
1Department of Physiotherapy, Epworth HealthCare, Melbourne, 2School of Health and Sport Sciences, University of the Sunshine Coast, Sunshine Coast, Australia, 3Department of Physiotherapy, Singapore General Hospital, Singapore, Singapore, 4La Trobe Sport and Exercise Medicine Research Centre, La Trobe University, 5Victorian Infant Brain Studies, Murdoch Children’s Research Institute, 6Epworth Monash Rehabilitation Medicine Unit, and 7Department of Physiotherapy, University of Melbourne, Melbourne, Australia
Objective: To establish the variability of fast testing velocity and joint range of motion and position when assessing lower-limb spasticity in individuals following neurological injury.
Design: Observational study of people with lower-limb spasticity.
Subjects: Patients with an upper motor neurone lesion (n = 35) and clinicians experienced in spasticity assessment (n = 34) were included.
Methods: The Modified Tardieu scale (MTS) was completed on the quadriceps, hamstrings (2 positions), gastrocnemius and soleus for each participant’s more affected lower limb by 3 assessors. Mean absolute differences (MADs) were used to calculate variability as a measure of reliability.
Results: Variability of peak testing velocity was greater at the ankle joint compared with the knee joint. The greatest MAD for V3 (fast) inter-rater testing velocity was 119°/s in the soleus, representing 29.4% of the mean variable value, and least for the quadriceps (64.3°/s; 18.5%). Inter-rater variability was higher than intra-rater variability for all testing parameters. The MAD for joint end angle ranged from 2.6° to 10.7° and joint start angle from 1.2° to 14.4°.
Conclusion: There was a large degree of inter- and intra-rater variability in V3 testing velocity when using the MTS to assess lower limb spasticity. The inter-rater variability was approximately double the intra-rater variability.
Key words: rehabilitation; lower extremity; central nervous system diseases; reproducibility of results; muscle spasticity; outcome assessment.
Accepted Sep 20, 2018; Epub ahead of print Nov 28, 2018
J Rehabil Med 2019; 51: 00–00
Correspondence address: Gavin Williams, Physiotherapy Department, Epworth Rehabilitation, 29 Erin Street, Richmond VIC 3121, Australia. E-mail: gavin.williams@epworth.org.au
Spasticity is prevalent in many neurological conditions in adults. Accurate assessment of spasticity is important in order to inform clinical decision-making and treatment options. Testing speed is a key component of the spasticity assessment process, but the reliability of how quickly the modified Tardieu Scale is performed has not been reported. This study found that the reliability of testing speed varied between lower-limb muscle groups, and variability was twice as great for inter-rater reliability as it was for intra-rater reliability. These findings have implications for the accurate identification of lower-limb spasticity, and its contribution to mobility limitations.
Neurological injuries, such as stroke, traumatic brain injury and multiple sclerosis, are highly prevalent and place a large burden on the healthcare system (1, 2). Due to the high prevalence of spasticity (3–6), the financial strain it places on the healthcare sector (7, 8), and the impact it has on patient outcomes and quality of life (5, 9), the accurate assessment and management of spasticity has become a major focus of neurological rehabilitation. Clinical measures of spasticity, such as the Modified Ashworth Scale (MAS) and the Modified Tardieu Scale (MTS) are quick and easy to perform with minimal equipment and are used to guide clinical decision-making for interventions such as botulinum neurotoxin A (BoNT-A) injections (10–12). The international consensus statements for the management of disorders of tone recommend the use of the MTS over the MAS as the MTS can more accurately differentiate spasticity from hypertonia (13, 14).
