
From the 1Department of Health Sciences, Lund University, Lund, 2Department of Hand Surgery, Skåne University Hospital, Malmö, 3Department of Neurology and Rehabilitation Medicine, Skåne University Hospital, Lund, Sweden, 4Department of Health Science, Luleå University of Technology, Luleå, and 5Department of Neuroscience, Rehabilitation Medicine, Uppsala University, Uppsala, Sweden
Objective: To evaluate the test–retest reliability of the Life Satisfaction Questionnaire (LiSat-11) and the association between items in individuals with chronic stroke.
Design: Test–retest design.
Subjects: Forty-five individuals (mean age 65 years) with mild to moderate disability at least 6 months post-stroke.
Methods: LiSat-11, which includes 1 global item ”Life as a whole” and 10 domain-specific items, was rated on 2 occasions, one week apart. Test–retest reliability was evaluated by kappa statistics, the percent agreement (PA) and the Svensson rank-invariant method. The association between items was evaluated with the Spearman’s rank correlation coefficient (rho).
Results: The kappa coefficients showed good to excellent agreement (0.59–0.97) and the PA ≤ 1 point was high (> 89%) for all items. According to the Svensson method, a small systematic disagreement was found for “Partner relationship”. The other items showed no systematic or random disagreements. All domain-specific items, except one (“Sexual life”) were significantly correlated with “Life as a whole” (rhos 0.29–0.80).
Conclusion: LiSat-11 is considered reliable and can be recommended for assessing life satisfaction after stroke. The association between items indicates that LiSat-11 measures various aspects that can impact on an individual’s life satisfaction.
Key words: outcome assessment; psychometrics; rehabilitation; reproducibility of results; self-report; quality of life; stroke.
Accepted Apr 25, 2018; Epub ahead of print Aug 6, 2018
J Rehabil Med 2018; 50: 713–718
Correspondence address: Elisabeth Ekstrand, Department of Health Sciences, Physiotherapy Research Group, Lund University, Box 157, SE-221 00 Lund, Sweden. E-mail: elisabeth.ekstrand@med.lu.se
After stroke, the remaining physical and cognitive impairments that many individuals experience can affect their ability to perform activities and participate in society (1–3), which can contribute to reduced life satisfaction (4, 5). Therefore, an overarching goal in stroke rehabilitation is to improve an individual’s life satisfaction (6). Life satisfaction is related to concepts such as happiness and wellbeing and can be measured as how an individual perceives his or her life situation (6, 7). The level of satisfaction is affected by the individual’s expectations in life and thereby reflects how well aspirations and achievements are being met (8, 9).
One commonly used self-reported outcome measure to assess life satisfaction in rehabilitation is the Life Satisfaction Questionnaire (LiSat), developed and validated by Fugl-Meyer et al. (6, 10). LiSat consists of a global item “Life as a whole” and different domain-specific items, such as vocation, economy, leisure and social relations. LiSat is available in 2 versions; LiSat-9, which contains the global item and 8 domain-specific items (6) and LiSat-11, which includes 2 more domain-specific items regarding satisfaction with somatic and psychological health (10).
LiSat is frequently used to assess life satisfaction in studies of persons with stroke (5, 11–16). Despite this, there is limited knowledge about the reliability of LiSat. To the best of our knowledge no study has evaluated the test–retest reliability of LiSat-11 and only one study has evaluated LiSat-9 in persons with stroke (17). That study included a sample of different diagnosis, such as stroke, traumatic brain injury, tumours and infections (17). They found LiSat-9 to have relatively low reliability; however, the sample consisted of persons with aphasia and cognitive impairments and the ratings were obtained by post. Furthermore, no comprehensive analysis of the systematic and random disagreements (measurement variability) was performed.
In clinical practice and in stroke research, life satisfaction is often assessed by using only the global item “Life as a whole” (18–23). In the original study with LiSat-11 (10), the associations between the global item and the domain-specific items were evaluated in Swedish adults and significant correlations were found for all domain-specific items (Spearman’s rho 0.23–0.54). However, it is not known how well the global item is representative of the other 10 domain-specific items after stroke and there is limited knowledge of the test–retest reliability in this population.
