
From the 1Roessingh Research and Development, 2Department of Biomechanical Engineering, and 3Department of Biomedical Signals and Systems, University of Twente, Enschede, The Netherlands
*These authors contributed equally to this article.
Objective: To explore the direct influence of a soft-robotic glove on movement duration and movement execution in elderly people with decreased hand func-tion during a reach-and-grasp task.
Design: Cross-sectional study.
Patients: Eight subjects, aged 55+ years, with decreased hand function.
Methods: The direct effect of the glove was explored using kinematic analysis during a reach-and-grasp task with a light (100 g) and heavy (1,000/2,500 g) cylindrical object, performed with and without the soft-robotic glove.
Results: There was no difference in total movement time between performance with and without the glove. With the glove, the relative time needed to transport the heavy object was shorter, while the relative time needed to grasp the heavy object was longer. In addition, transporting light objects involved a lower peak velocity and larger elbow extension, and grasping the object involved a larger hand opening compared with without glove.
Conclusion: As expected, no positive influence of the soft-robotic glove was found on total movement duration in elderly subjects. The influence of the glove on movement execution varied with movement phase. The positive and negative effects found may be due to a perceived confidence while carrying heavy objects with the glove, or compensation for loss of sensation, respectively. This information can be used to improve the glove design.
Key words: soft-robotic glove; assistive technology; elderly; hand; movement analysis; wearable devices; activities of daily living; upper extremity.
Accepted Feb 4, 2019; Epub ahead of print Feb 15, 2019
J Rehabil Med 2019; 51: 298–306
Correspondence address: Anne van Ommeren, Roessingh Research and Development, Roessinghsbleekweg 33b, PO Box 310, NL-7500 AH Enschede, The Netherlands. E-mail: a.l.vanommeren@gmail.com
The function of the ageing hand decreases as result of loss of muscle mass or age-related diseases, such as osteoarthritis or rheumatoid arthritis. This loss of func-tion results in limitations in performing activities of daily living, such as carrying heavy objects, drinking and eating. A wearable soft-robot glove (the ironHand) has been developed to support grip strength during daily life. This study assessed the effect of the ironHand on movement execution in 8 elderly people with decreased hand function due to age-related diseases. The influence of the glove on movement execution in elderly subjects varied with movement phase. Grasping of a heavy object took relatively longer, while its transport phase was relatively shorter, with the glove, compared with without the glove. These results provide insight into how a soft-robotic glove influences movement, both in a positive and a negative sense. This information could be used to improve the design of wearable robots for the hand.
The function of the ageing hand decreases as result of loss of muscle mass (i.e. sarcopaenia) (1), rheumatoid arthritis or age-related diseases (2, 3). Symptoms of a decrease in hand function in the elderly population often include loss of grip/pinch strength, joint stiffness, decreased range of motion and increased fatigue or pain (4–7). This loss of function results in limitations in performing activities of daily living (ADL), such as carrying heavy objects (4, 8, 9).
An effective approach to improving hand function in daily life is exercise training. Exercise training for older adults with reduced hand strength should consist of components that contain progressive resistance and functional exercise (10). Another approach to improving functional independence is the use of assistive devices (11), especially when exercise treatment does not solve all physical problems and people are left with, or experience, diminished hand function. These assistive devices are available in different shapes and sizes, ranging from simple aids (e.g. a jar opener) that support a specific task, to technological innovations that allow more functionality in daily life. Most of these robotic assistive devices consist of complex, bulky and expensive equipment, while often substituting upper limb movement of the user by robotic action (12).
Wearable assistive devices are focused less on substituting the user and more on assisting use of the hand, where needed, during ADL. An example is the soft-robotic ironHand glove, developed to support grip strength during ADL (13). The soft-robotic ironHand glove has been evaluated regarding feasibility (in terms of user acceptance and usability) (14, 15) and its effect on functional performance (13, 15, 16), showing promising results on user acceptance and usability. Although pinch strength increased significantly, ADL, such as picking up, and moving, objects, were performed slower with the ironHand glove compared with without the glove (15, 16). Clinical scales that score performance time may be less suitable to assess the direct effect of a soft-robotic glove on hand function, since aspects other than performance time can be influenced by use of such a glove, which was developed to support grip strength. For instance, small changes in movement execution can make a difference in functional use of the hand in daily life (17, 18).
