
From the Departments of Rehabilitation Medicine, 1School of Medicine, Chungnam National University, Daejeon, 2Department of Rehabilitation Medicine, Konkuk University School of Medicine and Konkuk University Medical Center, 3Department and Research Institute of Rehabilitation Medicine, Yonsei University College of Medicine, Seoul, 4Department of Physical and Rehabilitation Medicine, Chonnam National University Medical School, Gwangju, 5Department of Rehabilitation Medicine, Pusan National University School of Medicine, Pusan National University Yangsan Hospital, Busan, 6Department of Preventive Medicine, Wonkwang University School of Medicine, Iksan, 7Department of Rehabilitation Medicine, Kyungpook National University School of Medicine, Kyungpook National University Hospital, Daegu, 8Department of Rehabilitation Medicine, Wonkwang University School of Medicine, Iksan, 9Department of Rehabilitation Medicine, Jeju National University Hospital, Jeju National University, School of Medicine, Jeju, 10Department of Physical and Rehabilitation Medicine, Center for Prevention and Rehabilitation, Heart Vascular Stroke Institute, Samsung Medical Center, Sungkyunkwan University School of Medicine, 11Department of Health Science and Technology, Department of Medical Device Management & Research, SAIHST, Sungkyunkwan University, Seoul, Republic of Korea
Objective: To identify contributing factors that can be used to predict which patients with first-ever stroke will return to driving during 1 year after stroke.
Design: Multicentre cohort study.
Subjects: A total of 620 first-ever stroke patients who drove before stroke.
Methods: The Stroke Cohort for Functioning and Rehabilitation is a large, multicentre, prospective cohort study of all patients with acute first-ever stroke admitted to participating hospitals in 9 areas of Korea.
This study analysed the data from 1,354 patients who completed a face-to-face survey about return to driving at 1 year after stroke. A multiple binary logistic regression analysis model was used to analyse factors that potentially influenced return to driving during 12 months after stroke.
Results: Of 620 subjects, 410 (66.1%) returned to driving after stroke. They resumed driving at a mean of 2.15 months after stroke (standard deviation 2.32 years). Regression models showed that sex, age, modified Rankin scale (mRS), education about return to driving, and Fugl-Meyer Assessment (FMA) were significantly related to return to driving. Stroke type, ambulatory function, and language function at 7 days were not correlated with return to driving.
Conclusion: Male patients, education about return to driving, lower mRS, and higher FMA at 7 days after stroke are predictors of return to driving. This model could be used by clinicians to help counsel patients and their families.
Key words: stroke; automobile driving; rehabilitation; activities of daily living; cohort study; quality of life.
Accepted May 30, 2018; Epub ahead of print Sep 5, 2018
J Rehabil Med 2018; 50: 800–805
Correspondence addresses: Yun-Hee Kim, Department of Physical and Rehabilitation Medicine, Center for Prevention and Rehabilitation, Heart Vascular and Stroke Institute, Samsung Medical Center, Sungkyunkwan University School of Medicine, Department of Health Science and Technology, Department of Medical Device Management & Research, SAIHST, Sungkyunkwan University, 50 Ilwon-dong, Gangnam-gu, Seoul 135-710, Republic of Korea. E-mail: yunkim@skku.edu, yun1225.kim@samsung.com; and Min Kyun Sohn, Department of Rehabilitation Medicine, School of Medicine, Chungnam National University, Daejeon, Republic of Korea. E-mail: mksohn@cnu.c.kr
In terms of social participation, ability to drive is one of the most important activities for stroke survivors. However, it is difficult for healthcare providers to predict and provide guidance about return to driving during the early phase of stroke. Various predictive factors for return to driving were analysed among 620 patients with mild first-ever stroke. Sex, motor deficit, and stroke severity at 7 days after stroke were significant predictors for return to driving at 1 year after stroke. Using the Fugl Meyer Assessment score and the National Institutes of Health Stroke Scale, clinicians may be able to screen for stroke patients who have high probability of returning to driving at an early phase of stroke. This study may help healthcare professionals to advise stroke patients and their families concerning the likelihood of returning to driving.
Stroke is a major cause of disability worldwide, affecting participation in daily activities and social roles (1–3). In recent decades, there has been an increase in stroke survival rate, which has resulted in an increase in the number of people with perceptual and cognitive deficits (4). Stroke can have a spectrum of deficits that may influence patient’s driving skills, including reduced visual fields, visual scanning, attention, information processing speed, physical abilities, and visuospatial skills (5–9). These deficits can result in a reduction in on-road driving abilities (10, 11).
