
From the 1Department of Rehabilitation Medicine, The First Affiliated Hospital of Nanjing Medical University, and 2Department of Pathogen Biology and Immunology, Jiangsu Province Key Laboratory of Pathogen Biology, Nanjing Medical University, Nanjing, Jiangsu, China
#These authors contributed equally to this work.
Objective: To explore the relationship between electrical current and nerve–needle distance for localization of target nerves in peripheral nerve block, and the effects of injection speed, concentration, and injectate volume on alcohol dispersion using an animal model.
Methods: Rabbit tibial nerves were selected for localization. Nerve–needle distance was ascertained using a manipulator. The minimum current eliciting motor responses was recorded at nerve–needle distances of 0, 1, 2, 3, 4 and 5 mm. Rabbit tibial nerves were assigned into 3 groups: speed group, concentration group, and volume group. Nerves were localized by a stimulator and neurolysed with alcohol/contrast medium. Helical computed tomography (CT) was performed to measure volume/dispersion patterns of injectate.
Results: A linear relationship was observed between nerve–needle distance (X) and minimal current (Y) (Y = 0.13X + 0.22; r2 = 0.974; p<0.05) for the localization of the target nerve. CT scan revealed that the injection speed and volume significantly influenced the dispersion of alcohol (p<0.01), but concentration had no effect (p<0.05).
Conclusion: This study found a positive linear relationship between nerve–needle distance and minimum electrical stimulation in tibial nerve blockade. In addition, the results suggest that a low volume of alcohol with a low injection speed can help to improve nerve block in clinical practice.
Key words: muscle spasticity; rehabilitation; alcohol; tibial nerve.
Accepted Jun 15, 2018; Epub ahead of print Aug 8, 2018
J Rehabil Med 2018; 50: 00–00
Correspondence address: Jianan Li, and Hongxing Wang, Department of Rehabilitation Medicine, The First Affiliated Hospital of Nanjing Medical University, 300 Guangzhou Road, Nanjing, 210029, China. E-mail: lijianan@carm.org.cn; wang_hongxing@163.com
Spasticity can negatively influence rehabilitation training and activities of daily living. Nerve blockade with alcohol is a widely accepted method for reducing spasticity. Successful treatment requires accurate localization of the needle tip and understanding of the factors that influence alcohol dispersion. This study investigated the relationship between electrical stimulation and nerve–needle distance, as well as how injection speed, concentration and volume affect alcohol dispersion along the nerve trunk using an animal model. We conclude that there is linear relationship between nerve–needle distance and stimulation current for localization of the target nerve, and that the injection speed and volume influence the dispersion of alcohol, but that concentration has no effect.
Management of spasticity in rehabilitation medicine is a major challenge. Spasticity can negatively influence rehabilitation training and activities of daily living (1, 2), and can lead to secondary complications (e.g. pain, contractures, skin breakdown) (3–5). Chemical neurolysis is one of the most widely accepted and frequently used methods for reducing spasticity (6–9).
Neuromuscular blockade via injection of alcohol is frequently used to reduce the tone of overactive muscles in clinical practice (10–12). The effect of a nerve block using alcohol can be influenced by the: volume and concentration of injectate; selection of block site; localization of the target nerve; and dispersion of the injectate (13).
The injected fluids used in a peripheral nerve block spread along the route of least resistance (14). The spread of injectate to adjacent areas may lead to blocking of, and damage to, non-target nerves and muscles, resulting in unintentional loss of function (15). Theoretically, the closer the needle tip is to the target nerve, the less injectate will be needed for an identical blocking effect, and less undesired neurolysis of non-target nerves will result. Therefore, good understanding of the characteristics of localization and dispersion of alcohol injections along the target nerve is critical for the success or failure of peripheral nerve blocks.
Various methods are used for localization of target nerves: ultrasound, computed tomography (CT) and radiography (16, 17). Electrical stimulation is also used widely for localization of the target nerve (18, 19). The smaller the stimulation current that is required to elicit a response from a nerve, the closer the needle tip is to the target nerve. However, the exact relationship between the stimulation current and nerve–needle distance has not been evaluated systematically.
