Shengai Li, MS1,2, Argyrios Stampas, MD1,2, Joel Frontera, MD1,2, Matthew Davis, MD1,2 and Sheng Li, MD, PhD1,2

From the 1Department of Physical Medicine and Rehabilitation, McGovern Medical School, University of Texas Health Science Center – Houston, Houston, and 2TIRR Research Center, TIRR Memorial Hermann Hospital, Houston, TX, USA
*An abstract of this paper was presented as a scientific paper at the Association of Academic Physiatrists (AAP) Annual Meeting, Atlanta, GA, USA, during February 14–17, 2018.
Objective: To determine whether transcranial direct current stimulation augments the analgesic effect of breathing-controlled electrical stimulation in patients with spinal cord injury who have chronic neuropathic pain.
Design: Sham-controlled, single-blinded, single-centre, cross-over study of 12 participants with incomplete spinal cord injury. The treatment protocol included a 20-min transcranial direct current stimulation (sham or active), followed by a 20-min breathing-controlled electrical stimulation to the median nerve on the dominant side. The treatment session with sham or control transcranial direct current stimulation was given on different days in a randomized order. Visual analogue scale was used to assess neuropathic pain at baseline, 10 min after transcranial direct current stimulation, and 10 min after breathing-controlled electrical stimulation.
Results: Participants were blinded to the status of transcranial direct current stimulation. Out of the 12 participants, 10 completed sessions of both sham and active transcranial direct current stimulation, while the other 2 completed only active transcranial direct current stimulation and breathing-controlled electrical stimulation treatment. Out of the 12 participants, 7 showed analgesic effects after active transcranial direct current stimulation, while sham transcranial direct current stimulation produced some analgesic effects in 4 out of 10 participants. At the group level, there was no difference between active and sham transcranial direct current stimulation treatment. All except one participant responded positively to breathing-controlled electrical stimulation in all sessions. Visual analogue scale score for pain decreased significantly after breathing-controlled electrical stimulation combined with either active transcranial direct current stimulation or sham transcranial direct current stimulation treatment.
Conclusion: The immediate analgesic effect of breathing-controlled electrical stimulation was confirmed. However, this effect was not augmented after one session of transcranial direct current stimulation treatment.
Key words: electrical stimulation; neuropathic pain; spinal cord injury; transcranial direct current stimulation; breathing-controlled electrical stimulation.
Accepted Jun 12, 2018; Epub ahead of print xx, 2018
J Rehabil Med 2018; 50: 00–00
Correspondence address: Sheng Li, Department of Physical Medicine and Rehabilitation, McGovern Medical School, University of Texas Health Science Center – Houston, 1333 Moursund, Houston, TX 77030, USA. E-mail: sheng.li@uth.tmc.edu
This study examined whether transcranial direct current stimulation (tDCS) augments the analgesic effect of breathing-controlled electrical stimulation (BreEStim) in patients with spinal cord injury who have chronic neuropathic pain. The same cohort of 12 subjects with spinal cord injury received active or sham tDCS prior to a single session of BreEStim treatment on a different day. Both active and sham tDCS were found to have some analgesic effects in some patients, but there was no difference at the group level. BreEStim had an immediate analgesic effect; however, this effect was not augmented by the priming tDCS treatment. In summary, the immediate analgesic effect of BreEStim was not augmented by one session of tDCS treatment.
Neuropathic pain is an important contributor to suffering, poor rehabilitation outcomes and reduced quality of life in persons with spinal cord injury (SCI). Several factors affect this situation. Neuropathic pain is common (1–3). According to the US National Spinal Cord Injury Statistical Center (https://www.nscisc.uab.edu/), there are approximately 17,000 new cases of SCI per year, resulting in an estimated total of 282,000 patients with SCI in the USA. Approximately 65–85% of people with SCI experience neuropathic pain and, of these, approximately 33% have severe neuropathic pain (4). Neuropathic pain is difficult to manage (5). Pharmacological interventions are the first line of treatment (6), but are often associated with side-effects, such as addiction, withdrawal, constipation, and sedation; all of which may affect participation in activities of daily living. Neuropathic pain does not resolve over time. In contrast, many people with SCI report that the pain continues, and even worsens, over time (7). There are currently no effective pharmacological treatments for neuropathic pain. A number of pharmacological agents have been recommended by the Neuropathic Pain Special Interest Group (NeuPSIG) of the International Association for the Study of Pain (8). Unfortunately, opioids are currently the primary therapeutic options for neuropathic pain after SCI (9). Surprisingly, only 7% of responders in a postal survey reported that pharmacological treatment is effective (10). These challenges in treating neuropathic pain after SCI probably contribute to opioid overuse and the current epidemic of opioid use (11). The US Senate recently passed the Comprehensive Addiction and Recovery Act (CARA), which takes incremental steps to combat the epidemic, signing it into law in July 2016 (12). To combat this epidemic and to help manage neuropathic pain after SCI, in particular, further investigation of non-pharmacological modalities is needed.