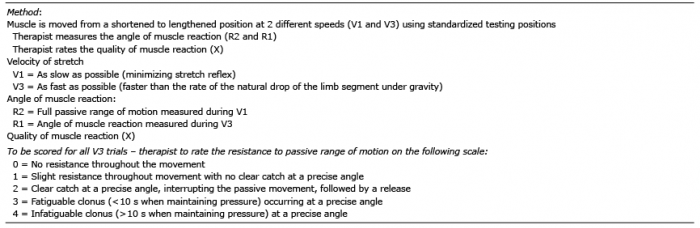
When using the MTS, it has been recommended that the following 3 factors are required to rate the intensity of a spastic response: (i) the strength and duration of the stretch reflex (i.e. X value); (ii) the angle at which the stretch reflex is activated (i.e. R1); and (iii) the velocity necessary to trigger the stretch reflex (15, 16). Studies investigating the reliability of the Tardieu Scale or MTS have primarily reported the inter-rater and intra-rater reliability of the R1, R2 and spasticity angles, with some studies reporting the reliability of the X value (17–22). In comparison, the testing velocity has received little attention and the psychometric properties of the testing velocity during the MTS remain unknown.
It is reasonable to suggest that the velocity of assessment may impact the stretch reflex (18); however, the application of the test in relation to velocity appears to be inconsistent and is likely to vary, depending on the instructions provided to the assessors, the assessor’s strength, the weight or size of the patient limb being tested and the properties of the individual muscle. Velocity is a key component of the definition of spasticity, and the recommended instruction is to move the limb “as fast as possible” during the V3 (fast) component of the assessment. There is no defined or recommended testing speed when testing the major lower-limb muscles, and the most appropriate testing speed during a V3 movement is unknown. The variability surrounding testing speed is also currently unknown, so it seems reasonable to suggest that further research needs to be conducted to investigate the variability of testing velocity using the MTS. The primary aim of this study was therefore to establish the inter- and intra-rater variability of the V3 peak testing velocity when assessing for lower limb spasticity using the MTS in adults who have an acquired brain injury. The secondary aim was to establish the inter- and intra-rater variability of the joint start angles, end angles and total range of motion (ROM) at V1 (slow) and V3, as well as the V1 peak testing velocity when assessing for lower limb spasticity using the MTS.
This study was approved by the Epworth HealthCare Human Research Ethics Committee (HREC 681-15) and the University of Sunshine Coast HREC (S/17/1011). All participants provided written informed consent prior to assessment.
Two groups were recruited to participate in this study: (i) adults with an acquired brain injury or neurological condition; and (ii) clinicians experienced in the assessment of lower limb spasticity.
Group 1: Patients with a neurological condition. A convenience sample of 35 individuals with a neurological condition was recruited to participate in this study. This exceeds the sample size used in previously published studies examining the reliability of other components of the MTS (17, 19–22). Each participant attended a single assessment session, lasting approximately 1.5 h. The inclusion criteria were: (i) diagnosed with a neurological condition, (ii) identified by their treating therapist or rehabilitation consultant as having 2 confirming features of the upper-motor neurological syndrome (radiological or clinical), (iii) attending physiotherapy for mobility deficits related to their neurological condition, (iv) able to have the MTS completed on their affected lower limb, and (v) adults (> 18 years of age) who were able to provide informed consent. The exclusion criteria were concurrent diagnosis of a congenital neurological or peripheral nervous system condition.
Group 2: Clinicians experienced in spasticity assessment. Physiotherapists, rehabilitation consultants and rehabilitation registrars were recruited as assessors from a range of healthcare networks. The assessors were eligible for inclusion if they had at least 3 years’ experience in neurological clinical practice and regularly assessed and treated spasticity within their clinical practice. Each assessor attended an assessment session lasting 4–6 h. Assessors were asked to complete the assessment protocol on 2, 3 or 4 participants pending their availability. This figure was chosen in consultation with a biostatistician and enabled a large, representative group of assessors to be recruited. It was planned that assessors were available to complete a minimum of 3 patient assessments. However, the option of 2 was included to enable the recruitment of several highly-specialised clinicians who were unable to commit to 6 h of testing.