Assessing functional tasks through kinematic analysis is useful for evaluating actual functioning of the upper limb in daily life, since kinematics movement analysis is seen as a sensitive and objective method to assess differences in movement execution (19). Therefore, the goal of the present study was to explore differences in movement duration of a reach-and-grasp task with and without the assistance of the ironHand glove. Secondly, the influence of the glove on duration of movement phases, movement smoothness, trunk displacement, peak hand velocity, hand opening and joint excursion of the elbow and wrist were explored.
A subgroup of 8 participants who also participated in an earlier cross-sectional study, investigating the overall orthotic effect of the ironHand glove (13), were included in this explorative study at Roessingh Research and Development (RRD), Enschede, the Netherlands. Inclusion criteria for participation in this study were: at least 55 years of age; experienced difficulties with performing ADL involving the hand; the most-affected hand is the dominant hand; able to perform at least 10° of active flexion/extension movement of the fingers; sufficient cognitive function to understand 2-step instructions; (corrected to) normal vision; and living at home. Exclusion criteria were: severe sensory problems; pain or wounds on the hand that may create problems when wearing the glove; severe contractures limiting passive range of motion; co-morbidities limiting functional use of the arms/hands; insufficient knowledge of the Dutch language to understand the purpose or methods of the study. All participants gave their written informed consent prior to the start of the study. The study was approved by the Medical Ethics Committee in Twente, the Netherlands (CCMO-number NL56746.044.16).
The ironHand glove was developed to support grip strength of the thumb, middle finger and ring finger (Fig. 1) (13). The ironHand system consisted of a 3-fingered wearable soft-robotic glove (Fig. 1A) and a control unit (Fig. 1B) that contains the embedded software to control the amount of force needed to support grip strength and the batteries. The control unit was attached at the belt of the participant (Fig. 1B). Sensory input from pressure sensors (Interlink Electronics, Camarillo, CA, USA) at the fingertips is used to control the amount of extra grip that is regulated by a tendon-driven mechanism. An intention detection logic ensures that the grip is activated in a natural and intuitive way with more grip support supplied when a stronger grip is applied on the object. The gain of the control mechanism (i.e. sensitivity) and maximal amount of support from the glove can be tuned for each individual. In this study, the maximal amount of grip strength support was set at 20 N for each participant and the gain of the control mechanism was tuned for each patient between 2 preprogramed modes based on the participants’ needs and experienced comfort.
Fig. 1. The ironHand system. A: Glove. B: Control unit (14).
Prior to performance of a standardized reach-and-grasp task, maximal handgrip strength was measured (without the glove) to describe the degree of functional limitations of the present sample (20, 21). In addition, information about the participants, such as sex, age, affected body side, dominant side and handgrip strength, was gathered. Next, participants performed a standardized reach-and-grasp task with various weighted cylindrical objects during a cross-sectional evaluation session. Both tasks were performed with the most-affected hand, once with and once without the ironHand glove, to evaluate differences in movement between both conditions with use of a 3D motion analysis systems. Sealed envelopes were used to randomize the order of glove use (first with or without the glove). The primary focus was placed on total movement duration. Secondarily, the effect of the glove on movement duration of movement phases, movement smoothness, trunk displacement, peak hand velocity, hand opening and joint excursion of the elbow and wrist were explored.
Maximal handgrip strength
Maximal handgrip strength of the most-affected hand was measured with a Jamar hydraulic hand dynamometer (Patterson Medical Ltd, Warrenville, IL, USA) with the handle position set at 4 for all subjects. The positioning of each subject was standardized, as described by the American Society of Hand Therapists (22). The participant had to squeeze the handgrip of the dynamometer maximally for 5 s. Handgrip strength was expressed in kg. The subject had 3 attempts, which were separated by at least 60 s rest. The mean of the 3 attempts was used for analysis.
Before participants started with the reach-and-grasp task, they were instructed about how to use the ironHand system properly and they tried it for a few minutes until they felt comfortable with its use.
Next, participants performed the standardized reach-and-grasp task (see Fig. 2 for the experimental set up) to assess movement execution with and without the ironHand glove. In the starting position, each participant was seated with the upper arm aligned with the trunk, the elbow flexed 90° and the palm of the hand positioned on the middle of the table at a predefined start position. The cylindrical object was placed in front of the hand and a platform was positioned within the maximal reaching range of motion of the participant. The task involved: (i) grasping a cylindrical object; and (ii) moving the cylindrical object to the predefined position on the platform; (iii) releasing the object at the platform; and (iv) returning the hand to the predefined start position. The task was performed with 2 differently weighted cylindrical objects (diameter 5 cm) of, respectively, 100 g (light condition) and either 1,000 g or 2,500 g (heavy condition), both with and without the glove. The light condition was included to assess the effect on movement execution without the weight of the object interfering with the execution of movement. The heavy condition was included to simulate an ADL task, in which weight is usually involved. In each condition, the task was repeated 3 times. Prior to the start of the measurements, participants had to lift an object of 2,500 g once to the platform/off the table. If they succeeded, the task was performed with the 2,500 g weight; otherwise, the task was performed with 1,000 g. The order of cylindrical weight was randomized.