Different neuromodulation interventions have been developed for pain management, such as transcutaneous electrical nerve stimulation (TENS) (13), electroacupuncture (14), spinal cord stimulation (15), deep brain stimulation (16), and transcranial direct current stimulation (tDCS) (17–19). tDCS is a promising non-invasive brain stimulation technique for pain management, which uses weak electrical currents applied through 2 oppositely-charged electrodes on the scalp to induce neuroplastic changes. These changes can alter pain perception in people with chronic pain, such as those with SCI. A meta-analysis of different neuromodulation techniques for pain management after SCI identified 8 clinical trials that have used various neuromodulation techniques in the last 15 years (20). Specifically, there were 3 tDCS, 2 transcranial electrical stimulation (TES), 2 repetitive transcranial magnetic stimulation (rTMS) and 1 TENS study. Overall, the effect was heterogeneous. However, patients with SCI were most responsive to tDCS compared with other interventions. Anodal tDCS targeting the primary motor cortex (M1) is thought to specifically modulate the excitability of cortico-thalamic pathways, thus altering the sensory component of pain (21). This hypothesis is supported by the findings of increased sensory perception and pain threshold after anodal tDCS targeting M1 (19). Furthermore, the analgesic effect was better and longer-lasting when tDCS was combined with visual illusion in patients with SCI (22).
Previously, we developed an innovative treatment for the management of neuropathic pain, termed breathing-controlled electrical stimulation (BreEStim) (23, 24). This technique is based on research into the systemic effects of human voluntary breathing on motor function and pain perception (23–29). In the BreEStim treatment (see details in (23)), human voluntary breathing triggers an external electrical stimulator that delivers a single pulse of electrical stimulation to a peripheral nerve, such as the median, ulnar, or radial nerve. Following BreEStim treatment on one side, pain thresholds increased without change in sensation thresholds in both the treatment and contralateral sides in pain-free healthy participants (30–32). Therefore, the BreEStim mechanism is postulated to occur at the central level, modifying how participants react to the noxious stimuli, i.e. the affective response to the same stimuli, or de-sensitization. In a previous study we found that patients with SCI who have chronic neuropathic pain demonstrate significant analgesic effects after receiving BreEStim treatment (33).
Both tDCS and BreEStim interventions have been shown to have analgesic effects in patients with SCI. The current study investigated whether neuromodulatory effects of tDCS could further augment the immediate analgesic effects of BreEStim in patients with SCI who have chronic neuropathic pain. It was hypothesized that tDCS could augment the analgesic effects of BreEStim treatment. Specifically, it was expected that BreEStim combined with active tDCS targeting M1 would result in a greater reduction in pain than BreEStim alone in patients with SCI who have chronic neuropathic pain.
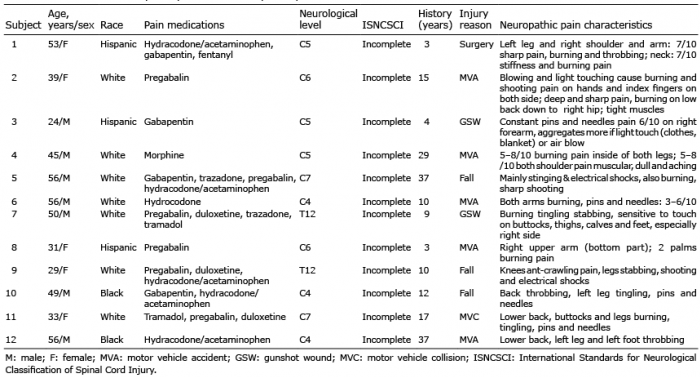
Twelve subjects with SCI (see Table I) from TIRR Memorial Hermann Outpatient SCI Clinic were enrolled in the study. All participants were assessed neurologically and referred by SCI board-certified physicians according to the International Standards for Neurological Classification of Spinal Cord Injury (ISNCSCI) (34).
