
From the 1Department of Rehabilitation Medicine and 3Department of Plastic and Reconstructive Surgery, Erasmus MC University Medical Center Rotterdam and 2Rijndam Rehabilitation, Rotterdam, The Netherlands
Objective: To develop and validate a clinically applicable and easy-to-use accelerometry-based device to measure arm use in people after stroke; the Activ8 arm use monitor (Activ8-AUM).
Design: Development and validation study.
Patients: A total of 25 people at different stages of rehabilitation after stroke were included in this study.
Methods: The Activ8-AUM consists of 3 single-sensor Activ8s: one on the unaffected thigh and one on each wrist. Arm use was calculated by combining movement intensity of the arms with data from body posture and movements on the leg sensor. Data were divided into 2 sets: one for determining situation-specific movement intensity thresholds for arm use, and the other to validate the Activ8-AUM using video recordings.
Results: Overall agreement between the Activ8-AUM and video recordings was 75%, sensitivity was 73% and specificity was 77%. Agreement between the different categories of arm use ranged from 42% to 93% for the affected arm and from 24% to 82% for the unaffected arm.
Conclusion: By combining the movement intensity threshold with body posture and movements, good agreement was reached between the Activ8-AUM and video recordings. This result, together with the easy-to-use configuration, makes the Activ8-AUM a promising device to measure arm use in people after stroke.
Key words: accelerometry; activity monitor; stroke; upper extremity; validation studies.
Accepted Apr 18, 2018; Epub ahead of print Jun 26, 2018
J Rehabil Med 2018; 50: 00–00
Correspondence address: Johannes B. J. Bussmann, Department of Rehabilitation Medicine, Erasmus MC University Medical Centre Rotterdam, PO Box 2040, NL-3000 CA Rotterdam, The Netherlands. E-mail: j.b.j.bussmann@erasmusmc.nl
*This article has been handled and decided upon by Chief-Editor Kristian Borg.
After a stroke most people suffer from an impaired arm resulting in limitations in daily life activities, greater dependency, and restrictions in social participation. Objectively measured arm use is important to evaluate the effect of motor rehabilitation. In addition, it can be used for personalized feedback and coaching for stimulating sufficient arm use. Therefore, we developed and validated a new easy-to-use and clinically applicable arm use monitor. This Activ8-AUM consists of three single-sensor accelerometers (Activ8) combining movement intensity of the arms (one sensor on each wrist) with data of body postures and movements (one sensor unaffected thigh). Combining these data, good agreement was reached between the Activ8-AUM data and reference video data. Therefore, this arm use monitor is a promising device to measure arm use in daily life after a stroke.
After stroke, approximately 75% of survivors have impairments of the arm, such as paralysis (1). These impairments often result in limitations in activities of daily living, greater dependency, and restrictions in social participation (2). Limitations in activities of daily living can be caused by reduced performance of the arm, which, in turn, may be the result of decreased capacity. However, the reduced performance can also be a result of other factors, leading to a discrepancy between what people can do (capacity) and what they actually do (performance), and in a weak to absent relationship between capacity and performance (3–5). This so-called non-use of the affected arm is an important topic in stroke rehabilitation (6). Therefore, in addition to measuring arm capacity with existing clinical measures, arm use also needs to be measured. Objectively measured arm use can be used to evaluate the effect of rehabilitation and, in coaching and feedback during rehabilitation, to stimulate arm use and personalize treatment.
Accelerometry has been introduced as an objective method to measure arm use in people after stroke (7–11). This technique is currently the only one that objectively measures arm use over long periods of time, and can thus be used to measure behaviour in daily life. Wrist-worn accelerometers measure arm movement and can provide a measure of arm use. However, the use of accelerometry to measure arm use has specific challenges, particularly regarding sensitivity and specificity: e.g. to what extent does the device accurately determine periods of arm use when measuring arm movements. Some types of arm use (e.g. holding a cup) are associated with as little movement as possible. In addition, not all movements are necessarily related to arm use, e.g. arm movements measured during walking and other whole-body movements are functionally different from arm movements during sitting or standing. This latter issue, in which arm use is generally overestimated, has been recognized in other studies. For example, Uswatte et al. (12) used the ratio of the affected and unaffected arm, assuming that movements during walking and whole-body movements affect both arms equally; this notion has also been applied by others (10, 11, 13). However, being able to remove arm movements due to walking would be a more reliable method to overcome this source of overestimating arm use. Therefore, our group developed and validated a device (the Vitaport ULAM (14)) that combines the movement intensity of the arms with data on body posture and movements (hereafter called “posture/movements”). This additional information allows walking to be detected and, based on this information, to separate arm movement during walking from arm use. Rand & Eng (15, 16) also used such a configuration to eliminate activity counts of arm swing while walking.