The aim of this study was to evaluate the test–retest reliability, in terms of agreement and systematic and random disagreement, of the LiSat-11 in individuals with mild to moderate disability after stroke and to evaluate the association between items.
Forty-five community-dwelling individuals with stroke (ischaemic or haemorrhagic) were recruited to the study from April to December 2013. All participants had been diagnosed and treated at the stroke unit in a university hospital in southern Sweden. The participants had mild to moderate disability after stroke, i.e. 1–3 according to the modified Rankin Scale (mRS) (24), and were at least 6 months post-stroke. Before being included in the study potential participants were interviewed about their life situation and level of disability. Those who were unable to understand and follow test instructions due to communication or cognitive impairments were not included in the study.
Prior to inclusion, information about the study was provided and the individuals gave written informed consent to participate. The principles of the Declaration of Helsinki were followed and the study was approved by the Regional Ethical Review Board, Lund, Sweden (Dnr 2012/591).
The Life Satisfaction Questionnaire-11 (LiSat-11) (10) assesses how satisfied an individual is with different aspects of life. LiSat-11 consists of the global item “Life as a whole” and the following 10 domain-specific items: vocation; economy; leisure; contacts with friends and acquaintances; sexual life; activities of daily living (ADL) (ability to manage self-care in dressing, hygiene, transfers); family life; partner relationship, somatic health; and psychological health. The items are rated according to 6 response options: 1 = very dissatisfying; 2 = dissatisfying; 3 = rather dissatisfying; 4 = rather satisfying; 5 = satisfying; and 6 = very satisfying. Higher scores indicate a greater level of perceived satisfaction.
Participants rated the items in LiSat-11 during an interview performed on 2 occasions (test occasion 1, T1, and test occasion 2, T2), 1 week apart, under similar conditions, as recommended by the COSMIN standards (COnsensus-based Standards for the selection of health Measurement Instruments) (25). The interviews were performed at the same place (a quiet, separate room in the hospital), by the same interviewer (first author) and at the same time of day. The interview took approximately 10 min to complete.
Prior to the interview the individuals were asked about their age, social and vocational situation, walking ability indoors and outdoors, whether they used walking aids, and whether they experienced shoulder pain or fatigue after their stroke. Furthermore, the individuals rated their perceived muscle strength in the affected side and their perceived participation according to the Stroke Impact Scale (SIS; domains 1 and 8, respectively). The interviewer also rated the level of disability according to the mRS. Data on time since stroke onset, type of stroke and side of paresis were verified from the medical records
Descriptive statistics, such as means, standard deviations (SD), frequencies, median and maximum and minimum (min–max) values, were calculated for demographics and clinical characteristics of the participants.
The test–retest reliability of each item in LiSat-11 (ordinal scale 1–6) was evaluated by kappa statistics (quadratic weights) (26–28), the percent agreement (PA) and the Svensson rank-invariant method (29). The kappa coefficients (the proportion of agreement observed beyond the agreement expected by chance) (26) were used to evaluate the agreement between the paired scores of T1 and T2. The strength of the kappa coefficient was interpreted as < 0.40 poor, 0.40–0.75 fair to good, and > 0.75 excellent (30).
The PA was used to evaluate the agreement as the proportion of individuals that had rated the same score or ± 1 point (PA ≤ 1 point) at T1 and T2. The Svensson method was used to evaluate whether there was disagreement, i.e. lack of agreement, in the test–retest ratings. Disagreement was evaluated as the relative position (RP) and the relative rank variance (RV) (29). The RP determines whether there is a systematic disagreement, i.e. a systematic shift of ratings to higher or lower scores. Possible RP values range from –1 to 1 and zero values indicate a lack of systematic disagreement. A positive RP value indicates that the participants had higher scores on T2 than on T1. The RV is a measure of the random disagreement and ranges from 0 to 1. A RV value larger than zero indicates the presence of random disagreement and the higher the RV value the more dispersed are the test–retest ratings. The RP and RV values were calculated together with a 95% confidence interval (95% CI); a statistically significant disagreement was indicated by a 95% CI not covering zero.