Table I. Characteristics of participants and neuropathic pain
The inclusion criteria were: SCI participants who: (i) had neuropathic pain after SCI with a score of 12 or above on the LANSS scale Leeds Assessment of Neuropatic Symptoms and Signs as in our previous study (33); (ii) were aged 18–75 years; (iii) had chronic pain for >3 months, and; (iv) had been stable on oral pain medications for the preceding 2 weeks. Participants were allowed to continue their pain medication at the prescribed dose and frequency. Patients were excluded if they: (i) were currently adjusting oral pain medication for neuropathic pain; (ii) had non-neuropathic pain, e.g. shoulder pain due to wheelchair use; (iii) had a pacemaker (to avoid possible side-effects of electrical stimulation); (iv) were not able to follow commands or to provide consent; (v) had asthma or other pulmonary diseases; or (vi) were not medically stable. Detailed information for the participants is listed in Table I. The study was approved by the Committee for the Protection of Human Subjects at the University of Texas Health Science Center at Houston. All participants provided written informed consent. The study is registered at https://clinicaltrials.gov (NCT03302793).
This study has a single-blinded, single-centre, sham-controlled, crossover design (Fig. 1). The protocol included a 20-min tDCS (sham or active) to the current dominant primary motor cortex (M1), followed by a 20-min BreEStim to the median nerve (160 times) transcutaneously on the current dominant side. Each combined intervention was given at least 3 days apart in a randomized order (33). Ten participants completed both active and sham tDCS sessions, while, due to scheduling issues, the remaining 2 participants only completed active tDCS sessions.
Fig. 1. The experimental design and settings. Neuropathic pain was assessed by visual analogue scale (VAS) at baseline (VASBaseline), 10 min after sham/active transcranial direct current stimulation (tDCS) (VAStDCS) and 10 min after breathing-controlled electrical stimulation (BreEStim) (VASBreEStim).
Participants were blinded to the status of tDCS (sham or active). Anodal tDCS targeting M1 (19) was used. During each session, participants received either active or sham stimulation to M1. A pair of surface sponge electrodes (35 cm2) were soaked in saline water and then applied to the scalp. The anode electrode was placed over C3 according to the 10–20 system for EEG electrode placement. The reference cathode electrode was placed over the supraorbital area on the opposite side. For all active tDCS conditions, direct current was delivered by a specially developed, battery-driven, constant current stimulator (Soterix Medical, NY, USA) with a maximum output of 10 mA. A constant current of 2 mA was applied for 20 min (the effect is usually expected to last 1–2 h after tDCS) (19). BreEStim was then delivered after the 20-min tDCS (active or sham).
The previous BreEStim protocol (30, 33) was used in this study. Briefly, participants wore a facemask connected to a Pneumotach system to record breathing signals. Surface electrodes were trimmed and placed transcutaneously over the median nerve 3 cm above the wrist (for experimental set-up, see Fig. 1). In the BreEStim treatment, a single-pulse (pulse width of 0.1 ms square wave) electrical stimulus was triggered and delivered transcutaneously to the median nerve, while participants were taking a fast, strong, deep inhalation, similar to a deep breath, but faster and stronger. The trigger threshold was set at 40% of peak airflow rate, i.e. the electrical stimulator was triggered to deliver an electrical pulse when the airflow reached its threshold. The airflow rate was measured with the Pneuotach system real-time. It is important to note that the participants controlled the intensity of electrical stimulation, increasing the intensity gradually if tolerated. Participants were explicitly instructed that awareness of painful stimulation was part of treatment protocol. The detailed protocol for BreEStim is available at https://www.jove.com/video/50077/. To standardize, the total number of electrical stimuli was 160, with sufficient rest allowed during the treatment as needed. The BreEStim treatment took approximately 20 min. As in previous studies, participants tolerated the procedure well.
The outcome measurement was a visual analogue scale (VAS) for pain assessment. VAS has been extensively used and validated (35). Each subject with SCI was given a standard and detailed explanation of the VAS scoring system prior to any intervention, and a card showing the scale and facial expressions. In a previous study (33), we applied the VAS 10 min after BreEStim. Similarly, in this study, VAS was applied at baseline (VASBaseline), 10 min after tDCS (VAStDCS) and 10 min after BreEStim (VASBreEstim) (Fig. 1). Participants were instructed to self-assess and report the level of pain at the time of evaluation. Therefore, VAS scores were reflective of immediate effects of interventions (sham/active tDCS or BreEStim). It was reported that the levels of pain were different in the different locations of the body across patients with SCI (36). To assess the overall analgesic effects of tDCS and BreEStim, VAS scores averaged across different body locations were used as an index of the global pain intensity in this study (33, 37). Participants were instructed to maintain the same schedule for pain medications. To minimize possible confounding effects of medications on the interventions, both sessions (sham/active tDCS) were performed at similar times of day in individual participants.