Fig. 2. Schematic measurement set up with marker placement.
During all trials, movements of the trunk and upper extremity segments were captured with 6 infrared cameras of the motion capture system VICON MX13+ (Oxford Metrics, Oxford, UK) by recording the position of reflective markers. In total, 15 reflective markers were placed on the hand, arm, thorax and neck (Fig. 2), according to the guidelines of the International Society of Biomechanics (23). In addition, 3 markers were placed on the cylindrical objects to record their movements during the task.
The recorded movement data were analysed using VICON Nexus 1.8.2 and transferred to MATLAB software (R2015a, MathWorks Inc., Natick, MA, USA) for further custom analysis. All position data were low-pass filtered with a second-order Butterworth filter of 20 Hz with zero phase shift.
The recorded data started at the first, and ended at the last moment that the tangential velocity of the hand exceeded 2% of the maximum velocity of the hand based on the second metacarpal marker (24). From that recording, 4 task phases were identified as described below and presented in Fig. 3.
Fig. 3. Division of tangential velocity profile of the hand marker in 5 phases. The horizontal line represents the threshold used for the detection of the 5 phases of the reach-and-grasp task (schematic representation).
The start of the grasping phase was identified through either the position of the cylindrical object relative to the hand or the velocity profile of the object within the timeframe between index 2 and index 3 (see Fig. 3). The indices were chosen at 15% of the maximal velocity of the hand to facilitate the determination of the movement phases. The position of the object relative to the hand reaches a minimum when an attempt is made to grasp. In addition, when the object’s velocity is larger (mean +2 times standard deviation (SD)) for the first time than when the cylindrical object stood still, it is likely that the cylindrical object is moved by an external source. The start was set at the lowest frame number of the 2 options. The end of grasping was defined as the last frame number of:
The start of the reach-with-object phase coincided with the end of the grasping phase. The end of this phase was set at the frame number when the object touched the platform. This event was chosen, because the object was always lifted higher than the height of the platform, after which the impact of the object with the platform caused a minimum in the vertical position of the object.
Releasing started at the end of the reach-with-object phase and ended with the last frame number of either:
The start of the final reach coincided with the end of the releasing phase and the end of this phase occurred at the first time that the tangential velocity of the hand was smaller than 2% of the maximum speed of the hand (24).
The grasping and releasing phases were manually checked by comparing the frame numbers with the visualized VICON data. If the algorithm and manual check deviated more than 0.05 s, parameters associated with that grasp or release phase were removed from further analysis.
The primary outcome measure, total movement duration, was calculated from the initiation of grasping until the end of the final reach.
Secondly, the influence of the glove on time needed to execute each of the 4 phases was calculated in absolute and relative (percentage of total movement time) duration. The time prior to grasping was used to calculate the mean and SD of the motionless cylindrical object. Outcome measures comparable to previous studies performing kinematic analyses of a reach-and-grasp task were calculated to assess the influence of the ironHand glove on movement execution (25–27). Smoothness of the movement, expressed as the number of movement units (NMUs) (28), was calculated over the entire movement. Local minima and maxima in the tangential velocity profile of the marker on the second metacarpal head were searched for the determination of a movement unit. The difference between a consecutive minimum and maximum with an amplitude of 20 mm/s or more indicated a velocity peak that corresponds to the smoothness and efficiency of movement (28). A movement unit was identified when the time between 2 consecutive peaks exceeded 150 ms (24). Maximal trunk displacement (TD) was defined as the maximal 3D displacement of the trunk marker during the task compared with the initial position in rest. Maximum speed during the reach-with-object phase was calculated from the tangential velocity profile of the hand, based on the marker positioned at the head of the second metacarpal. Maximal hand opening prior to grasping was calculated as the maximal distance between the thumb and middle finger marker. The elbow angle during the entire task was calculated from the angle between the vector of the upper and lower arm. Joint excursion of the elbow was determined by subtraction of the smallest angle from the largest angle between those vectors. Maximum elbow extension angle was measured, and determined as the largest angle between the upper and lower arm. Excursion of the wrist was calculated by subtracting the smallest angle from the largest angle between the forearm and hand in flexion and extension direction.
