum (admission/ ICU) strongly correlated (r > 0.7) with the injury severity variables, therefore was not included in the final analysis.
Two separate multiple regression models were estimated using a hierarchical approach (block-wise entry) (29), to assess relationships between the measures of discharge process and self-perceived overall satisfaction with transition and quality of care transition, accounting for baseline characteristics. Independent variables were entered in 3 blocks, including patients’ demographics, injury characteristics and hospital discharge or care transition related measures. We used a conservative approach of allowing 1 predictor for every 8–10 participants.
Results from the multiple regression modelling are presented in adjusted R2 and R2 change, and unstandardized B coefficient with 95% confidence intervals. Prior to carrying out the multiple regression analyses, possible multicollinearity between independent variables was investigated using a variance inflation factor. Normality of residuals was controlled for with inspection of histogram and p-p plots; no outliers were identified. To check for internal validity, the models were run with 1,000 bootstrap samples (29).
The study was approved by the regional ethics committee, REK Middle-Norway (approval numbers 2014/1454 and 2015/2307). All study participants received oral and written information, and provided written consent. For patients under 18 years of age, parents also provided written consent according to local policy. The burden of study participation for the patients was considered low; and expected to have no influence on medical treatment.
In the relevant timeframe, 104 patients were included in CENTER-TBI, and they were placed into admission or ICU stratum. Eight patients died shortly after injury, and 3 did not speak Norwegian fluently, leaving 93 eligible participants. Of these 93, 18 were not contactable for follow-up and 1 withdrew prior to the 6-month follow-up, leaving 74 patients. There were no statistically significant differences between the 74 participants and the 30 patients who were not included in the current study, regarding stratum, age, sex, education, ISS and length of hospital stay.
The participants had a mean age of 44 years (standard deviation (SD) 19, range 16–85 years), and 70% were male; Table II shows the patient characteristics. Road traffic incidents accounted for 40% of the injuries; 42% were due to falls. Most injuries were mild TBIs, based on GCS assessment (72%). There were no statistically significant differences between admission and ICU stratum, in terms of demographics and cause of injury. As expected, there were statistically significant differences between admission and ICU stratum regarding injury characteristics (GCS p= < 0.001, ISS p= < 0.001, length of stay p= < 0.001, discharge destination p= < 0.001, discharge weekday p = 0.04). The majority of patients in the admission stratum were discharged directly home (86%), after a mean hospital stay of 3 days (median 2 days). Among patients in the ICU stratum, 91% were discharged to a local hospital or rehabilitation unit, and the mean length of hospital stay was 18 days (median 10 days). No patients were discharged directly to a nursing home.
The participants had a mean age of 44 years (standard deviation (SD) 19, range 16–85 years), and 70% were male; Table II shows the patient characteristics. Road traffic incidents accounted for 40% of the injuries; 42% were due to falls. Most injuries were mild TBIs, based on GCS assessment (72%). There were no statistically significant differences between admission and ICU stratum, in terms of demographics and cause of injury. As expected, there were statistically significant differences between admission and ICU stratum regarding injury characteristics (GCS p= < 0.001, ISS p= < 0.001, length of stay p= < 0.001, discharge destination p= < 0.001, discharge weekday p = 0.04). The majority of patients in the admission stratum were discharged directly home (86%), after a mean hospital stay of 3 days (median 2 days). Among patients in the ICU stratum, 91% were discharged to a local hospital or rehabilitation unit, and the mean length of hospital stay was 18 days (median 10 days). No patients were discharged directly to a nursing home.
Furthermore, there were several statistically significant differences regarding the discharge process between the strata (Table III). According to notes in the medical records, discharge from hospital was planned for 58% of patients, the majority being in the ICU stratum, and all ICU patients received discharge summaries at day of discharge. The following discharge process variables were in favour of ICU stratum patients: discharge from trauma hospital planned (p < 0.001); communication between sending and receiving team noted in medical records (p <0.001); discharge summary delivered at day of discharge (p <0.001); and discharge summary included information about need for co-ordinated healthcare services (p = 0.003). The timing of follow-up was indicated in the discharge summary more frequently than in the admission stratum (p = 0.002).
Table IV describes responses on the outcome measures VAS and CTM-3®. For overall satisfaction with care transition (VAS, range 0–100), there was a 100% response rate; mean 74 (SD 24), with no statistically significant differences between strata (p = 0.6). The outcome reflecting quality of care transition from the patient perspective (CTM-3®, range 0–100) had a response rate of 92%; mean 64 (SD 20), with no statistically significant difference between strata (p = 0.3). A total of 7 patients (9%) answered the questions with help from family members, all in ICU stratum, and with severe disability at the discharge as assessed by GOS.