In order to minimize the negative side-effects of peripheral neurolysis, so that the potential impairment of non-target nerves and muscles is reduced, one must identify how different injection factors (speed, volume, concentration) influence alcohol dispersion. Studies have shown that injection speed, as well as the concentration and volume of injectate, can affect dispersion (20), but these influences have not been determined clearly in peripheral nerve blocks using alcohol (20).
The aim of this study was to determine the characteristics of the localization and dispersion of alcohol injections for peripheral nerve blocks by investigating: (i) the relationship between electrical stimulation current and nerve–needle distance; (ii) the effects of different injection speeds, concentrations and volumes on alcohol spread into surrounding tissues.
All animal experimental protocols were in accordance with the Guide for the Care and Use of Laboratory Animals (US National Institutes of Health, Bethesda, MD, USA) and were approved by the ethics committee of Nanjing Medical University and Jiangsu Province Hospital, Nanjing, China.
The present study was in 2 parts: a nerve localization study and an alcohol dispersion study. Seven New Zealand white rabbits were used for the nerve localization study, and 27 rabbits for the alcohol dispersion study. All of the rabbits were provided by the Laboratory Animal Center of the Agricultural Science Institute of Jiangsu Province, Jiangsu, China.
A Nerve Stimulator (SY-708A; Jiangsu Skyray Instrument Company, Jiangsu, China) was used in all experiments. The pulse width of the stimulus was 0.2 ms, and the pulse frequency 2 Hz. A Teflon-coated needle (Jiangsu Skyray Instrument Company, Jiangsu, China) was used to locate the nerve. All of the needle body was insulated, only the bevel surface of the needle tip was uninsulated.
To investigate the relationship between stimulation current and nerve–needle distance, a total of 7 New Zealand white rabbits (14 tibial nerves) were acclimatized for 1 week in rooms with controlled conditions (temperature: 20~25°C; humidity: 40~60%) before the study. On the day of the experiment, the trunk and extremities of the rabbit were held on a table in a prone position without movement. Phenobarbital (30 mg/kg body weight) was delivered through the auricular vein for general anaesthesia. The skin area over the buttocks, posterior thigh, and calf was shaved. A longitudinal incision was made on the lateral side of the posterior thigh. With careful separation along the fascial septum between the hamstring muscles, the tibial nerve was exposed with little or no bleeding. Great care was taken to avoid injury to blood vessels and nerves. Rectal temperature was maintained at 38°C with an infrared lamp throughout the experiment.
To investigate the relationship between the nerve–needle distance and the required current, the nerve–needle distance was determined by measuring the needle movement. To achieve this aim, the needle and a 1-ml syringe were placed on a 3-dimensional manipulator. The extent of advance and retraction of the needle could be measured on the scale of the manipulator axis. The needle was connected to the cathode of the stimulator. The anode of the nerve stimulator was attached to the heel of the hind limb. The needle was inserted at the popliteal fossa and adjusted by the manipulator in a mediolateral direction or up and down until the centre of the needle tip was in contact with the nerve trunk. The nerve–needle distance at this point was defined as 0 mm. The nerve stimulator was turned on and the stimulation current adjusted. The minimum current required to elicit a motor response (movement in the ankle joint or toe) was recorded. The needle tip could be lifted up vertically using a 3-dimensional manipulator by screwing the micrometre nut, which raised the needle 1 mm when turned 360°. Then, the needle was withdrawn by 1-mm increments until the nerve–needle distance was 5 mm. The minimum current to elicit a motor response at each nerve–needle distance (1, 2, 3, 4 and 5 mm) was recorded, which allowed determination of the relationship between the nerve–needle distance and the required current.
To investigate the influence of injection speed, injectate concentration and volume on dispersion, nerve block was performed with different alcohol injection speeds, concentrations or volumes, and then CT scan was used to observe and evaluate the dispersion. The nerve block using alcohol was carried out at the tibial nerve of anaesthetized rabbits with the help of a nerve stimulator. A 5:1 mixture of alcohol and contrast medium (iopromide; Ziqi Biotechnology Company, Shanghai, China) was injected. This mixture could be imaged by CT to evaluate the extent of injectate dispersion. This process was repeated with different concentrations and volumes of alcohol, as well as different injection speeds, to evaluate how each influenced the alcohol dispersion.