The MTS involves stretching the relevant muscle through its entire ROM at a slow velocity (V1) and then a fast velocity (V3) (18, 23). The end angle during the V1 movement, or full passive ROM, is referred to as R2 and the angle of muscle reaction during the V3 movement is referred to as R1. The spasticity angle refers to the difference between R2 and R1, with a larger spasticity angle indicating a larger degree of velocity dependent spasticity (23). A 5-point scale (see Appendix I) is used to rate the type of muscle reaction (X value) which occurs during the V3 movement, ranging from no resistance through to infatiguable clonus. The MTS was completed on the more affected lower limb of each participant for the gastrocnemius (supine, leg extended), soleus (supine, hip and knee flexed to 90°), hamstrings at 40° hip flexion (supine, full knee flexion), hamstrings at 90° hip flexion (supine, full knee flexion) and quadriceps (prone, leg extended) using standardized testing positions (20, 23). Three V1 and 3 V3 trials were performed for each muscle group by 3 different assessors on each participant, totalling 90 trials per participant (i.e. 3 slow movements and 3 fast movements per assessor for each of the 5 muscle groups tested).
Participants were asked to remain relaxed throughout the assessment and the following instructions were provided to the assessors:
R2: the assessor was asked to move the joint slowly through its full available ROM.
R1: the assessor was asked to move the joint through its full available ROM as quickly as possible. Assessors were instructed to stop at the “point of muscle reaction” during V3. Therefore, R1 reflected the angle of muscle reaction during the V3 movement. No further guidance regarding velocity of assessment was provided.
The assessors were blinded to each other’s assessment to avoid adjustment of testing velocity or joint position based on observing other assessor’s movements. The order of the 3 assessors was randomized for each of the muscle groups tested for each participant to minimise any bias caused by repeated stretching applied by the same therapist.
For each trial, the relevant movement was recorded using a 13-camera 3-dimensional motion analysis (3DMA) system, Optitrack. This system uses small, light-reflective markers which are monitored at a speed of 120 Hz to accurately record joint movement. For each muscle group the markers were placed on specific anatomical landmarks of the lower limb which have been outlined in Table I. Motive Body software, version 1.8.0 (NaturalPoint, Inc., Corvallis, OR, USA) was used to capture the data and label the markers. Data was then exported into a customised programme designed for this project using LabVIEW 2014 (National Instruments, Austin, TX USA) software. This software enabled the start- and end-point of the trial to be selected and was able to quantify joint angles and the velocity of movement using trigonometry. The testing velocity was quantified using joint angular velocity in degrees per second. Once saved, the peak angular velocity, joint start angle, joint end angle and total ROM for each joint movement was exported into a database to be used for analysis.
Appendix I. Modified Tardieu scale
Table I. Anatomical landmarks for marker placement
To assess absolute inter-rater variability, the mean absolute differences (MADs) between any 2 measurements of joint start angle, joint end angle, total ROM and peak testing velocity which were obtained by the different assessors were calculated. To assess absolute intra-rater variability, the MADs between any 2 measurements of joint start angle, joint end angle, total ROM and peak testing velocity which were obtained by the same assessor were calculated (24). Hence, all estimates of the MADs were expressed in the same units as the measurement-of-interest. To compute 95% confidence interval (95% CI) for all MADs, a percentile bootstrapping technique over 500 iterations was used (25). All inter- and intra-rater variability analyses were done in R, version 3.4.4 (R Foundation, Vienna, Austria), using the functions written by Zhouwen Liu (available at http://biostat.mc.vanderbilt.edu/wiki/Main/AnalysisOfObserverVariability).
In addition, the MAD expressed as a percentage difference of the mean variable value was calculated for each muscle group for the primary testing parameter, peak testing velocity. This enabled further reporting of the variability in testing speeds between muscle groups. The MAD expressed as a percentage difference of the mean variable value was not calculated for joint angles, as each muscle group had a distinctly different start- and end-point, which did not enable comparison. For example, if the gastrocnemius has a mean end angle of 10° dorsiflexion and a MAD of 5°, the MAD would correspond 50% of the mean variable value. Whereas, if the quadriceps also had a MAD of 5°, but a mean end angle of 130° knee flexion, the MAD would correspond to only 3.8% of the mean variable value. As such, the percentages for joint angles would not be representative of true variability when comparing the muscle groups.