However, stopping driving can result in depression, reduced social connectedness, and increased risk of entry to long-term care, which is not surprising, as lack of access to transportation is associated with reduced access to social participation and healthcare (12–15). Inability to drive may affect a person’s ability to travel to work, and to undertake everyday tasks, such as shopping and visiting out-patient department clinics, and it can be regarded as symbol of dependence and lack of freedom (16, 17).
Driving is an extremely complicated task requiring many functional abilities that may be affected by a stroke (18). These functional abilities generally fall into 3 domains: motor (e.g. turning the steering wheel, using foot pedals, turning on windscreen wipers), visual-perceptual (e.g. recognizing traffic signs, noticing events in the periphery of vision, parking between lines) and cognitive domains (e.g. being aware of the speed limit, knowing the directions to the destination, planning and assessing safety in merging and changing lanes) (19). It is difficult to ascertain which patients will return to driving. Knowing what characteristics may predict returning or not returning to driving is important for physicians, social workers, and rehabilitation professionals involved in the care of stroke survivors. Studies have found that 30–66% of patients return to driving after a stroke (20–23). Non-returners are generally more disabled than returners, based on total Functional Independence Measure (FIM) scores, modified Barthel Index scores, and arm function tests (16, 24).
Pre-stroke driving frequency, post-stroke Barthel Index, and marital status have been shown to have predictive value for return to driving at 6 months post-stroke in people with ischaemic stroke (20). Stroke Impact Scale and Mini-Mental State Examination scores measured at 3 months post-stroke and stroke type have been shown to be predictive for return to driving at 1 year (21). Both of these studies used samples from acute hospital settings, thereby including patients with a wide range of stroke severity and functional deficits. These studies measured the independent variables at 3 months in Western countries. Thus, there is need to analyse patients in Asian countries and to perform early measurement of independent variables for return to driving. Our search did not reveal any studies of prediction of return to driving in South Korea or any other Asian country. Therefore, this is the first and large sample-sized study based on a stroke cohort in Asia. The aim of this study was to identify initial clinical factors that predict return to driving and to explore the current situation of return to driving after first-ever stroke in Koreans during the 12 months after stroke.
the Korean Stroke Cohort for functioning and rehabilitation (KOSCO), which is a partnership among 9 tertiary grade university hospitals in the Republic of Korea (25). KOSCO, designed as a 10-year long-term follow-up study of stroke patients, is a prospective multi-centre project investigating the factors that influence residual disabilities, activity limitations, and long-term quality of life in patients who have had a first-time stroke. The cohort collects demographic and clinical data from participants who have a primary diagnosis of first-ever stroke including residual disabilities, activity limitation, and quality of life. Ischaemic and haemorrhagic strokes are included, but transient ischaemic attacks are excluded. The detailed rationale and protocol of KOSCO has been described previously (25). Written informed consent was obtained from all patients prior to inclusion in the study, and the study protocol was approved by the local ethics committee at each hospital.
This study presents the interim results of KOSCO for evaluating the functional levels of first-time stroke patients at 12 months after onset. The data at 12 months after stroke onset in patients (n = 3,738) who were recruited to KOSCO from August 2012 to July 2015 were analysed. Data on normal cognitive function at 12 months with a Korean Mini-Mental State Examination (K-MMSE) score of more than 24 were included for further analysis (26). This indicates that the answers for return to driving are valid and reliable. Among the included patients (n = 1,594), the data were analysed for patients (n = 620) without missing values who were driving before stroke.
Independent variables were selected from the database with regard to previous literature, data availability, and clinical judgement. These variables included demographics such as age, sex, driving education, stroke type (infarction vs haemorrhage), National Institutes of Health Stroke Scale (NIHSS), Korean Version of Frenchay aphasia screening test (K-FAST), Functional Ambulatory Category (FAC), FMA of affected side, and modified Rankin scale (mRS) (21, 27).The clinical measures represent a range of impairments in motor (FMA, FAC), attention (NIHSS), language (K-FAST), and disability level (mRS). All clinical measurements were collected at 7 days after stroke during the acute care stay.