A 16-detector row spiral CT system (Somatom Emotion 16; Siemens, Munich, Germany) was used for imaging injectate diffusion after blockade of the tibial nerve. Scanning parameters were: 130 kV; 60 mA; 500 Hounsfield units (HU) for window width; 40 HU for window level; 1.5 mm for slice thickness and pitch. CT images were used to calculate the volume of the diffusion. The images were reconstructed into 3 dimensions by volume-rendering to evaluate the pattern and extent of the dispersion. CT scan was carried out 10 min after nerve blockade (the preliminary experiment showed that alcohol stopped spreading 10 min after injection).
To investigate the influence of injection speed, injectate concentration and volume on dispersion, 27 New Zealand White rabbits of either sex (2.0~2.5 kg) were selected for this experiment. A total of 54 tibial nerves were studied. Three groups were created based on different influencing factors (injection speed, concentration and volume of alcohol) of injectate spread. The groups included a speed group (n = 9, 3 subgroups), concentration group (n = 6, 2 subgroups) and volume group (n = 12, 4 subgroups). For each subgroup (n = 3) of all groups, 6 tibial nerves were studied.
The speed group (group I) was divided into 3 subgroups (Ia, Ib, Ic). Each tibial nerve in subgroup received 0.3 ml 100% dehydrated alcohol at different injection speeds (in ml/s: Ia, 0.004; Ib, 0.01; Ic, 0.1). Injection speed was controlled by single-channel injection pump (WZ-50C6; Jiangsu Suyun Medical Material Company, Jiangsu, China).
The concentration group (group II) was divided into 2 subgroups (IIa, IIb). Each tibial nerve in subgroup received a 0.3-ml injection of alcohol at different concentrations (IIa, 50% alcohol; IIb, 100% dehydrated alcohol). All subgroups received injections at a speed of 0.01 ml/s.
The volume group (group III) was subdivided into 4 subgroups (IIIa, IIIb, IIIc, IIId). Each tibial nerve in subgroup received different injection volumes (in ml; IIIa, 0.1; IIIb, 0.3; IIIc, 0.5; IIId, 1.0) at identical speed (0.01 ml/s) and identical concentration (100% dehydrated alcohol).
After nerve blockade, helical CT was performed for all rabbits to measure the volume of injectate and its dispersion pattern using 3-dimensional reconstruction.
For the nerve localization study, the relationship between electrical current and nerve–needle distance was evaluated using linear regression analysis. For the alcohol dispersion study, 3 separate analysis of variance (ANOVA) analyses with Bonferroni correction were made to compare the volumes of alcohol dispersion between subgroups of each group (I, II and III). Statistical analyses were carried out with STATA v9.0 (Stata Corp., TX, USA). p < 0.05 was considered significant.
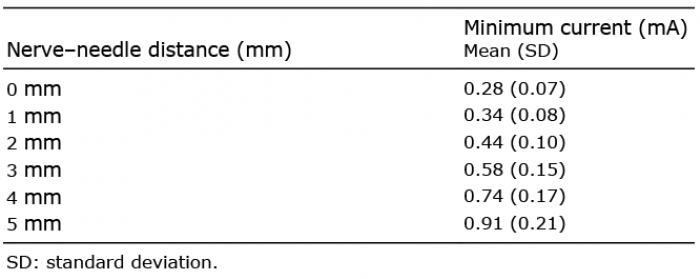
The minimum currents required to elicit a motor response from the tibial nerve at each nerve–needle distance measured are shown in Table I. A scatter plot was created, and linear regression analysis showed a linear trend between the minimum current required and nerve–needle distance. Taking the nerve–needle distance as an independent variable X, and minimum intensity of electrical current as Y, a linear relationship between X and Y was noted (Y = 0.13X + 0.22; r2 = 0.974; p < 0.05) (Fig. 1).
Table I. Minimum current required to elicit a motor response of the target nerve at different nerve–needle distance
Fig. 1. Relationship between nerve–needle distance and required current. Linear regression analysis shows a linear relationship between nerve–needle distance (X) and minimum current (Y). The linear equation is Y = 0.13X + 0.22 (r2 = 0.974, p < 0.05).
To investigate the influence of the injection speed of the injectate on dispersion, alcohol was injected with different speed and then dispersion was observed. The volume of alcohol dispersion of group Ic (0.1 ml/s) was significantly different from that of Ia (0.004 ml/s) and Ib (0.01 ml/s) (p < 0.01). The difference between Ia and Ib was not significant (p > 0.05) (Fig. 2).