Group 1: Patients with a neurological condition. Table II outlines the demographics of the 35 patients with a neurological condition who were recruited to participate in this study.
Table II. Participant demographics
Group 2: Experienced assessors. Thirty-four experienced assessors were recruited, including rehabilitation physiotherapists (n = 26), rehabilitation consultants (n = 5), acute physiotherapists (n = 2) and a rehabilitation registrar (n = 1). The assessors had a mean of 14.3 (range 4–40) years of experience. Thirty assessors reported the Tardieu Scale or MTS as their most frequently used clinical scale of spasticity. The remaining 4 assessors reported using the MAS as their most frequently used clinical scale of spasticity.
Table III outlines the mean value across all 35 participants, the MADs with 95% CIs and the MAD as a percentage of the mean variable value for each muscle group, testing speed (V1 and V3) and testing parameter (start angle, end angle, total ROM and peak testing velocity) as a measure of both intra-rater and inter-rater variability.
Table III. Mean absolute differences (MAD) (95% CI) and percentage difference from mean for intra-observer and inter-observer variability
Variability of testing velocity. For all measurements the inter-rater MAD was greater than the intra-rater MAD. These results (Table III) highlight the large variability in V3 testing velocity across a cohort of experienced assessors, especially at the ankle joint. However, as clinical decision-making is primarily based on the results of the V3 trials, the V1 results do not have the same degree of clinical importance as the V3 findings.
Variability of joint end angle. Joint end angle during V3 represented the R1 value, or the angle of muscle reaction when the affected limb was moved “as fast as possible”. As this is an important component of a clinical spasticity assessment it was considered the focus of the secondary aim. Similar to peak testing velocity, the inter-rater variability was higher than the intra-rater variability across all 5 muscle groups for joint end angle.
Variability of joint start angle. When analysing joint start angle, results were similar for both the V1 and V3 trials. Unlike testing velocity and joint end angle, there was only a small difference between inter- and intra-rater variability for gastrocnemius, soleus and quadriceps trials. However, the hamstrings trials at both 40° and 90° hip flexion demonstrated a similar pattern to testing velocity and end angle, with the inter-rater variability almost double that of the intra-rater variability across the V1 and V3 trials.
Variability of total joint ROM. The quadriceps had the greatest inter- and intra-rater variability when analysing total joint ROM. The MAD for intra-rater variability of joint ROM during the V3 quadriceps assessment was 5.7° and the MAD for inter-rater variability was 9.2°. The other muscle groups demonstrated greater inter- and intra-rater variability, with no clear pattern regarding which muscles were assessed with greater consistency.
To our knowledge this is the first study to examine the variability of testing velocity when assessing for lower limb spasticity in individuals following a neurological injury. When examining the primary aim of variability of peak testing velocity during the V3 (fast) movement, the inter-rater variability was almost double that of the intra-rater variability across all of the muscle groups. In a clinical setting it is preferable that one clinician completes all spasticity measures on a particular patient within and between sessions; however, this is often not feasible (20). The findings from this study may have important implications for previously published studies examining the reliability of the MTS, which have reported variable results in regards to the reliability of X scores, R1 values and spasticity angles.
The magnitude of the variability in peak testing velocity appeared to be associated with the muscle group tested. Greater variability occurred during the V3 movements at the ankle joint (gastrocnemius and soleus) compared with the hamstrings, and the lowest variability in testing velocity occurring in the quadriceps muscle. This is potentially problematic as the gastrocnemius and soleus muscles tend to have the highest prevalence of lower limb spasticity and are the most targeted muscle for BoNT-A injection (26). Accurate spasticity assessment is an integral part of pre- and post-BoNT-A injection protocol (14), therefore it is imperative that the assessment process is reliable. An accurate system that is able to provide real-time feedback is required to improve the variability of clinical assessment, particularly testing velocity. Future research should focus on the validation of user-friendly technologies that are able to provide feedback on testing velocity in order to improve reliability. This may provide clarity surrounding the previously identified issues regarding spasticity assessment and assist in achieving optimal patient outcomes.