Individual values across participants were averaged per task, glove condition and weight of the cylindrical object. Values per parameter were reported as median with interquartile range (IQR, 25–75th percentile). Due to the small sample size, differences between performance with and without the ironHand glove were non-parametrically tested for all kinematic variables using the Wilcoxon signed-rank test. Effects were considered significant for α ≤ 0.05. No correction for multiple testing was applied, since the nature of the study was explorative (29). Effect sizes were calculated ( indicating a small (r ≤ 0.3), medium (0.3 > r < 0.5) or large (r ≥ 0.5) effect. IBM SPSS Statistics 23 was used for the statistical analysis.
Eight adults between 59 and 79 years old participated in this study (Table I). All participants experienced difficulties in performing daily activities due to heterogeneous diseases that affect hand function. Six participants were diagnosed with rheumatoid arthritis/osteoarthritis, one participant had multiple sclerosis and one had carpal tunnel syndrome. Baseline handgrip strength data indicated “weak”’ handgrip strength for all participants, based on cut-off points related to increased risk of mobility limitations (30). Four participants were able to lift 2,500 g.
Table I. Demographic characteristics
Movement execution parameters averaged over all subjects are shown in Table II. A typical example of task execution, in terms of movement time, movement phases, speed and movement smoothness, is shown in Fig. 4.
Fig. 4. Representation of a typical example of total movement duration, absolute duration of movement phases and movement execution with and without the glove.
Table II. Values of kinematic variables without and with the glove
No negative influence on total movement duration was found (Table II). After division of the movement into phases, an increase in the relative time needed to grasp the object and a decrease in time needed during the reach-with-object phase with the glove compared with without the glove (p = 0.05 and p = 0.04, respectively) was found only in the heavy condition (Fig. 5).
Peak velocity was smaller with support from the glove in the light condition (p = 0.01), but was not seen with the heavy object (Fig. 6).
Fig. 5. Difference scores (with minus without the glove) of the heavy object are presented per participant and group median for the movement time for the grasping, reach-with-object, releasing and reach-to-base phases relative to the total movement time.
Fig. 6. Individual scores per participant (lines) and group boxplot with and without glove of peak velocity (left) and maximum hand opening distance (right), using the light object. Note that the y-axes do not start at 0.
Maximum hand opening was larger in the reach-to-grasp phase of the light object while receiving support from the glove (p = 0.05) (Fig. 6).
No differences in either movement smoothness or trunk displacement were found when comparing with and without the glove in both the light and heavy condition (Table II).
No significant differences in joint excursion of the elbow and wrist were found with the glove compared with without the glove, except for a larger elbow extension excursion and a larger maximum elbow extension angle in the light condition (p = 0.04 and p = 0.01, respectively).
The influence of grip support from the soft-robotic ironHand glove on movement execution of the upper extremity during a simulated reach-and-grasp task with a light (100 g) and heavy cylindrical object (≥ 1,000 g) has been investigated in the present study. As expected, no positive influence of the ironHand glove on total movement duration was found in either of the weight conditions. During the light condition, movements were executed within the lower range of a person’s capacity. In the heavy condition, movements were performed more towards, but still within, the upper limits of functional performance. With the glove, transportation of light objects occurred with a lower peak velocity and higher elbow extension, and grasping of the object involved an increased hand opening, while with the heavy objects relative grasp duration was longer and relative transport duration with the object was shorter, compared with without glove.
So far, few studies have investigated functional performance with and without support from a soft-robotic glove (13–16, 31, 32). Polygerinos’ group assessed the direct effect of a soft-robotic glove on the Jebsen-Taylor Hand Function Test in 1 healthy subject, and reported that it took longer to perform several tasks with the glove compared with normative performance times of healthy subjects without the glove (32). Although this finding is in line with previous studies performed with former versions of the current ironHand glove within the elderly population with or without age-related diseases (13–16), the longer time needed to perform a task with the glove was not seen in the current study.
Although some studies assessed movement execution during ADL in older adults (26), to our knowledge no study has assessed the direct influence of a wearable assistive technology of the hand for older adults on movement execution during a functional task. The light condition was well within the performance range of the subjects. It is possible that it is unnatural to perform a task, which can be performed without support, while wearing a glove that provides unnecessary grasp support and decreases sensation. Therefore, compensation for an unknown situation or decreased sensation because of wearing a glove might have affected the performance in the light condition. Peak velocity of the hand during the task was lower and elbow excursion was larger with the glove in the light condition compared with without the glove.