KOSCO participants were contacted at outpatient clinics or by visiting a patient’s home at 12 months after stroke to complete a follow-up survey that included questions about their driving status. This survey can be answered only by the patients or primary caregivers. The survey questions of interest for this study were “Did you drive before stroke?”, “Have you been instructed about driving after stroke? (driving education)”, and “Have you restarted driving your car?” The participant could answer “yes” or “no.”
After excluding non-drivers, answers to the third question were used to determine return to driving. Variables were then compared across the 2 groups of interest, returners and non-returners, using the appropriate statistical hypothesis test (independent samples t-test or χ2 test) to search for significant differences that may be predictive of return to driving. Candidate independent variables to be placed in the binary logistic regression (BLR) model were then selected from all the variables (listed above) using the results of the direct comparison test, previous research (20, 21) and data availability. The coefficient, odds ratio, and p-value for each candidate variable were calculated by univariate analysis of binary logistic regression to explore the influence of each variable on return to driving, which was coded 1 for all analysis. After univariate analysis, significant variables were entered into the multiple regression analysis using 3 models. Two models (Models I and II) were then estimated by enter and forward selection with all significant variables. Another model (Model III) was calculated using only clinical measurement at 7 days after stroke. For the binary variables (coded 0 or 1), we assigned the reference value 0 to female sex, and to no driving education, respectively. After confirming the regression model, the area under the curve (AUC) of the receiver operating characteristic (ROC) curve was measured to compare effectiveness among models. p-values less than 0.05 were considered statistically significant. All analyses were performed using SPSS version 21.0.
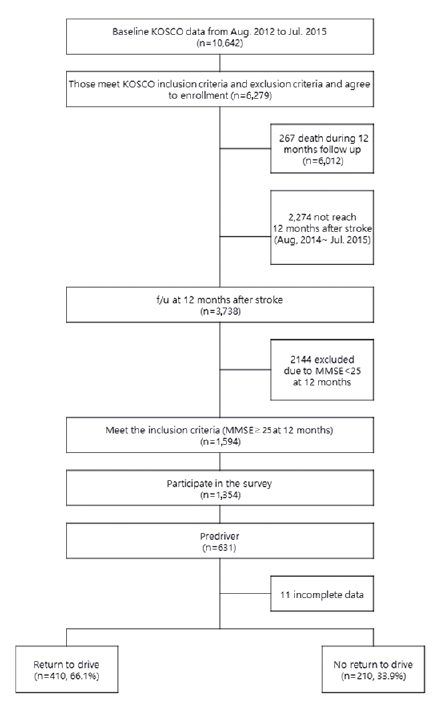
A total of 10,642 patients with a primary diagnosis of ischaemic or haemorrhagic stroke were screened from August 2012 to July 2015. In total, 6,279 stroke patients met KOSCO inclusion and exclusion criteria and agreed to enrollment, a participation rate of 59%. The number of patients with MMSE scores above 24 was 1,594 from among 3,738 patients who were followed up at 12 months. Of the 1,594 patients (MMSE >24) who completed the 12-month follow-up, 1,354 participated in the survey, and 631 were driving at stroke. Of these 631 patients, 11 were excluded because of missing information. Therefore, a total of 620 first-time stroke patients were included in the final analysis (Fig. 1).
Fig. 1. Consort flow diagram for the study.
The mean age (standard deviation; SD) of this subgroup (pre-driver) at time of stroke was 57.35 years (SD 11.67 years), and 85.20% were male. Of the 620 who were drivers, 66.1% (n = 410) had returned to driving at 12 months after stroke. The return to driving occurred 2.15 months (SD 2.32 months) after stroke. Among pre-drivers, 28.5% (n = 177) had received education about return to driving. The demographic and clinical characteristics of each group are shown in Table I.
Table I. General and clinical characteristics of driving returners and non-returners
From univariate logistic regression analysis, age, sex (male/female), stroke type (ischaemic, haemorrhagic), education about return to driving (yes/no), as well as FAC, FMA, K-FAST, K-MMSE, mRS, and NIHSS at 7 days after stroke onset were selected for multivariate regression. Table II shows the odds ratio for each independent variable in each model. All variables show statistical significance except stroke type, NIHSS, FAC, and K-FAST.
Table II. Odds ratios and significance levels for candidate predictors with univariate binary logistic regression analysis, for exploring the influence of each variable on return to driving
Table III shows the odds ratio and its confidence interval (CI) for each logistic model. Sex, driving education, FMA of affected side, age, and mRS showed statistical significance with both model I and model II. The R2 of model I was 0.28 (p < 0.001), and it correctly identified 90.0% (287/319) of returners and 41.6% (67/161) of non-returners. Overall, 73.8% of participants were correctly identified. The area under the ROC curve using this model was 0.74 (Fig. 2).