Since the previously developed Vitaport ULAM is an expensive multi-sensor system; and, because it is not user-friendly for patients to wear, and for therapists to analyse the data, it is not practical for use in daily life. To overcome these issues, but to still objectively measure arm use combined with posture/movements in daily life, a new clinically applicable and easy-to-use arm use monitor is required. In a previous study, we showed that measuring posture/movements in people after stroke with the Activ8 Physical Activity Monitor (Activ8) resulted in a >95% accuracy for the “upright position” and >90% accuracy for “lying/sitting and bicycling”1. The Activ8 is a simple, single-sensor, low-cost accelerometer that is suitable for use in daily life (17). In the present study we used the functionality of the existing Activ8, placed on the front of the unaffected thigh, combined with 2 additional Activ8s, one on each arm; this new configuration was called the “Activ8 arm use monitor” (Activ8-AUM).
The aims of the present study were to develop an algorithm to detect arm use with the Activ8-AUM, and to assess the validity of this new device and algorithm to detect arm use in people after stroke.
1Fanchamps, et al. Accuracy of detection of body postures and movements using a physical activity monitor in people after stroke.
The present study included people after stroke with mobility problems in the arm, leg, or both, aged between 18 and 75 years. People after stroke were excluded when mobility problems were not caused by the stroke, or when they had insufficient communication skills or cognitive function to understand instructions. To ensure safe participation, people after stroke with a Functional Ambulation Category score <3 (18) were also excluded. Between October 2015 and February 2016, eligible people after stroke were recruited (from Rijndam Rehabilitation (inpatients, outpatients and ex-patients)), Rotterdam, The Netherlands via their physiotherapist or were approached by letter via their treating physician. For screening, the clinical expertise of the individual’s physical therapist or physician was used. All participants provided written informed consent. The study was approved by the Medical Ethics Committee of Erasmus MC University Medical Center Rotterdam (MEC 2015-211).
A total of 25 people after stroke were included: 22 males and 3 females, mean age 56 years (standard deviation (SD) 12 years). These participants had a mean post-stroke time of 15 months (SD 14); 10 participants had a haemorrhagic stroke, and 11 were affected on the right side. Arm function was measured with the Frenchay Arm Test (scores 0–5, with higher scores indicating better function) (19): 14 participants had a score of 0 or 1, 1 participant had a score of 2, and 10 participants had a score of 4 or 5.
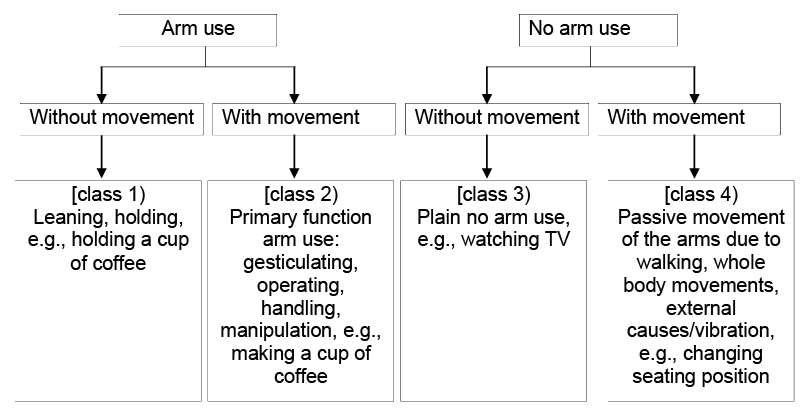
For this study, the theoretical starting point was the framework for arm use, as defined by Schasfoort et al. (20). According to this framework, arm use is defined as “active movement of parts of the arm, holding objects or leaning” (Fig. 1). This framework also shows that arm use is conceptually not the same as arm movement, and reveals the challenges and limitations of measuring arm use with accelerometry. For example, arm use can occur without much movement (e.g. when holding a cup; Fig. 1, class 1). On the other hand, arm movement is not necessarily related to arm use, e.g. arm movements that are primarily the result of whole-body movements, such as changing sitting posture (Fig. 1, class 4). In Schasfoort et al.’s framework (20), arm movement during walking is considered to be secondary use. In the present study, we focus only on primary use, assuming that this occurs only during sitting or standing. Therefore, analysing arm data during walking was beyond the scope of this study.