On the other hand, when participants had to perform a task closer to the upper limits of their functional capacity, the disadvantageous influence regarding peak velocity was absent. Moreover, transport of the heavy object, the phase in which the glove supports the user most, was faster with the glove compared with without the glove. This suggests that grasp support can be beneficial for older adults while performing a task close to the limits of their functional capacity. The participants might have felt more confident when using the glove with the heavy object, enabling them to increase their movement speed when holding the object. The high usability score and positive attitude towards the ironHand glove observed in previous studies with the glove (13) might support this improved confidence experienced when grasping and lifting objects.
Although participants needed relatively less time to transport the heavy object with the assistance of a soft-robotic glove compared with without, a relatively longer time was needed to grasp the heavy object with glove support. It is likely that the observed positive effects (relative shorter transporting phase) were counterbalanced by the negative influences (relative longer grasping time), resulting in no differences in total movement time, as observed in the present study. This might also play a role in the lack of improved performance time on the functional level with the glove, as was found in previous studies (13, 15, 16). One plausible explanation for the relatively longer grasping phase is that the participants waited for feedback from the system, in the form of noticeable force exerted on their hand, before they felt confident enough to lift the object. In this case, the time it takes between registration by the glove’s control system that support is needed and actual force exertion being perceived by the participant is represented as a delay during grasping of the object. Therefore, it is beneficial to explore possibilities to reduce the time between grasp initiation and actual force transfer of the glove on the hand. One option is to detect grasping movements before actual contact with the object is made. To realize this, reach must be distinguished from reach-to-grasp movements. Possible ways for exploration of earlier grasp intention detection are with the use of electromagnetic sensors, inertial measurement units, bend sensors and pressure sensors (33–35).
A factor that might have contributed to the extent to which effects were (not) observed in the present study is the time dedicated to familiarization. Although participants used the glove for approximately 10 min before starting the reach-and-grasp tasks until they felt comfortable with it, it is possible that they did not reach its full potential (36). Radder et al. (16) reported that functional performance time of older adults with hand function problems with a previous version of the ironHand glove increased during no more than 3 repetitions up to the level of unsupported movements, despite an initial slower performance with the glove. Nevertheless, in the study of Radder et al. (16) no plateau in performance was reached yet after 3 repetitions, suggesting that performance time may have improved further beyond the familiarization time applied in the present study. Although, so far, no studies have assessed the effect of prolonged use of an orthosis that supports grip function in older adults, it is known that training is essential to improve the performance of older adults with declined hand function (10). Therefore, prolonged low-intensity training with an assistive soft-robotic glove in a home setting might enhance hand function in older adults. Additional research, in which the ironHand glove is used for a prolonged period in ADL, is planned to obtain more insight into its possible effects on functional performance.
A few limitations of this study should be taken into account when interpreting the results and generalization towards ADL. First, this study is only performed in a small group (n = 8) of participants (only women) with diverse pathologies. Secondly, it might be that participants were not completely familiarized with use of the system (as discussed above). Thirdly, even though we attempted to simulate an ADL task, it is not possible to mimic an ADL situation precisely and still standardize it for research purposes, due to additional factors, such as cognitive load and environment, influencing task performance. Subsequent testing in a home situation is suggested to assess the effect of the glove on functional outcomes and its impact on every-day life. Fourthly, the task was only partly adapted to the participants’ abilities. Although the capacity of participants was considered by adjusting the workspace to their reaching range of motion and selecting the heaviest object they could lift, the personal maximum performance was not precisely tested.
All in all, when exploring the effect of the wearable soft-robotic ironHand glove on movement execution in elderly people, both positive and negative influences of using a soft-robotic glove during a simulated ADL task, in terms of movement kinematics, were found. In contrast to previous studies, a negative influence on total time needed to perform a task was absent, using either light or heavy objects. In a situation in which an ADL, such as holding or carrying tableware, groceries or other weighted household items, is represented (object ≥ 1,000 g), participants might have adapted their movement execution due to the perceived confidence while wearing the glove. However, compensation for an unknown situation or loss of sensation due to wearing a glove may have affected the performance of the reach-and-grasp task that can easily be performed without assistance (100 g object). Longer usage of the glove in ADL might overcome effects that are present due to unfamiliarity with glove usage. The information obtained can be used for improving the design of wear-able robots for the hand, and to better understand how these systems can be applied successfully in practice.