Statistical analysis of VAS is controversial (38). Both parametric and non-parametric tests have been used for VAS scores and both performed similarly (39). Although VAS is an ordinal scale, it is considered to possess properties of interval and ratio data, and can be analysed using parametric methods (40). The current study used parametric tests for power calculation and statistical analysis.
Power calculations were performed based on published data on tDCS (20) and BreEStim (33). A meta-analysis comparing the effects of tDCS treatment for neuropathic pain after SCI showed a standardized effect size of 0.52 (20). Using a paired Student’s t-test, and assuming the within-subject correlation to be 0.5, to achieve a power of 0.8 with an alpha level of 0.05, we needed to recruit 4 patients to be tested under both sham and active tDCS conditions. To study the interactions between BreEStim and tDCS, i.e. to compare the changes from post-tDCS to post-BreEStim in groups of BreEStim + active tDCS and BreEStim + sham tDCS, we found that in BreEStim+sham tDCS group (i.e. BreEStim alone in our previous study (33)), the VAS score reduced by 2.6 (from 6.3 to 3.7, with an approximate standard deviation (SD) of 1.5) (33). We hypothesized that active tDCS would augment the BreEStim-induced analgesia. Therefore, we assumed that in BreEStim + active tDCS group, the VAS score would be reduced by approximately 4, with a similar SD of 1.5. Using the paired t-test with the same correlation, to achieve a power of 0.8 with an alpha level of 0.05, we needed to recruit 10 patients to be tested under both sham and active tDCS.
Descriptive statistics were used for the characteristics of participants with SCI. Within-subject repeated measures 2-way analysis of variance (ANOVAs) were performed on the VAS scores by interventions in the 10 participants who completed both active and sham treatments. The factors were “Intervention” (2 levels, sham tDCS+BreEStim vs. active tDCS+BreEStim) and “Time” (3 levels, baseline, post-tDCS, and post-BreEStim). In all 12 participants who completed the active tDCS treatment, a within-subject 1-way ANOVA was performed to assess whether active tDCS and BreEStim had additive analgesic effects. Post-hoc analyses were further performed to compare the individual and combined analgesic effects. p < 0.05 was chosen to indicate statistically significant differences.
All participants tolerated the protocol well. Ten of the 12 participants completed both sham and active tDCS sessions, while the remaining 2 only completed active tDCS and BreEStim treatment. As shown in Fig. 2, 7 out of 12 participants had positive analgesic responses to active tDCS, while sham tDCS produced analgesic effects in only 4 out of 10 participants. However, BreEStim had immediate analgesic effects in all except one subject. At the group level (Fig. 3), there was no difference between active and sham tDCS treatment. VAS decreased from 5.7 (VASBaseline) to 5.1(VAStDCS) after active tDCS, and from 6.0 (VASBaseline) to 5.4 (VAStDCS) after sham tDCS. VAS score decreased significantly after BreEStim in the active tDCS group (VASBreEStim, 3.2) and in the sham tDCS group (VASBreEStim, 3.5) (F2,18= 45.96, p<0.00001) (Fig. 3). For all 12 participants who completed active tDCS and BreEStim, a main effect of Time was found (F2,22= 44.07, p < 0.00001). Post-hoc tests showed no significant change in VAS after active tDCS (VASBaseline 5.9 vs. VAStDCS 5.3), but VAS decreased significantly after BreEStim (VASBreESti 3.1).
Fig. 2. Individual analgesic responses to combined sham (left) or active (right) transcranial direct current stimulation (tDCS) and breathing-controlled electrical stimulation (BreEStim) therapy. VAS: visual analogue scale.
Fig. 3. Mean analgesic responses to combined sham (black) or active (grey) transcranial direct current stimulation (tDCS) and breathing-controlled electrical stimulation (BreEStim) therapy. Visual analogue scale (VAS) was assessed at baseline (VASBaseline), 10 min after sham/active tDCS (VAStDCS) and 10 min after BreEStim (VASBreEStim). *Statistical significance.