Table III. Odds ratio of multivariate logistic regression models, proportion of variance in return to driving (R2) associated with predictor variables, accuracy (n of correct assessments/n of all assessments) and AUC of the ROC curve to compare effectiveness among models
Fig. 2. Receiver operating characteristic (ROC) curve of the 3 regression models.
This is the first study to evaluate the current state of return to driving after stroke in the Republic of Korea. It revealed that approximately 64% of first-ever stroke patients returned to driving before 12 months after stroke. This percentage is higher than previous studies on return to driving 1 year after stroke (16, 17, 28), but is consistent with some other studies (21, 29). In these studies, patients who received inpatient rehabilitation services or cross-sectional status will probably have had more severe stroke than those who received acute care only, thus leading to a lower rate of return to driving.
For the general demographic data, male, young and ischaemic stroke patients showed an association with return to driving. After BLR models were made, male sex was maintained with high odds ratio (Model I = 2.98, Model II = 3.03). This association with male sex is not in line with a previous Western study (17). We assume that the discrepancy is due to cultural and societal infrastructural differences between countries. In South Korea, the percentage of women over 60 years of age who drive is lower than that in the USA. Males in our sample were 85.2% of total pre-drivers, a very high percentage compared with a previous USA study (17).
Although not in the final model, higher NIHSS scores (higher impairment) may be associated with a lower probability of return to driving (odds ratio = 0.92, Table II). When looking at the clinical measures performed at 7 days after stroke, our univariate model demonstrates that motor, cognitive, and global functional deficits are predictors of return to driving at 1 year after stroke. Lower mRS (disability) and K-MMSE (cognitive impairment) and higher FMA (better sensorimotor function) of the affected side measured at 7 days after stroke onset indicate a higher likelihood of return to driving.
As the NIHSS is routinely collected at acute stroke care centres around South Korea, and the FMA is a well-known performance-based impairment index for patients with post-stroke hemiplegia, this model could easily be applied to patients with stroke at acute stroke management facilities. This predictive model could assist clinicians in counselling patients about their likelihood of return to driving, and in selecting the type of rehabilitation programme to use. In addition, FMA and NIHSS scores could be measured longitudinally to determine the likelihood of return to driving. The mean time of return was 2.15 months after stroke onset.
Furthermore, provision of education about return to driving is strongly associated with return to driving. In models I and II, the odds ratio (95% CI) of driving education was 2.42 (1.49–3.94) and 2.44 (1.50–3.96), respectively. In this study, there was no specific date when education about driving was administered; how-ever, the mean return time suggests a time frame. In South Korea, there are no regulations about return to driving after a stroke event.
While it is extremely important to know whether the patient is safe to drive, it is also important to be aware of those who are likely to attempt driving. Safe driving is important, given that a large percentage of stroke survivors are not provided with driving evaluations or advice about return to driving (16). This is consistent with our result (25.9%) regarding the relatively low frequency of driving education before return to driving. We assume that the relatively high odds ratio of driving education is associated not only with the clinician’s opinion and judgement about their patient’s driving ability, but also with the patient’s desire to return to driving. There is no validated, widely used evaluation tool for the assessment of driving performance after stroke. Although frequency of education about driving is low, there is good correlation between provision of education about return to driving and actual return to driving. These results suggest that there is a need for a validated evaluation tool and systematic educational programme for return to driving after stroke.
According to Models I, II and III, the general level of disability (as measured using the mRS) was the most powerful predictor of return to driving, not the FMA, a performance-based impairment index. We assumed that these results were based on the complex requirement of return to driving, a function that needs relatively good visual perception, attention, motor strength, cognitive function, and so on. Therefore, FMA, which only measures sensorimotor impairment, cannot be the key measurement to predict return to driving. These results suggest that comprehensive tools for evaluation of return to driving are needed to measure such various functional domains.