Spearman’s rank correlation coefficients (rho) were calculated to evaluate the association between the global item ”Life as a whole” and the 10 domain-specific items. The correlations were calculated on data from the first test occasion. The strength of the correlations was interpreted as: rho < 0.3 negligible; 0.3 to < 0.5 low; 0.5 to < 0.7 moderate; 0.7 to < 0.9 high; and ≥ 0.9 very high (31).
Data were analysed with IBM SPSS Statistics version 23 (IBM Corp., Armonk, New York, USA), the kappa coefficients by the MedCalc, version 15 (www.medcalc.org) and the Svensson method by the Elisabeth Svensson program (www.oru.se/esi/svensson). Probability values less than 0.05 were considered statistically significant.
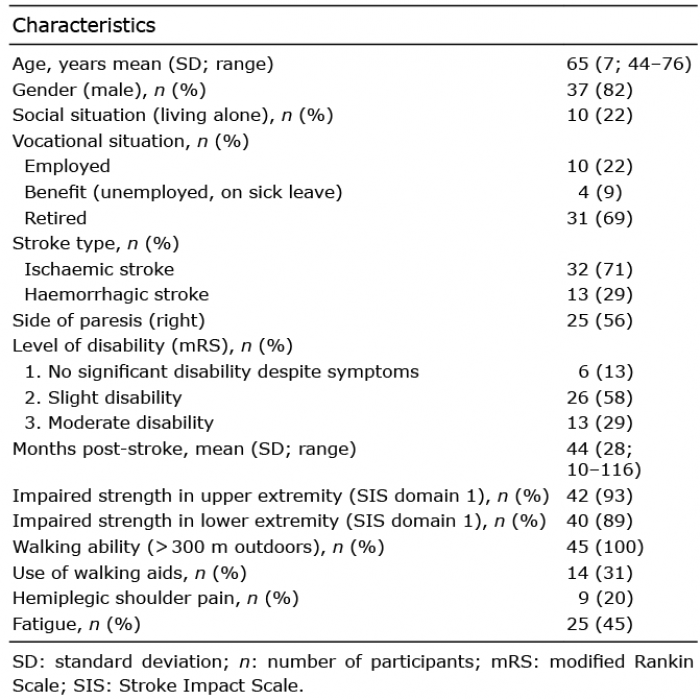
The clinical characteristics of the 45 participants (8 women, 37 men) are shown in Table I. Their mean age was 65 years and the majority were retired and lived with another person. Most of them had a mRS level of 2, indicating slight disability, and the mean time since stroke onset was 44 months. All participants were able to walk independently outdoors, and approximately one-third used a walking aid.
Table I. Characteristics of participants with chronic stroke (n = 45)
Table II shows the distribution of the frequencies of the item scores of LiSat-11 at T1 and T2, together with the median, minimum and maximum values. For most items the participants used all response options of the scale (1–6) with the exception of items ”ADL” and ”Family life”, where only 4 response options were used (3–6). For the item “Somatic health” most response options were used (2–6), but the majority of participants rated the item as “Rather satisfying” (response option 4).
Table II. Distribution of the frequencies of the item scores of Life Satisfaction Questionnaire (LiSat-11) on the first and second test occasion (n = 45)
Table III shows the test–retest reliability of each item score of LiSat-11. The kappa coefficients ranged from 0.59 to 0.97. Most items had a kappa coefficient larger than 0.75, except ”ADL”, ”Family life”, ”Somatic health” and ”Psychological health”, where the kappa coefficients ranged from 0.59 to 0.73. The PA ≤ 1 point ranged from 89% to 100% for all items. According to the Svensson method, no significant systematic or random disagreements, were found except for “Partner relationship”, which showed a small negative change in RP, i.e. the participants systematically rated the item with lower scores at T2.