Table IV. Outcome: patients overall satisfaction with care transition and quality of care transition
Results from model 1 investigating associations between age, sex, injury characteristics (GCS, ISS, length of stay, discharge place), patient experience of involvement in care transition and experience of care co-ordination, and overall satisfaction are presented in Table V. Age and sex had no statistically significant effect, explaining only 2% of the total variance in the satisfaction with care. Injury characteristics and discharge place explained 3% of variance.
Table V. Model 1: hierarchical multiple regression of patient overall satisfaction with care transition (n = 74)
Only the third step, with variables regarding patient involvement in the discharge process/transition of care and continuity of care, was statistically significant, and explained a total of 30% of the variance in the dependent measure. Both patient involvement in the discharge process (p = 0.002) and patient experience of co-ordinated healthcare (p = 0.001) reached statistical significance. The positive direction of an unstandardized B coefficient indicates that patients who were involved in the discharge process and co-ordination of healthcare also reported a higher satisfaction with care transition. The B value of ISS and length of hospital stay (LOS), representing the severity of the injury, was negative, indicating that more severe injuries were associated with lowered satisfaction with care (p = 0.07 and p = 0.05, respectively). Bootstrapping analysis supported the results for LOS (p = 0.03), patient involvement in discharge process (p = 0.004), and coordinated healthcare (p = 0.006), but not ISS (p = 0.14).
Model 2 investigated associations between age, sex, injury characteristics, discharge planning, patient involved in discharge process, and co-ordinated healthcare. The results are presented in Table VI.
Table VI. Model 2: hierarchical multiple regression of quality of care transition, measured with Care Transition Measurement (CTM-3®) (n = 68)
The first step did not reach statistical significance and explained 4% of the total variance in the dependent variable. By adding factors related to injury severity and discharge place, the amount of explained variance increased to 17% (p = 0.01). The third step, representing the patient’s perspective, showed statistical significance (p = < 0.001), explaining 36% of variance.
As in Model 1, the B value of ISS (p = 0.02) was negative, indicating that more severe injury was associated with worse quality of care transition. Also, the B value for the variable “patient cognitive status and ability to communicate described in discharge summary” (p = 0.01) was negative, indicating that patients who had no description of cognitive status and ability to communicate in the discharge summary reported lower quality of care transition. The B values of patient involvement in the discharge process and coordination of healthcare remained statistically significant in this model as well (p = 0.003 and p = 0.007, respectively). Bootstrapping analysis supported all statistically significant results in Model 2: ISS (p = 0.03), patient involvement in discharge process (p = 0.006), coordinated healthcare (p = 0.007), except the cognitive status and ability to communicate described in discharge summary (approaching statistically significance, p = 0.075).
The major factors affecting overall satisfaction and quality of care transition were patient experience of involvement in care transition and co-ordination of care. The results demonstrate that the discharge planning process varied, and that discharge summaries differed in structure and completeness. Furthermore, patients with more severe injuries (i.e. higher ISS and/or longer length of hospital stay), were less satisfied with transitions of care and its quality, in line with our hypothesis.
One-third of patients reported that they were not involved in the discharge process. A comparable number of patients did not experience continuity in their care transitions, hence not meeting the demands of patient-centeredness. In a qualitative study of elderly surgical patients, Perry et al. (30) found lack of an active role in the discharge, need for family support at home, uncertainty of how to return to usual activities, and a paternalistic medical model. Patient-centeredness (i.e. care that is respectful and responsive to individual preferences and needs) and participation in healthcare decision-making is highlighted in policy documents, both worldwide (15) and nationally (31). The patient perspective is an important area of WHO’s Patient Safety Strategy (14), and our results indicate a need for improvement in this area. The literature on patient participation in healthcare decisions emphasizes factors such as information provision, involvement of patient and family in discharge planning, and the attitude of healthcare professionals as important (7, 14, 16). Furthermore, an association between increased patient involvement and higher ratings of quality of care from the patient perspective has been described (7, 16), indicating that participation in healthcare decision may be a quality indicator of healthcare services.
Real participation may be difficult to achieve for patients with TBI shortly after injury, due to the nature of TBI recovery process. Patients with TBI may experience cognitive impairment in the acute phase. Furthermore, patients may have little previous experience with the healthcare system and limited knowledge about available resources. Coleman (6) stresses the importance of providing information to patients/caregivers of what to expect after discharge, but ensuring adequate information may not always be a simple matter in clinical practice (17). Paterson et al.’s study described a discrepancy in perceptions of information provided at the hospital, as caregivers for patients with TBI did not recall being given information, while healthcare professionals felt they had provided extensive discharge planning and education about the condition and services available (17).