Fig. 1. Different classes of arm use showing the relationship between arm use and arm movement.
A measurement protocol was designed (Table I) that included activities mainly encompassing 1 of the first 3 classes of Fig. 1. Although no activities with class 4 as a major part of the activity were included, this class was expected to occur during other activities. Measurements were performed at a rehabilitation clinic or at the participant’s home. Each specific activity lasted approximately 80 s; however, especially at the participant’s home and during complex activities with an arm task, the duration of some activities could be shorter (e.g. if the activity was completed) or longer (e.g. kitchen activities). The total protocol lasted for a maximum of 1 h (including rests between activities). During lying, sitting and standing without an arm task, participants were instructed to stay as still and comfortable as possible. During all other activities, they were instructed to perform the activity at a comfortable, self-selected pace and use their own movement strategy. Any activities that appeared to be too difficult for an individual were excluded from the protocol. For safety reasons, participants stated their own physical limits, and supervision was available during all measurements. However, to ensure that activities were performed as “normally” as possible (to reflect everyday life), the supervision was kept as unobtrusive as possible.
Table I. Activities of daily life included in the measurement protocol
The Activ8-AUM consists of 3 Activ8s (2M Engineering, Valkenswaard, The Netherlands) (17): one on the front of the unaffected thigh, and one on each wrist (Fig. 2). All sensors are easy to attach: those on the wrists are worn dorsally (like a watch) and attached with a wristband. The sensor on the leg is attached (with skin tape while sitting) to the front of the leg approximately halfway between the hip and the knee. The concept of the Activ8-AUM is similar to that of the Vitaport ULAM used by Schasfoort et al. (14), which has sensors on the wrists, chest and legs, and combines the movement intensity of the arms with data on posture/movements to calculate arm use.
Fig. 2. Placement of the 3 Activ8s of the Activ8 arm use monitor (Activ8-AUM) device.
The Activ8 contains a triaxial piezoelectric crystal accelerometer and was originally designed as a single-sensor device to wear on the leg or in a trouser pocket. It measures posture/movements (lying/sitting, standing, walking, cycling, running, and non-wear) as well as their movement intensity (expressed in the arbitrary unit movement counts). Detection of posture/movements is based on the angular position of the sensor and the movement intensity, whereas movement intensity is based on the variability around the mean of the raw acceleration signal. Raw acceleration signals are measured at 12.5 Hz and converted to posture/movements with a resolution of 1.6 Hz. Data were stored with the smallest possible epoch (5 s), resulting in 8 samples per epoch for posture/movements. For each epoch the movement counts were calculated per detected posture/movements. The internal clock used a 32 kHz watch crystal (20 ppm), resulting in a max clock drift of 2 s per 24 h.
To be able to measure arm use, 2 additional Activ8s were used (1 on each wrist). In the analyses, only the movement intensity data from these 2 sensors were used. For this, the movement counts of the detected posture/movements were summed per wrist sensor to a single value for each 5-s epoch per arm, representing the total movement intensity of that arm during those 5 s. Therefore, the smallest unit for which the data could be analysed was an entire epoch of 5 s.