Table III. Test–retest reliability of each item of the Life Satisfaction Questionnaire (LiSat-11) (n = 45)
Table IV shows the correlations between the global item ”Life as a whole” and the 10 domain-specific items. All domain-specific items except 1 (”Sexual life”) were significantly correlated with ”Life as a whole”. The highest correlations were found for the items ”Psychological health” (rho = 0.80), ”Contacts with friends and acquaintances” (rho = 0.69) and ”Leisure” (rho = 0.62). The items ”Sexual life”, ”Family life” and ”Economy” had the lowest correlations with ”Life as a whole” (rho = 0.29–0.34).
Table IV. Association between global life satisfaction and the 10 domain-specific items in Life Satisfaction Questionnaire (LiSat-11) (n = 45)
The main findings of this study are that the scores of the 11 items in LiSat-11 showed good to excellent agreement based on the kappa coefficients. For all items the PA≤ 1 point was high (> 89%) and no item, except 1, showed any systematic or random disagreement according to the Svensson method. All domain-specific items, except one, were significantly correlated with “Life as a whole”.
The kappa coefficients of LiSat-11 in our study were generally higher than in the previous study of LiSat-9 in individuals with acquired brain injuries (stroke, traumatic brain injury, tumours and infections) (17). These authors reported kappa coefficients of 0.34 to 0.69 compared with 0.66–0.97 (items 1–9) and 0.59–0.73 (items 10 and 11) in the present study. However, their sample included individuals with more severe cognitive impairments and aphasia and the ratings were collected by post, to which the participants responded by themselves or with help from another person (17). The differences in results indicate that LiSat might be more suitable for individuals with mild to moderate stroke and that the ratings are more reliable if they are collected through an interview.
To evaluate the agreement between the 2 test occasions and to be able to compare these data with previous studies, kappa coefficients were used in the present study. However, kappa coefficients have limitations when the ratings are concentrated in few response options (32). This was, in fact, the case for the items “ADL”, “Family life” and “Somatic health”, which automatically yielded lower kappa values.
To expand the reliability analysis the LiSat-11 was also evaluated by the PA and the Svensson method. The PA ≤ 1 point was high for all items. No items showed any significant systematic or random disagreement, except “Partner relationship”, which showed a small systematic disagreement. However, “Partner relationship” showed a high kappa value and high PA≤ 1 point. Taken together, the current results indicate that LiSat-11 could be considered reliable and recommended for use in assessing life satisfaction in individuals with mild to moderate disability following stroke.
In the present study all items except 1 (”Sexual life”) were significantly correlated with ”Life as a whole” and the strength of the correlations ranged from low to high. The strongest correlations were found for ”Psychological health” (rho = 0.80), ”Contacts with friends and acquaintances” (rho = 0.69) and ”Leisure” (rho = 0.62), whereas the lowest correlations were found for ”Economy” (rho = 0.35) and ”Family life” (rho = 0.32). These results are partly in agreement with the study of Fugl-Meyer et al. (10), who also found the highest correlation between the global item and ”Psychological health” (0.52), and that the item ”Economy” had one of the lowest correlations. Furthermore, these authors found higher correlations for ”Family life” (rho 0.50) and ”Partner relationship” (rho = 0.50) than we did. However, they included approximately 2,500 persons, 18–64 years of age, whereas most participants in our study were older than 64 years and retired. Therefore, it is difficult to fully compare the results.
Nevertheless, the current results indicate that there are individual variations regarding the degree of importance that different domains have for a person’s life satisfaction. Even if some aspects of life show low levels of satisfaction this will not necessarily be reflected in the global item. The association between the global item ”Life as a whole” and the domain-specific items can be seen either as a ”top-down” or a ”bottom-up” model. From a ”top-down” perspective the global item can be seen as a disposition, i.e. an individual who is satisfied with his or her life as a whole tends to be satisfied with the other life domains. On the other hand, from a ”bottom-up” perspective, an individual who is satisfied with the different life domains tends to be satisfied with life as a whole (10). To further understand the underlying construct of LiSat-11, a Rasch analysis and validation using a larger sample would be valuable. Also, a fit to the Rash model would enable the use of total sum scores of the LiSat-11.