In this study, a cohort of 12 participants with SCI who had chronic neuropathic pain received active or sham tDCS on different days prior to receiving BreEStim treatment. Both active and sham tDCS produced some analgesic effects in a subgroup of participants, but at the group level, neither tDCS interventions produced a significant analgesic effect. As seen in the previous study (33), the current results confirm that BreEStim produced immediate analgesic effects. No augmented analgesic effects were observed in the combined tDCS and BreEStim treatment.
In this study, participants with SCI responded more frequently after active tDCS than after sham tDCS for neuropathic pain. However, no significant differences were observed in analgesic effects between sham and active tDCS interventions at the group level. This result was inconsistent with previous studies. In general, tDCS has moderate analgesic effects for neuropathic pain after SCI, according to a meta-analysis (20). Pain reduction of 1.33 units on a 10-item scale was found post-tDCS treatment from pooled data in an SCI population. However, results from the included studies were heterogeneous. Many factors, such as history of depression, duration of chronic pain after SCI, and duration of treatment can influence the effectiveness of tDCS treatment. Patients with SCI with a mean pain duration <5 years had significant pain reduction after tDCS treatment (17, 41, 42). In contrast, patients with SCI with a pain duration > 5 years did not benefit from tDCS treatment (22, 43). These findings demonstrate that patients with SCI with longstanding neuropathic pain are refractory to tDCS treatment. In our cohort of participants with SCI, 9 out of 12 participants had a pain duration >5 years. This could explain why we did not observe significant improvements at the group level after active tDCS treatment.
It has been shown that, when combined with visual illusion, tDCS treatment leads to augmented analgesic effects in patients with SCI, compared with tDCS alone or visual illusion (VI) alone (22). In contrast, in the current study, there was no difference in analgesic effects between BreEStim with active tDCS or with sham tDCS. The contrasting findings were probably attributable to subject enrolment, rather than the modality difference between illusion and BreEStim. In Soler et al.’s study, 9 of 10 participants had a pain duration of 5 years or less in the tDCS + VI group, while the pain duration was longer than 5 years for the majority of participants in the other 3 groups (tDCS, VI, or placebo). This difference in pain duration among experimental groups may explain the different outcomes, at least for tDCS vs tDCS+VI groups, as shown by a meta-analysis highlighting the important role of pain duration (20).
In contrast to the observation that there was no difference in analgesic effects between active and sham tDCS in patients with SCI who had chronic neuropathic pain, BreEStim treatment had significant analgesic effects post-treatment. The contrasting results suggested different underlying mechanisms between 2 interventions for neuropathic pain after SCI. In this study, a commonly used tDCS was adopted, including 2 mA anodal tDCS targeting M1 for 20 min (44). It is known that anodal tDCS targeting M1 increases both pain and sensory perception thresholds (19). A study on positron emission tomography findings after anodal tDCS to M1 reported decreased metabolism in dorsolateral prefrontal cortex and increased metabolism in medulla and anterior cingulate cortex and insula in patients with SCI who had neuropathic pain (41). These findings suggest that tDCS can modulate emotional and cognitive components of pain.
BreEStim has been shown to increase the pain threshold, without affecting the sensory perception threshold, in a number of studies (30–32). As such, BreEStim provides central de-sensitization effects and thus analgesic effects for chronic neuropathic pain after SCI (33, 45) and amputation (45). BreEStim-induced analgesia and de-sensitization is probably related to impaired memory consolidation of peripheral electrical stimulation. Voluntary breathing activates cortical and subcortical areas extensively, including the insula. If peripheral aversive stimulation, such as electrical stimulation, is given during activation of the insular cortex, painful electrical stimulation is not remembered, or is remembered to a lesser degree. In other words, there is item-specific impairment of aversive memory reconsolidation, i.e. anterograde amnesia (46). In agreement with these findings, in the current study participants with SCI reported electrical stimulation during BreEStim was not sharp or aversive. This is possibly related to de-sensitization of painful stimulation.
Neuropathic pain after SCI is probably due to maladaptive plastic cortical reorganization and sensitization of the central nervous system (CNS), although this is poorly understood (3, 47–50). As a result of SCI and partial/complete denervation of spinal neurones, communication between the brain and the periphery is partially or completely interrupted. Neuroplasticity at the injury level can lead to recovery, but maladaptive neuroplasticity, such as collateral sprouting, astrocytic/microglia activation, and loss of descending inhibition, also occurs at the spinal and supraspinal levels, leading to CNS sensitization and subsequent central pain. Because of its de-sensitization effects, BreEStim was able to provide immediate analgesic effects for patients with SCI who had longstanding chronic neuropathic pain, while such relief was not always seen after tDCS.