Patients in the ICU stratum were more severely injured than patients in the admission stratum, thus they were in need of more complex medical treatment and care. Discharge was planned for a majority of ICU patients; however, only 41% were discharged directly to a rehabilitation unit. This is lower than expected, considering our previous recommendations regarding a continuous chain of treatment and rehabilitation after severe TBI (32, 33). Stenberg et al. (34) describes a similar situation in northern Sweden, where patients with severe TBI often were discharged to local hospitals and did not follow the desired rehabilitation chain. A substantial variation in structure and process of in-hospital rehabilitation and referral to rehabilitation facilities exists between European neurotrauma centres and future research is needed to study rehabilitation referral decision-making processes (35).
Kripalani et al. (12) addressed the issue of the discharge summary as a tool for discharge communication in a systematic review of information transfer, from inpatient to outpatient caregivers. The discharge summary is the most common method for documenting a patient’s diagnostic findings, hospital management, and arrangements for post-discharge follow-up (12). Kripalani et al. (12) found low availability of discharge summary on the day of discharge (12–34% available), lack of information regarding test results (missing in 7–22%), discharge medications (missing in 2–40%), test results pending at discharge (missing in 65%), patient or family counselling (missing in 90–92%) and follow-up plans (missing in 2–43%). In our study, we found that most discharge summaries were delivered on the day of discharge (80%); however, a substantial portion of discharge summaries did not provide information about a patient’s capacity for self-care and need for healthcare (68% missing), patient’s cognitive status and ability to communicate (37% missing), discharge medication (39% missing) and follow-up (30% missing).
Despite these findings, the content of the discharge summary did not influence the patient overall satisfaction (VAS). However, the description of a patient’s cognitive status and ability to communicate was a significant factor in a model of quality of care transition (CTM-3®). As the discharge summary is a significant tool for communication to the care-providers, the study findings may suggest that the quality of information transfer from trauma hospital is often inadequate. Reasons may be a shortage of time and work shifts, and different clinicians involved in the treatment of patients in an acute-care setting, thus lacking familiarity with patients and their medical histories (36).
Coleman (6) highlighted that patient complexity is an important risk factor for poor transitional care. Our results may indirectly support this, as we found that factors representing medical complexity (higher overall severity of trauma and longer hospital stay) negatively influenced satisfaction with transitions of care and quality of care transition.
For patients in the admission stratum, discharge was planned for only one-third of patients. This is probably explained by short hospital stays, where many patients are discharged the day following admission. The low rate of documented planning and involvement of patients in this study may support the description of pressure on acute hospital beds described in the literature (36, 37). Regarding the content of the discharge summary, the only factor in favour of patients in the admission stratum was more frequently described follow-ups, reflecting that these patients were discharged directly home, and referred to general practitioners and/or outpatient treatment, where discharge summary is used as a physician referral.
A major strength of this study is that the participants were adults of all ages, and with varying degrees of injury severity, thereby allowing the study to assess a broad range of care needs for this population.
The main limitations were that this was a single-centre study, with a small sample size, and that the majority of patients had mild TBIs, as assessed by GCS. The latter is in line with other studies conducted across the TBI severity levels in patients admitted to trauma centres (3, 38, 39). A small sample size limited the number of variables that could be assessed in the regression analysis; however, the internal validity of model stability by bootstrapping analysis supports our results. Although the models explain 30% and 36% of variance in patient satisfaction and quality of care transition, there are important factors we did not assess in this study, such as co-morbidity, post-discharge interventions, functional level and work-participation at follow-up, etc.
Furthermore, patients’ experience with transition and satisfaction with care were self-reported and a short version of care transition measurement with only 3 questions was used. Participants did not answer anonymously; however, to reduce this potential bias, honest feedback was encouraged.
A factor that is both a strength and a limitation is the time-point for patient feedback, which was 6 months post-injury. This is a strength because patients had time to experience how the injury affected their daily life and may have formulated opinions on what their healthcare needs were after hospital discharge. It is also a limitation because time weakens and affects memory, and response bias cannot be ruled out; however, in patients with more severe injuries, with possible cognitive deficits, family caregivers, considered to be reliable third-parties, verified the information (40).
Patients were discharged from several different wards, representing the reality of acute hospital treatment. This study might be of international interest, as it reflects practice in the largest trauma hospital in Norway, with a well-organized public trauma system and rehabilitation healthcare services.
We chose to isolate the process of discharge from trauma hospital because of its importance for decisions and recommendations concerning further care. Future studies should investigate the relationship between acute and post-acute transition of care and post-discharge interventions, and further explore the relations between transition of care, interventions and patient outcomes, health-related quality of life and hospital readmission. In addition, to assess and compare the quality of transition from multiple viewpoints (patient, proxies, nurses, doctors, discharging unit, receiving unit) soon after the transition is warranted.
Furthermore, it would be of great value to develop interventions for healthcare professionals working with TBI that facilitate patient participation in care transitions, as well as to enable patients/proxies to take part in decision-making processes.