A handheld digital video camera was used to record all activities; this served as the reference method. Each second of the video was classified based on the classes described in Fig. 1: (i) arm use without movement; (ii) arm use with movement; (iii) no arm use without movement; and (iv) no arm use with movement. To do this, criteria for the different classes were developed, extensively discussed and tested. Arm use was defined as voluntary, purposeful activity of the arm, related to active movement of the arm, holding objects or leaning. Movement was defined as at least an observable movement of the wrist with a minimal duration of 1 s; this meant that a minor finger movement or a movement lasting only a fraction of 1 s was not assigned as movement. These 2 definitions were combined to classify the 4 classes mentioned above. If a classification was ambiguous, a second researcher was asked to analyse this part of the measurement. In cases of no agreement a third observer was involved. Both arms were scored separately, because the classification of both arms was not necessarily the same during 1 s. Thereafter, the 1-s 4-class classification was converted to a 5-s 2-class classification to be comparable to the 5-s dichotomous output of the Activ8-AUM, i.e. arm use and no arm use. First, classes 1 and 2 of the 1-s classification were re-coded to arm use and classes 3 and 4 were re-coded to no arm use. Then, the majority of the samples within an epoch determined the classification for the entire epoch, either as arm use or no arm use.
As mentioned, the Activ8-AUM combines the movement intensity of the arms with data on posture/movements from the leg sensor. The Activ8-AUM is based on the assumptions that: (i) arm use occurs only during sitting and standing, and (ii) arm use is associated with a movement intensity above a certain level. The second assumption requires the definition of an optimal movement intensity threshold. To do this, half of the data were selected as a development dataset, and the other half were used to validate the Activ8-AUM. The detection of posture/movements and calculation of the movement counts was performed with the standard Activ8 software. These data were the input for an in-house MATLAB programme detecting arm use.
First, the data on posture/movements from the leg sensor were combined and time-synchronized with the data on movement intensity from the arm sensors and with the video data. Synchronization of the sensors was based on the time stamps within the data files, using the “synchronize” function of MATLAB. The second step was selecting epochs of lying/sitting and standing, based on the posture/movements data from the leg sensor. An epoch was selected as lying/sitting when at least 5/8 samples within the 5-s epoch were determined as lying/sitting. The same holds for standing, when at least 5/8 samples had to be determined as standing for an epoch to be selected as standing. To fulfil the second assumption of the Activ8-AUM mentioned above, in the development dataset 4 movement intensity thresholds were determined, for the following situations: (A) unaffected arm during lying/sitting; (B) affected arm during lying/sitting; (C) unaffected arm during standing; (D) affected arm during standing. Although the protocol was carefully planned, such an imposed protocol probably has a different ratio of arm use and no arm use from that in daily life. This different ratio might affect the optimal movement intensity threshold. Therefore, our data were adjusted to create a ratio comparable to that established earlier in the daily life of people after stroke (6). To establish the optimal movement intensity threshold for each of the 4 situations mentioned above (A–D), thresholds were systematically changed between 1 and 40 movement counts, in steps of 1. Within each of the 4 situations, arm use was determined based on all possible thresholds (0/1, no arm use/arm use) and was compared with the 2-class classification of arm use according to the video data. To determine the accuracy of each threshold per situation, Youden’s index (21) was calculated as follows:
Youden’s index = sensitivity + specificity - 100
In this, sensitivity was defined as:
and specificity was defined as:
For each situation listed above (A–D), the movement intensity threshold with the highest Youden’s index was chosen as the value for the movement intensity above which that period of time was classified as arm use.
To validate the Activ8-AUM the optimal movement intensity thresholds, determined in the development dataset, were applied to the validation dataset. Again, arm use according to the Activ8-AUM was compared with arm use according to the video data (both dichotomous measures: arm use/no arm use). Sensitivity, specificity, and agreement were then calculated overall and for different groupings of the data: per limb, per class of Fig. 1, and per activity of the protocol. Agreement was defined as:
When calculating the outcomes for each activity in the protocol, no arm use was expected in activities without an arm task, and arm use was expected only in activities with an arm task. However, since the video recordings were used as the gold standard, it is possible that some arm use appeared in activities without an arm task, and sometimes no arm use occurred in activities with arm tasks. Therefore, both sensitivity and specificity were calculated per task, provided that arm use or no arm use appeared for a sufficient length of time, i.e. more than 60 s (12×5-s epochs).