The mean peak testing velocity during the V3 movement for the 5 muscle groups tested ranged from 320 to 404°/s. These velocities are far greater than the joint angular velocity of the lower limb during functional activities, such as walking. For example, a walking speed of ≥ 0.80m/s is required to achieve unlimited community ambulation (27). A recent study highlighted that the mean speed of ankle dorsiflexion during mid-swing in a cohort of healthy controls walking at a speed of 0.80–0.99 m/s is approximately 150°/s (28). This value is less than half of the mean testing velocities for gastrocnemius (347°/s) and soleus (404°/s), which were produced in this study. Assessors in this study were requested to complete the V3 assessment “as fast as possible” to align with the current MTS testing procedure. This finding highlights the need for further research to be conducted in the field where testing velocity is accurately and reliably applied and matched to functional activities, such as lower limb angular velocity during walking.
One future research direction evolving from the completion of this study involves investigating whether variability of a lower limb spasticity assessment is improved when the assessment is completed at a consistent or nominated speed rather than “as fast as possible”. Further training of the treating team may improve the consistency with which the MTS is applied (29). Controlling for testing velocity would assist in identifying whether different velocities result in changes to R1, spasticity angle and X values and which of these has the greatest relationship to functional activities, such as walking. For example, investigating whether a gastrocnemius spasticity assessment consistently completed at 200°/s produces a more reliable result in terms of X value, R1 and spasticity angle compared with an assessment completed “as fast as possible”. The nominated speed should be proportional to the joint angular velocity during a specific functional activity, such as walking, in order to maximize the functional relevance of the bedside clinical assessment. It is particularly important to ensure that the assessment speed relates to the goal of spasticity intervention; for example, improved walking speed, in order to ascertain a greater understanding between the relationship between spasticity and functional performance to optimize treatment decision-making and patient outcomes. However, as the MTS is administered as a passive test, it remains unclear how the findings of the MTS may relate to muscles that are partially active during walking, and how they may interact with other features of the upper motor neurone lesion.
A large cohort of assessors and patients were recruited to take part in this study, so unlike traditional reliability studies, not all patients were tested by each assessor. This study design was chosen due to practicality, given the time commitment required by each patient and assessor. The negative associated with this method is that it does not allow for traditional analysis techniques, such as correlations, to be performed. However, this study has enabled the evaluation of a large number of both patients and assessors and may well be more representative of spasticity assessment in the “real world”. This design removes the potential bias of studies with only a single or a few assessors. Given the level of experience in spasticity assessment, the large cohort of assessors may, in fact, be considered a strength of this study. In the design of this study, the V3 assessments occurred after the V1 assessments for each muscle group. It is possible that the stretch imposed on the muscle during the V1 assessment may have influenced the V3 results. However, given that the stretch was brief and was not sustained for sufficient time to induce a therapeutic effect, we feel that the impact of VI testing prior to V3 testing was minor.
There were notably fewer rehabilitation registrars or consultants (17.6%) participating in this study compared with physiotherapists (82.4%). There was, however, no reason to expect inter-disciplinary differences in variability. There may be differences in variability based on level of experience, so only experienced assessors who regularly complete spasticity assessment were included. As such, the results may not necessarily be applicable to assessors who are less experienced or to those who primarily complete assessment of the upper limb, such as occupational therapists.
Finally, as the MTS was the chosen outcome measure for this study, the results are specific to Lance’s velocity dependent definition of spasticity (30, 31), and are not applicable to other positive features of the UMNS, such as hypertonia, co-contraction and dystonia. A more recently published definition of spasticity encompasses all positive features of the UMNS, including spasticity, hypertonia, tendon reflexes, dystonia, clonus and spasms under a single umbrella term (11). While this definition may provide a more holistic overview of the UMNS, there are associated challenges in developing an assessment tool that addresses each component of the UMNS. Due to the high prevalence of velocity-dependent spasticity and the profound impact it has on functional outcomes following neurological injury (3–6, 9), it is important that the clinical tools used to assess spasticity are both valid and reliable (11, 13, 14).