The results of this study support existing literature that underlines the importance of patient and/or caregiver involvement during the discharge process. Our findings demonstrate that a patient’s experience of involvement in healthcare decision-making, and co-ordination of care, is important for self-perceived satisfaction with transition and quality of care transition.
One-third of patients reported they were not involved in the discharge process, and information in discharge summaries was often inadequate, suggesting that the discharge process was not optimal for all patients and should be improved. Furthermore, patients with more severe overall injury were less satisfied with transitions of care and its quality, suggesting that special consideration should be given to patients with more severe injuries and their family caregivers.
The authors would like to thank all participants. The study was supported by The European Union FP 7th Framework Program (grant 602150).
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize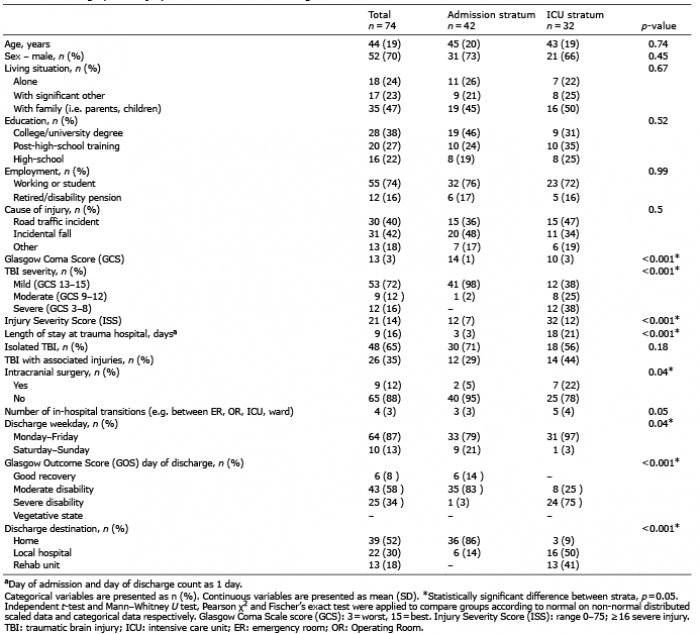 Click to show fullsize
Click to show fullsize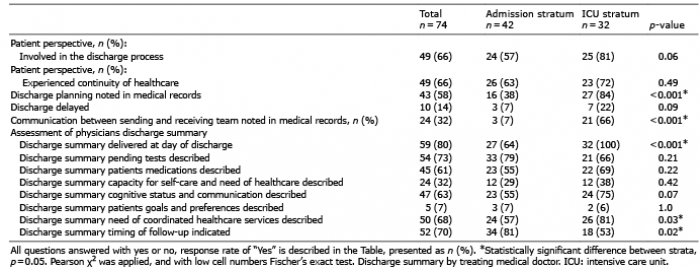 Click to show fullsize
Click to show fullsize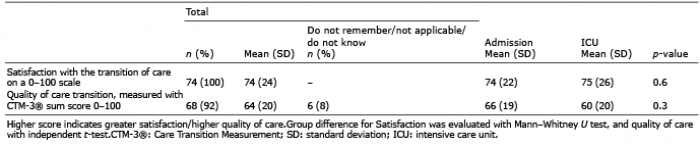 Click to show fullsize
Click to show fullsize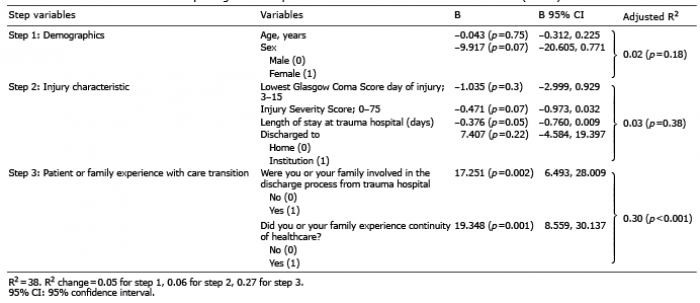 Click to show fullsize
Click to show fullsize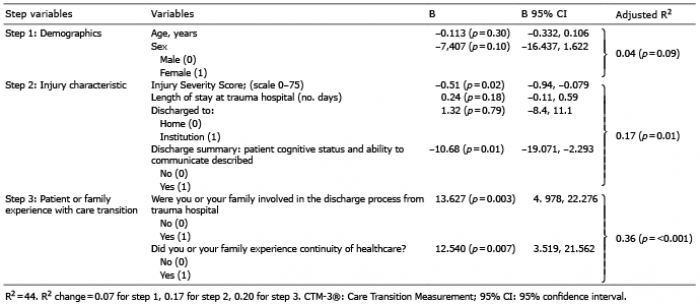 Click to show fullsize
Click to show fullsize