Fig. 2. Influence of injection speed on alcohol dispersion. The volume of alcohol dispersion of different speed groups Ia (0.004 ml/s), Ib (0.01 ml/s) and Ic (0.1 ml/s).
To investigate the effect of the concentration of the injectate on dispersion, alcohol with different concentration were injected and then dispersion was observed. However, there was no significant difference between the volume of dispersion of group IIa (50% alcohol) and IIb (dehydrated alcohol) (p > 0.05) (Fig. 3).
Fig. 3. Influence of concentration on alcohol dispersion. The volume of dispersion of different concentration groups IIa (50% alcohol) and IIb (dehydrated alcohol).
To investigate the effect of the volume of the injectate on dispersion, alcohol with different volumes was injected and then spread was observed. The volume of spread of any 2 groups was significantly different from each other (p < 0.01). The volume of dispersion of group IIId was significantly greater than that of the other subgroups (p < 0.01) (Fig. 4).
Fig. 4. Influence of injection volume on injectate dispersion. The dispersion of different volume groups IIIa (0.1 ml), IIIb (0.3 ml), IIIc (0.5 ml), and IIId (1 ml).
Alcohol neurolysis is widely acknowledged as an effective treatment for spasticity (12, 21–23). The “ideal” treatment strategy would be to achieve long-lasting relief of disabling hypertonia without causing impairment of motor function, impairment of sensation, or other non-therapeutic side-effects in the surrounding areas (24). This strategy requires accurate localization of the needle tip and understanding of the factors that influence injectate dispersion. The present study focused on investigating the relationship between electrical stimulation and nerve–needle distance, as well as how injection speed, concentration and volume independently affect injectate dispersion along the nerve trunk. The results indicate that there was linear relationship between nerve–needle distance and minimal current for the localization of the target nerve, and CT construction found that the injection speed and volume significantly influenced alcohol dispersion, but concentration had no effect.
Various methods have been used to guide needle placement. Generation of a motor response by peripheral nerve stimulation with current delivered through the injection needle remains the “gold standard” for identification of the endpoint for needle advancement (25). Although monitoring a motor response during passage of current through the nerve block needle is a standard technique for guiding placement of the needle, there is minimal understanding of the final relationship between needle and nerve when using this method. Theoretically, the smaller the stimulation current required for a distal motor response, the closer the needle tip is to the target nerve. Urmey’s study found that ability to stimulate the nerve at low amperage (e.g. < 0.5 mA) indicates an extremely close position to the nerve (26). However, the exact distance between the needle tip and nerve is not clear. Other previous studies have examined the relationship between the stimulation current level and nerve–needle distance in animal models. The reported findings indicate that the needle was within 3 mm for thresholds of 0.37~0.47 mA in rabbits (27) and within 2 mm for thresholds of 0.9–1.2 mA in cats (28). In the present study, the minimal stimulation current was 0.28 mA when the needle tip contacted the nerve trunk, and the stimulation current gradually increased as the nerve–needle distance changed from 0 to 5 mm. Our findings are consistent with the previous studies.
It has been reported that the extent of injectate dispersion can be observed through anatomical exposure if the injectate is “marked” with a stain (27, 29). The extent of dispersion can be observed and measured in this way, but the volume and temporal distribution of the injectate cannot be measured. In our study, iopromide was used to mark the alcohol because it is hydrophilic and readily soluble in ethanol. With the alcohol marked with iopromide, the volume and temporal distribution of the alcohol dispersion could be evaluated by CT, and the pattern and extent of spread measured by 3-dimensional reconstruction.
It has been reported that patient positioning, needle site, speed of injection, as well as the concentration and volume of local anaesthetic can influence the distribution of neural blockade (20). Hence, we chose different injection speeds, concentrations and volumes as influencing factors to explore alcohol dispersion during blockade of the tibial nerve.
The extent of alcohol dispersion of group Ic was significantly greater than that of groups Ia and Ib. This finding suggested that faster injection speed would lead to the larger dispersion area. A high injection speed will increase the momentum of the injectate, and may explain why the dispersion was greater after higher injection speed. The result suggests that the injection speed should be controlled to decrease the alcohol spread to non-target nerves and muscle.