There was a large degree of inter- and intra-rater variability in testing velocity when using the MTS to assess for lower limb spasticity. The inter-rater variability was approximately double the intra-rater variability across all 5 muscle groups and the largest variability existed at the ankle joint (gastrocnemius and soleus). Joint start angle, end angle and total ROM demonstrated less variability than testing velocity.
This project was supported by funding obtained from the Australian Physiotherapy Research Foundation Seeding Grant, Royal Automobile Club of Victoria Sir Edmund Herring Memorial Scholarship, and the Epworth Research Institute.


 Click to show fullsize
Click to show fullsize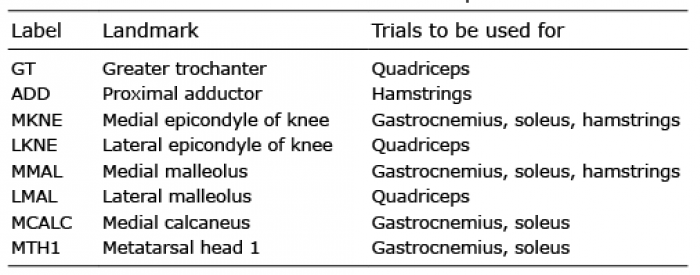 Click to show fullsize
Click to show fullsize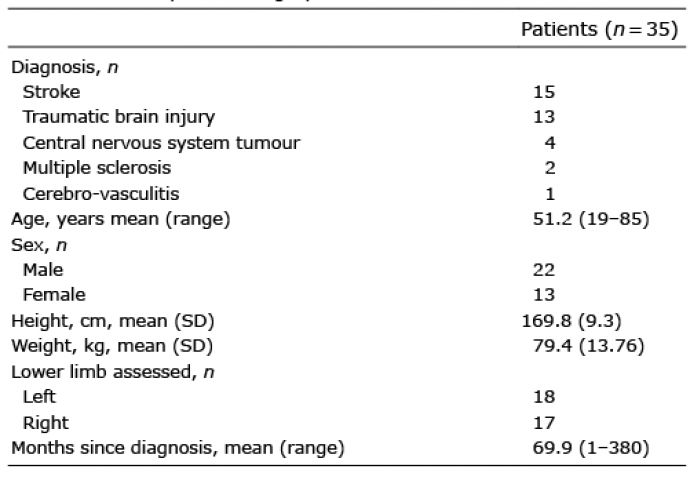 Click to show fullsize
Click to show fullsize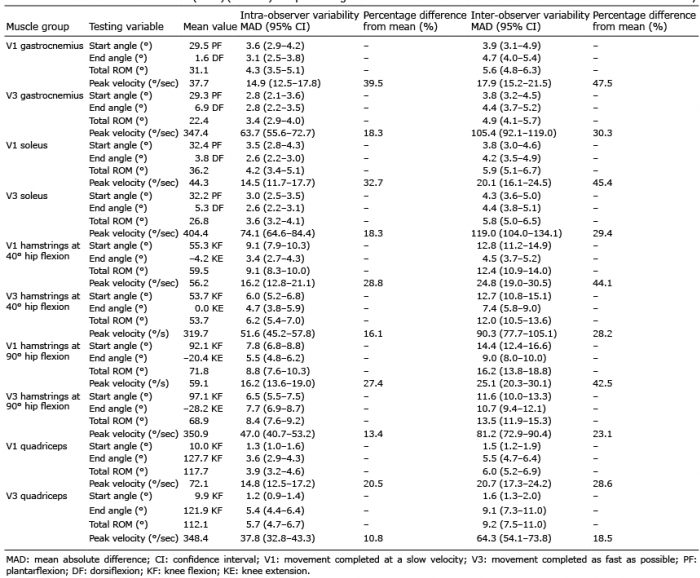 Click to show fullsize
Click to show fullsize