The “negative” effect of tDCS in this study should not be interpreted as “negative analgesic effects” of tDCS treatment. It is more appropriate to interpret it as a lack of immediate analgesic effect after 1 session of tDCS treatment (51). This finding is probably attributable to study design limitations. In contrast to previous studies of the long-term use of tDCS (1~2 weeks), only one session of active or sham tDCS was given in the current study. Some cumulative effects may occur after a delay. In a more recent study, Thibaut et al. (51) reported analgesic benefits of a 5-day treatment with tDCS compared with sham tDCS, measured at 4-week follow-up. A long-term combined tDCS and BreEStim therapy in the future will be able to better examine whether there is a synergistic effect. Such study is better performed in SCI participants with a shorter pain duration (< 5 years), that tDCS-induced analgesia is evident (17, 41, 42). Further research is needed into whether there is a synergistic effect in long-term combined tDCS and BreEStim therapy. Such a study should be performed in subjects with SCI with a shorter pain duration (<5 years), so that tDCS-induced analgesia is evident (17, 41, 42). Similarly, research into long-term BreEStim treatment (5 days or more) is needed to elucidate possible cumulative analgesic effects.
An immediate analgesic effect occurs after BreEStim, but not after active tDCS. No additive analgesic effect was observed in a combined tDCS and BreEStim intervention for neuropathic pain after SCI.
This study was supported in part by NIH NICHD/NCMRR R21HD087128, R21HD090453, Mission Connect, a programme of the TIRR Foundation (015-116). The authors thank Liang Zhou, PhD, statistician and Associate Professor at the Center for Clinical and Translational Sciences at McGovern Medical School, University of Texas Health Science Center – Houston, who performed power calculations.
Competing interests: Sheng Li holds US Patent No. 8,229,566 ‘’Method and Apparatus of Breathing-Controlled Electrical Stimulation for Skeletal Muscles’’, issued on 7/24/2012 and U.S. Patent No. 8,588,919 ‘’Method and Apparatus of Breathing-Controlled Electrical Stimulation for Skeletal Muscles’’ Divisional of Application No. 12/146,176 (issued as U.S. Patent 8,229,566). Sheng Li was blinded to all experiments and had no direct patient contact in this study.


 Click to show fullsize
Click to show fullsize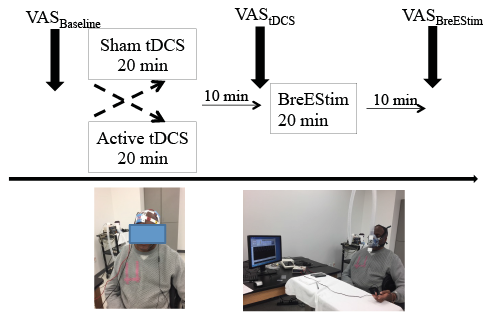 Click to show fullsize
Click to show fullsize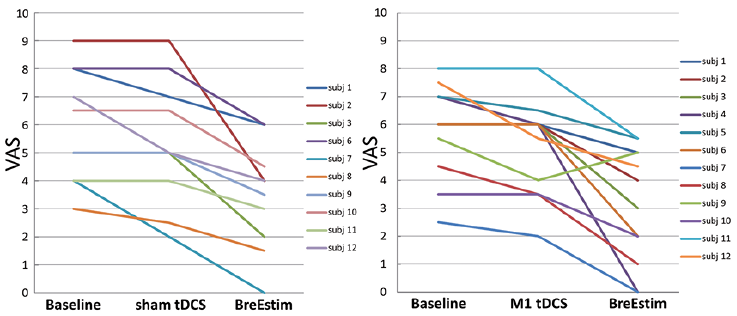 Click to show fullsize
Click to show fullsize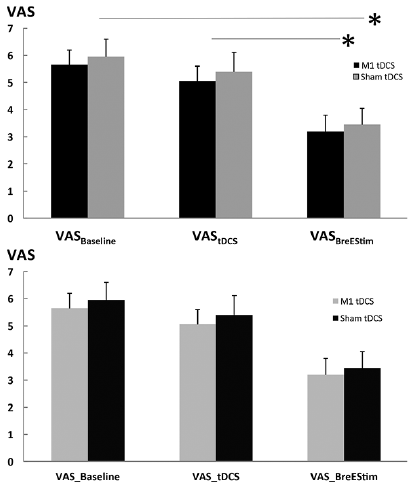 Click to show fullsize
Click to show fullsize