Six participants (relatively early after stroke onset) who were unable to perform all the activities in a first session, agreed to participate in an additional session later on during rehabilitation; for these participants, both sessions were used for analysis. The total group of 31 measurements was divided into 2 datasets; a development dataset with 16 measurements and a validation dataset with 15 measurements.
Fig. 3 presents the movement counts for different activities of the development dataset. For both the affected and unaffected arm, the median movement counts of activities without an arm task were low compared with those with an arm task, indicating that a threshold could be set for discriminating between these situations. However, the interquartile range was relatively large for all activities, indicating that the intensity of arm use and no arm use differed between and within participants, and that an overlap in movement counts existed between arm use and no arm use. For the affected arm, median movement counts were smaller than for the unaffected arm, with the largest difference during standing.
Fig. 3. Median movement counts (25th to 75th percentile) per activity for the unaffected and affected arm. Note: the first 3 activities are subcategories of lying/sitting, the remainder are subcategories of standing. Horizontal lines indicate the movement intensity thresholds above which an epoch is classified as arm use (black for the unaffected and grey for the affected arm). The 75th percentile for throwing a ball with the unaffected arm was 94 counts.
The overlap in movement counts between arm use and no arm use showed that it was not possible to define a threshold for detecting arm use with 100% accuracy. Based on the highest Youden’s index, 4 movement intensity thresholds defining arm use were determined: for both standing and lying/sitting activities, separately for the affected and unaffected arm (Fig. 3: see horizontal lines). Table II shows that, after applying these thresholds in the development dataset, the sensitivity, specificity, and agreement between the Activ8-AUM data and the video data were all 74% or higher.
Table II. Data on sensitivity, specificity, and agreement in total time between Activ8 arm use monitor (Activ8-AUM) and video recording in the development dataset and validation dataset
Table III shows the number of epochs, the sensitivity, specificity, and agreement between the Activ8-AUM and the video of the validation dataset for the different groupings of data. Table II directly compares these variables in the development and validation dataset. The validation dataset contained 2,802 5-s epochs for the unaffected arm and 2,557 5-s epochs for the affected arm, which corresponds to ≥3.5 h of measurement. Overall, detecting arm use had a sensitivity of 73% and a specificity of 77%. In cases in which arm use was incorrectly classified, it was classified as arm use or no arm use depending on what was classified, since the Activ8-AUM has a dichotomous output. When evaluating the validity per class of Fig. 1, or per activities of the protocol, the accuracy was consistent, but with some important exceptions. “Arm use without movement” (class 1) was frequently detected incorrectly, especially in the unaffected arm (sensitivity unaffected arm: 24%; affected arm 42%). An example of this is holding onto the table during standing, which is arm use without movement but which was often incorrectly classified as no arm use. Also “no arm use with movements” (class 4) was less accurately detected (specificity unaffected arm: 53%; affected arm: 64%). As expected, when comparing the validity between the development and validation dataset, the sensitivity, specificity and agreement was max. 12% lower, although 2 values were higher, max 10% (Table II, validation dataset).
Table III. Data on sensitivity, specificity, and agreement in total time between Activ8 arm use monitor (Activ8-AUM) and video recording in the validation dataset
This study developed and validated the Activ8-AUM to measure arm use in people after stroke. This device consists of 3 simple, low-cost accelerometers (one on the unaffected thigh and one on each wrist). The device provides data on the movement intensity of the arms, and on posture/movements based on the leg sensor. Combining these different types of data allowed us to define body posture-specific movement intensity thresholds for arm use, and to separate arm movement during walking from arm movement during sitting and standing. In the validation part of the study, the Activ8-AUM showed similar results in detecting arm use as the previously developed Vitaport ULAM (20), which measured more detailed data on posture/movements and arm use. However, the Vitaport ULAM is not practical for use in daily life.