This study is partly funded by the Active and Assisted Living (AAL) programme (AAL-2013-6-134), via ZonMw (the Netherlands), Vinnova (Sweden) and SERI (Switzerland).
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize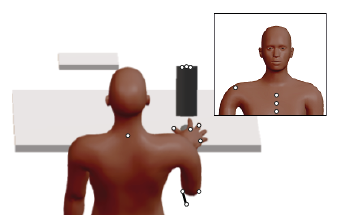 Click to show fullsize
Click to show fullsize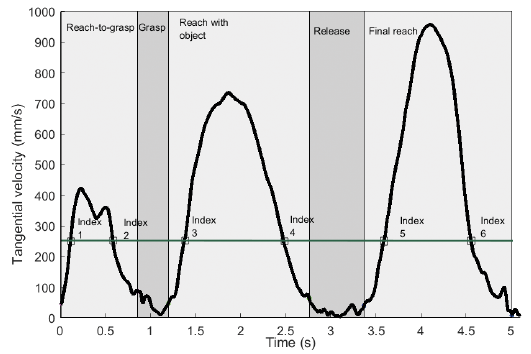 Click to show fullsize
Click to show fullsize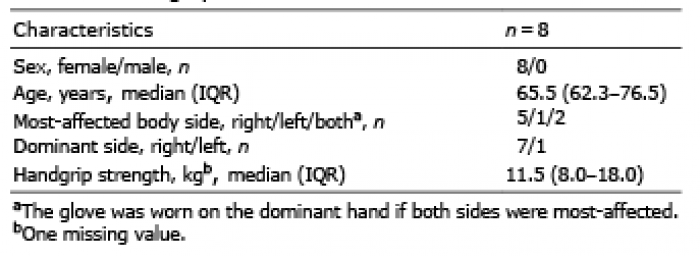 Click to show fullsize
Click to show fullsize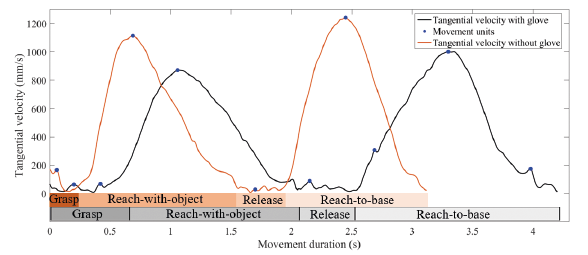 Click to show fullsize
Click to show fullsize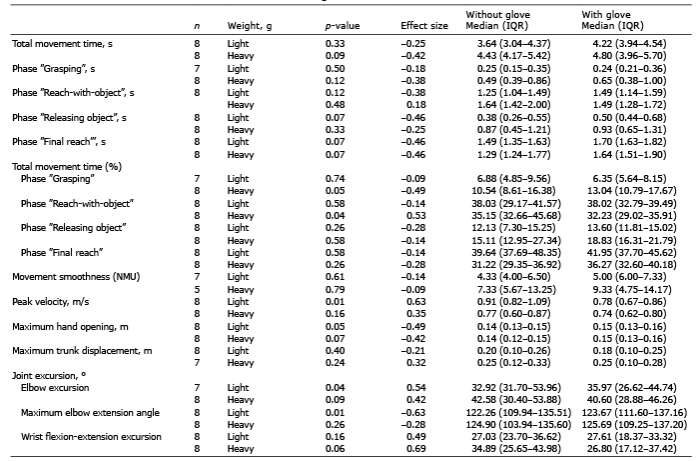 Click to show fullsize
Click to show fullsize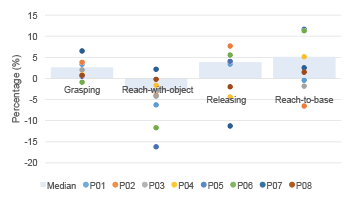 Click to show fullsize
Click to show fullsize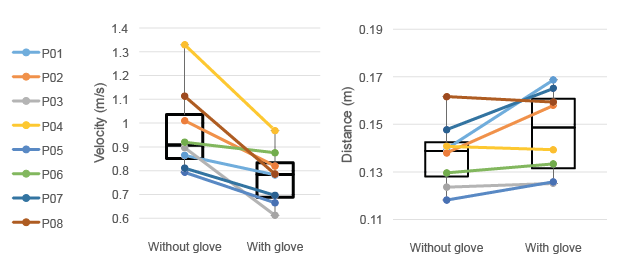 Click to show fullsize
Click to show fullsize