This study has several limitations. First, the inclusion criteria were relatively narrow. Because the inclusion criteria included normal cognitive function (K-MMSE > 25) at 12 months after stroke, this study could not demonstrate the status of all stroke patients, because 57.4% of the sample had cognitive impairment at 12 months. Secondly, the study was conducted prospectively with a multicentre design, which may have impacted data reliability. To counteract this problem, the KOSCO committee leads a training course for rehabilitation specialists twice a year. Because the 9 participating centres were located at the main cities of their areas, the cohort, while representative of South Korea, a developing country in East Asia, was relatively smaller and more urban than many stroke cohorts. Thus, there is need for caution in generalizing these findings to other settings, such as Western countries or rural areas. In addition, data were missing on some of the clinical measures. Because the database uses clinical measures collected by rehabilitation specialists during acute and critical periods after stroke, missing data are expected. Although statistical tests were completed to check for randomness of missing data, it cannot be guaranteed that data were missing randomly. Thus, we excluded 11 subjects with incomplete data. This should be taken into account in designing screening tools for use in the clinical setting. Other factors, such as age, driving education, and any other demographic characteristics, need to be considered when counselling patients on return to driving. This study was focused only on whether participants returned to driving; it did not address the issue of safety to return to driving. Predictors of fitness to drive after stroke have been presented in a previous study (30), but actual safety for return to driving has not been addressed.
Conclusion
In South Korea, approximately 60% of patients with first-ever stroke in this study returned to driving. A similar frequency of return to driving was found in previous studies. Motor deficits and general stroke severity at 7 days after stroke were significant predictors of return to driving at 1 year after stroke. Male sex, education about driving, lower mRS, and higher FMA at 7 days after stroke are predictors of return to driving. Using these factors, clinicians may be able to screen for patients who will return to driving at an early period after stroke. This model may enable healthcare professionals to advise persons with stroke and their families.
The authors would like to thank all participants for their commitment to the study.
Funding. This work was supported by the Research Program funded by the Korea Center for Disease Control and Prevention (2016-E33003-02).
The authors have no conflicts of interests to declare.


 Click to show fullsize
Click to show fullsize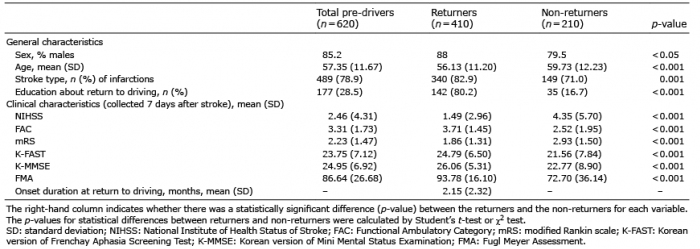 Click to show fullsize
Click to show fullsize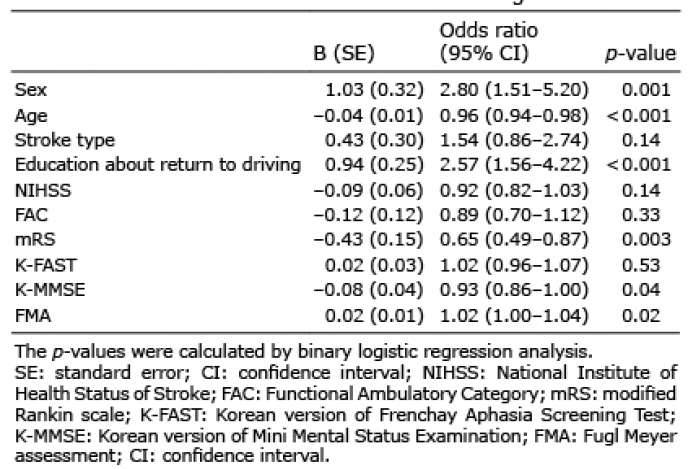 Click to show fullsize
Click to show fullsize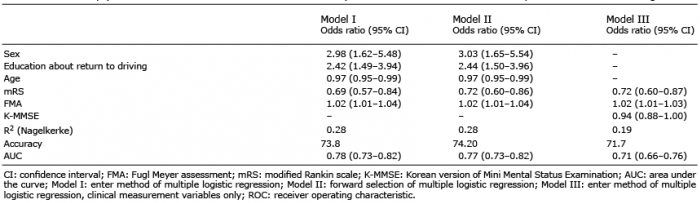 Click to show fullsize
Click to show fullsize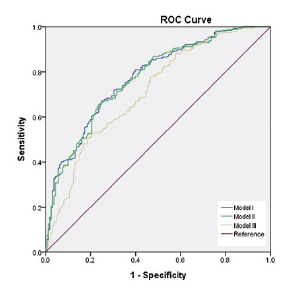 Click to show fullsize
Click to show fullsize