Arm use in people after stroke has also been measured by other groups. In the present study, the method of measuring arm use was conceptually similar to the approach of Schasfoort et al. (22) and Michielsen et al. (6) using the Vitaport ULAM, and to Rand & Eng (15) using accelerometers on the wrists and hip. Other studies used simpler sensor configurations, based on sensors on each wrist (10, 11, 13, 23–25). Besides measuring arm use in daily life, Lemmens et al. (26) focused on the detection of specific activities of daily living, such as “drinking from a cup” and “brushing hair”. For this they needed several accelerometers on the hand, wrist, arm and chest. Thus, most of the available devices do not use information on posture/movements or a movement intensity threshold; however, the effect of using this additional information and threshold has not yet been evaluated.
A general limitation of using accelerometry to quantify arm use is that not all arm movement should be considered as arm use and, vice versa, no arm movement is not necessarily an indication of no arm use. The Activ8-AUM also has this limitation: arm use was poorly detected during holding an object or leaning, when arms are displaced little or not at all (Table III, class 1). Also, no arm use was detected less accurately when the arm was moving (class 4). However, adding data on posture/movements was helpful in reducing this latter form of mistakes: arm movement during walking was not incorrectly classified as arm use, due to the known body movement of walking. However, during no arm use, arm movements due to slight general trunk movement during standing were still misclassified as arm use. This general limitation of accelerometry should not hamper future usage of the Activ8-AUM. Arm use that is difficult to detect with accelerometry (e.g. holding, leaning, small manipulations) is mainly preceded and followed by arm movements to bring the arm into the correct position. While, in people after stroke, less leaning and holding with the affected arm is expected, easily detectable arm movements will also be performed less often. Moreover, it is highly likely that arm movement and arm use are related (27). Therefore, although it is not possible to directly measure arm use with accelerometry, the amount of arm movements were considered a meaningful parameter.
In the development part of this study, 4 movement intensity thresholds were determined, above which an epoch is optimally classified as arm use. Four different thresholds were used to take into account the differences in movement intensity between lying/sitting and standing, and between the affected and unaffected arm. This approach was supported by the data: the optimal threshold for standing (when more body movement affecting arm movement can be expected) was higher than for lying/sitting. Also, the optimal threshold for the affected arm (associated with slower movements and lower movement intensities) was lower than for the unaffected arm. It should be noted, however, that the severity of a stroke will affect the movement and movement intensity of the affected arm. In the present approach, thresholds are based on group level data, which may be suboptimal for individuals. In the future, more individualized thresholds could be explored, e.g. using different thresholds for different levels of arm function based on standardized tests (e.g. the Frenchay Arm Test (19)).
To determine the 4 optimal movement intensity thresholds, Youden’s index was used because it combines sensitivity and specificity (21). We felt that, for our device, sensitivity and specificity are equally important and that, therefore, the highest sum of both is the best criterion to define the thresholds. An alternative criterion could have been the highest agreement; however, the benefit derived from the highest sum of both the sensitivity and specificity would then be lost. Moreover, our data showed that agreement was a less discriminative criterion, because several thresholds showed comparable optimal agreement percentages.
It is important to realize that sensitivity and specificity and, therefore, Youden’s index are influenced by the activities included in the protocol, and the ratio of arm use to no arm use. Thus, whether the 4 determined thresholds will be as optimal to measure arm use in daily life will depend on the extent to which the activities of daily life differ from those in the protocol, and the ratio of arm use to no arm use in daily life. To take this into account, our data were adjusted to create a ratio comparable to that established previously in people after stroke (6).
In the present study an overall agreement of 75% was found between the Activ8-AUM data and video data, which is comparable to the agreement scores of the previously developed Vitaport ULAM (20). That earlier system provided meaningful outcomes in several studies in people after stroke (6) and in patients with complex regional pain syndrome (22), which supports the conclusion that the agreement percentage of 75% is acceptable for application in descriptive and evaluative studies. However, the large individual difference in overall sensitivity, specificity, and agreement showed that movement intensity thresholds, which are based on group level data, are not optimal for all individuals. One reason for this is the ratio of arm use to no arm use. Although in the total group we adjusted our data to create a ratio comparable to that in daily life of people after stroke (6), the individual data still show a large difference in that ratio, especially in participants with low agreement scores. Inspection of specific activities showed that standing without arm task was often detected incorrectly. During standing, although no arm tasks were imposed, some participants were holding onto a table or a walking aid. In the video analyses this was scored as arm use (without movement, class 1), whereas the Activ8-AUM detected this as no arm use, due to the low movement intensity; this is a typical example of the above-described source of misdetection.