In clinical practice, 45–100% alcohol is usually used for nerve blockade (30). The present study showed no significant difference between the volumes of spread of different-concentration groups. It has been reported that a low volume and high concentration of local anaesthetic is more efficacious than a high volume and low concentration in the nerve block (31). To increase the chance of success and decrease the risk of non-therapeutic side-effects, a low volume and high concentration of alcohol is recommended for neurolysis.
Alcohol volume is another important factor affecting the extent of dispersion. The extent of dispersion of group IIId were significantly greater than those of the other subgroups. It has been reported that increasing the volume of the injectate can increase pressure in the fascial layer (32), and the higher pressure would “drive” the injectate to spread over a larger area. Hence, the extent of spread from the blockade area appears to be closely related to the volume of alcohol injected. Therefore, accurate location of the needle close to the target nerve is needed so that the smallest amount of alcohol required to elicit a therapeutic effect can be used.
Combined with the above results for the alcohol dispersion influence factor analysis, a high concentration and low volume of alcohol with low injection speed and accurate location of the needle could be recommended for the nerve block.
This study has certain limitations. The small number of subjects, particularly in the nerve localization study, means that these results must be considered preliminary and serve primarily to generate hypotheses. A much larger study, using animal subjects subjected to block experiments, is recommended. This study investigated separately the influence of 3 factors (injection speed, concentration and volume) on the dispersion of alcohol. Thus, further extensive research is needed into the best combination of speed, concentration and volume. In addition, since the present study was performed on animals, confirmation of the results in a study of patients is necessary before these findings can be applied in a clinical setting. However, this is the first study to investigate the nerve–needle distance and stimulation current relationship using a 3-dimensional manipulator, and to determine the influence of alcohol injection speed, concentration and volume on alcohol dispersion, using CT reconstruction.
This study confirmed the hypothesis that there is a positive linear relationship of nerve–needle distance and the minimum electrical stimulation required to elicit a motor response during rabbit tibial nerve blockade. This procedure could be used as an important reference for localization of the injection site. In addition, the study suggests that a low volume of alcohol with a low injection speed can promote dispersion of the injectate, which may help to improve the clinical practice of the alcohol nerve blockade. This is a preliminary study in an animal model and further research is needed before the findings can be applied in clinical settings.
The authors gratefully acknowledge Xu Miao (Department of Medical Imaging of the First Affiliated Hospital of Nanjing Medical University) for his professional assistance with the CT scanning.
Disclosures: This work was supported by a grant from the National Natural Science Foundation of China (No. 81070181) to Xiao Lu.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize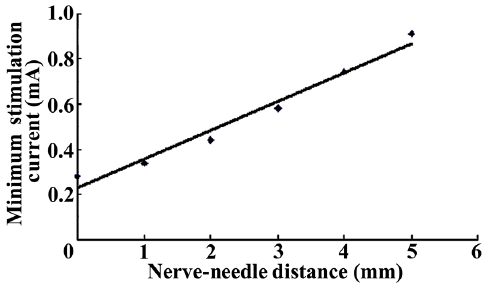 Click to show fullsize
Click to show fullsize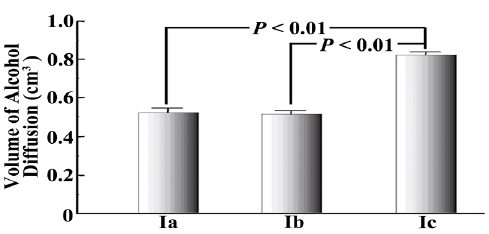 Click to show fullsize
Click to show fullsize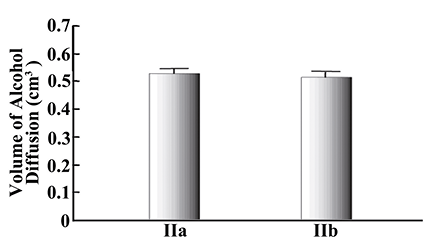 Click to show fullsize
Click to show fullsize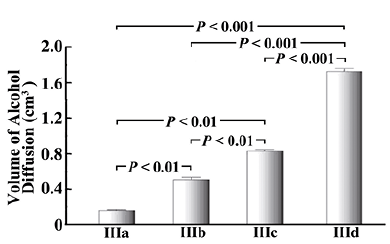 Click to show fullsize
Click to show fullsize