A strength of this study is that all participants were in a stable phase after stroke and the data were collected according to the COSMIN standards (25). Furthermore, 45 participants were included, which can be considered sufficiently large when the reliability of an outcome measure is evaluated (33). However, more men than women participated, thus the results cannot be generalized to the entire stroke population. Also, as the test–retest data were obtained under standardized test conditions (same location, at the same time of the day and with the same time interval), it may not reflect a real clinical situation.
LiSat-11 is reliable and can be recommended to assess
life satisfaction after stroke. The association between the global item “Life as a whole” and the domain-specific items indicates that LiSat-11 measures various
aspects that can impact on an individual’s life satisfaction.
The authors would like to thank the individuals who volunteered to participate and to RPT, Michael Miller, PhD, for revision of the English language. The study was supported by grants from the Swedish Stroke Association, Vårdakademin at Skåne University Hospital, the Norrbacka Eugenia Foundation, Skåne county council’s research and development foundation and the Faculty of Medicine at Lund University.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize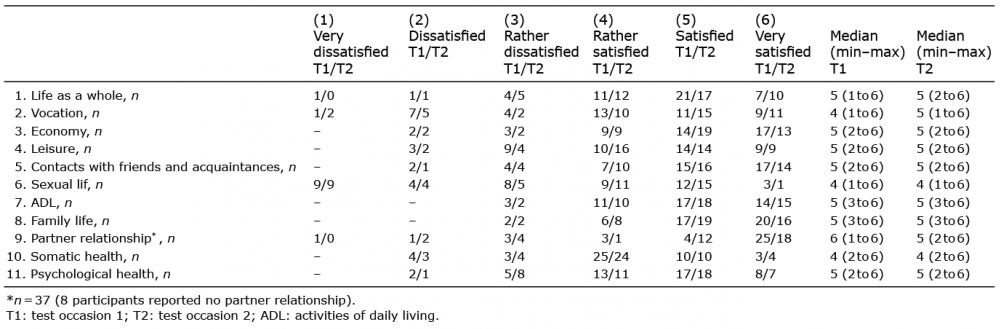 Click to show fullsize
Click to show fullsize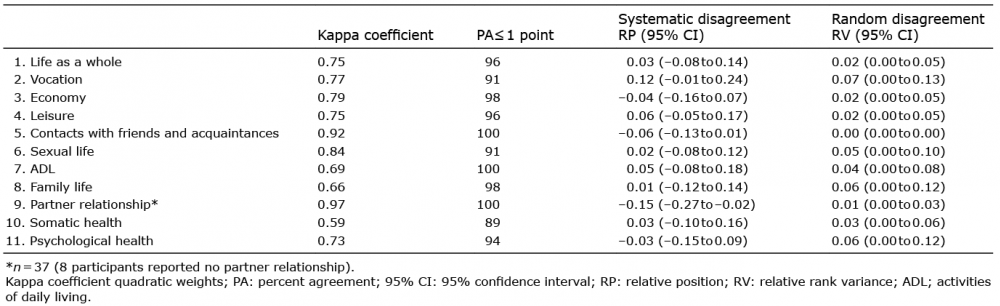 Click to show fullsize
Click to show fullsize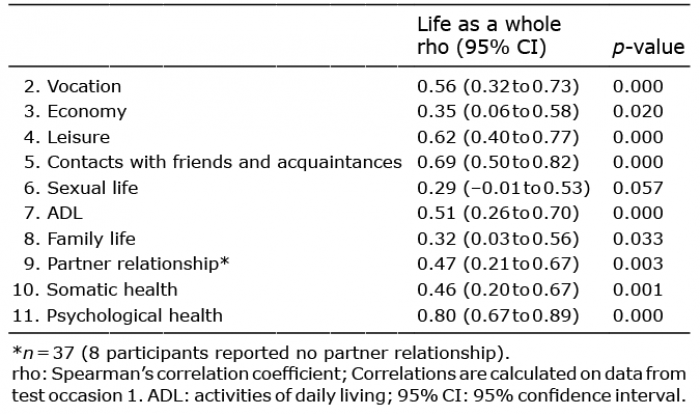 Click to show fullsize
Click to show fullsize