Some limitations of the study need to be addressed. First, one Activ8 was used on the thigh to detect posture/movements, in order to distinguish between lying/sitting, standing, and other body movements. This application of the Activ8 was previously validated to measure posture/movements in healthy persons2 and people after stroke3, and showed good discrimination between lying/sitting, standing, and other postures and movements. Nevertheless, detection of posture/movements is not flawless and might have influenced the periods in which arm use was determined. However, we expected this influence to be small, i.e. based on the accuracy of the Activ8, very few periods of actual lying/sitting or standing will be missed. A second limitation is that quantifying the reality (i.e. what actually happened) per second, based on the videos, was difficult and prone to subjective interpretation. To decrease this effect, classification of arm use was performed carefully, based on well-defined criteria for the different classes. Classification was first practiced and then performed by one researcher; agreement with a second researcher was obtained in cases of doubt.
2Horemans, et al. The Activ8 activity monitor: validation of posture and movement classification.
3Fanchamps, et al. Accuracy of detection of body postures and movements using a physical activity monitor in people after stroke.
This study developed a novel, clinically applicable, easy-to-use arm activity monitor. Acceptable agreement between the Activ8-AUM and the video recordings was reached for measuring arm use when a movement intensity threshold for the arm accelerations was combined with posture/movement data. In addition to this acceptable agreement, the Activ8-AUM has an easy-to-use configuration with 3 simple, low-cost, accelerometers placed on the leg and on both wrists. Therefore, the Activ8-AUM is a promising device for researchers and clinicians to measure arm use in people after stroke.
The authors thank all the people after stroke who participated in this study, Gerard M. Ribbers for his help in recruiting participants, and the students involved in the data collection.
The project was internally funded by Rijndam Rehabilitation.
All participants provided written informed consent. The study was approved by the Medical Ethics Committee of Erasmus MC University Medical Center Rotterdam.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize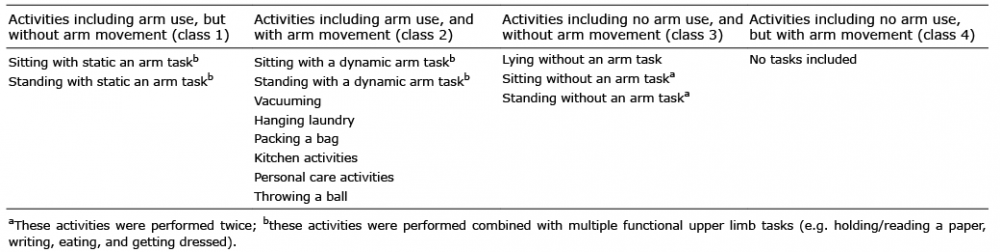 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize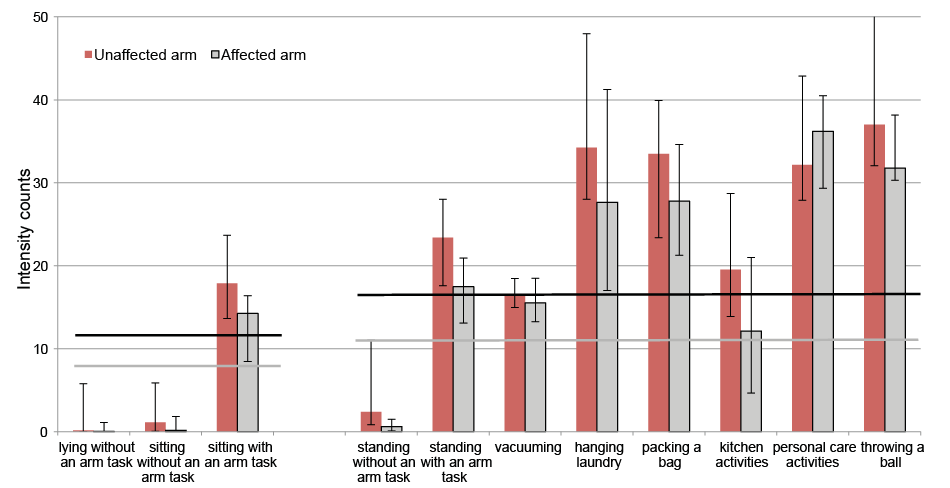 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize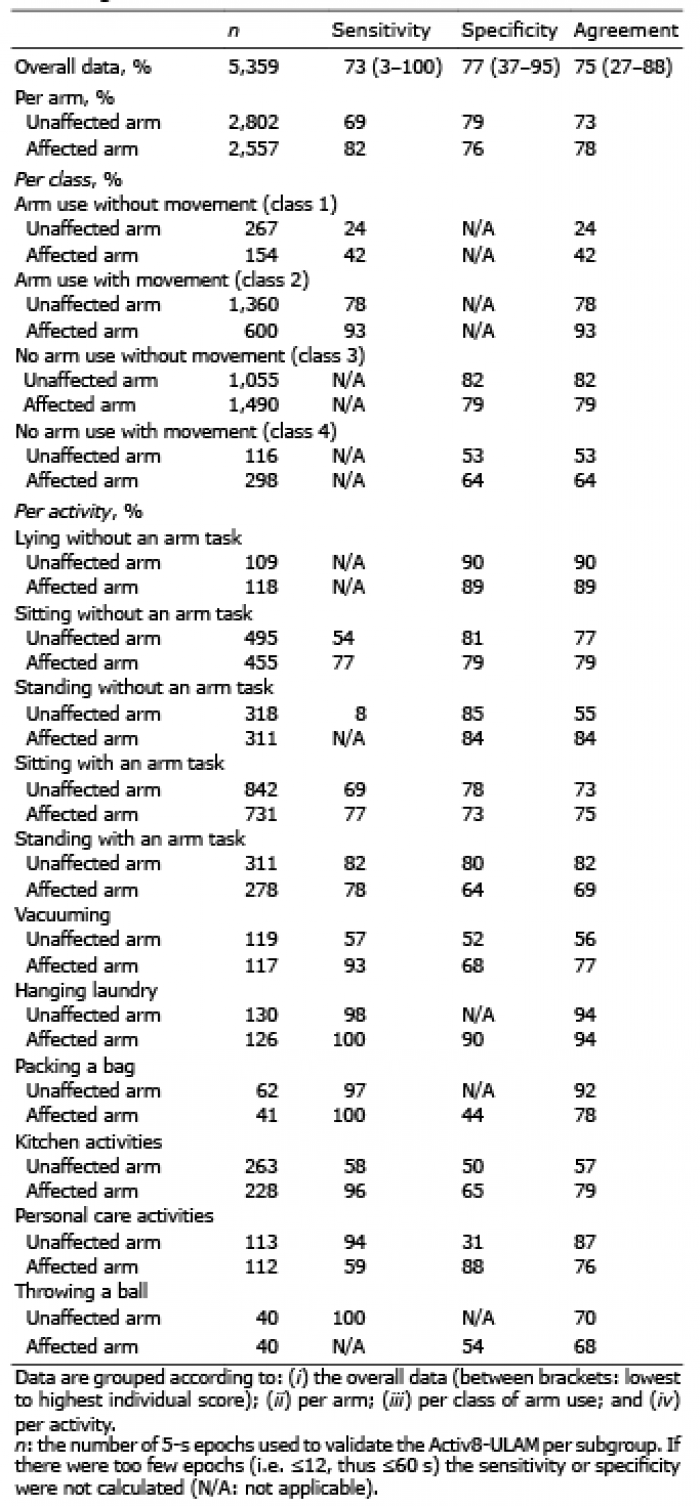 Click to show fullsize
Click to show fullsize