
From the 1Monash Institute of Cognitive and Clinical Neurosciences, School of Psychological Sciences, Monash University, 2School of Psychology and Public Health, La Trobe University, 3Monash-Epworth Rehabilitation Research Centre, Melbourne, 4Translational Public Health and Evaluation Division Stroke and Ageing Research, Department of Medicine, School of Clinical Sciences at Monash Health, Monash University, Clayton, 5Stroke Division, The Florey Institute of Neuroscience and Mental Health, University of Melbourne, Heidelberg, 6Rehabilitation and Aged Care, Medical Program, Monash Health, Melbourne, 7Epworth-Monash Rehabilitation Medicine Unit, Southern Medical School, 8Department of Epidemiology and Preventive Medicine, Monash University, Victoria, and 9Allied Health, Royal Melbourne Hospital, Melbourne, Australia
Objectives: Memory deficits are common after stroke, yet remain a high unmet need within the community. The aim of this phase II randomized controlled trial was to determine whether group compensatory or computerized cognitive training approaches were effective in rehabilitating memory following stroke.
Methods: A parallel, 3-group, single-blind, randomized controlled trial was used to compare the effectiveness of a compensatory memory skills group with restorative computerized training on functional goal attainment. Secondary outcomes explored change in neuropsychological measures of memory, subjective ratings of prospective and everyday memory failures and ratings of internal and external strategy use.
Results: A total of 65 community dwelling survivors of stroke were randomized (24: memory group, 22: computerized cognitive training, and 19: wait-list control). Participants allocated to the memory group reported significantly greater attainment of memory goals and internal strategy use at 6-week follow-up relative to participants in computerized training and wait-list control conditions. However, groups did not differ significantly on any subjective or objective secondary outcomes.
Conclusion: Preliminary evidence shows that memory skills groups, but not computerized training, may facilitate achievement of functional memory goals for community dwelling survivors of stroke. These findings require further replication, given the modest sample size, subjective nature of the outcomes and the absence of objective eligibility for inclusion.
Key words: cognition; rehabilitation; episodic memory; memory; stroke; clinical trial phase II.
Accepted Feb 6, 2019; Epub ahead of print Feb 28, 2019
J Rehabil Med 2019; 51: 343–351
Correspondence address: Renerus Stolwyk, Monash Institute of Cognitive and Clinical Neurosciences, School of Psychological Sciences, Monash University, Melbourne, Australia. E-mail: rene.stolwyk@monash.edu
Memory problems are commonly reported following stroke but receiving help for these difficulties remains a high unmet need among survivors. Two different approaches to memory rehabilitation are available: memory skills group training and computerised cognitive training; however, it is unclear which approach is more effective. This study compared these two approaches in 65 stroke survivors who all reported memory difficulties. We found that participants who received memory group training were more likely to achieve their memory improvement goals than those who received computerised cognitive training. It was concluded that memory skills group training may be a more effective approach to improve memory function in daily life following stroke, but more research is required.
Memory impairment is one of the most commonly reported cognitive consequences of stroke (1) and can compromise rehabilitation engagement (2). Despite this, support for memory problems remains a high unmet need within the community (3) and has been identified by patients, researchers and clinicians as a high-priority research area (4).
Memory skills group (MSG) training and computerized cognitive training (CCT) are commonly used approaches to rehabilitate memory. Although both share the fundamental goal of improving everyday memory outcomes (5), there are a number of key differences between these interventions. CCT adopts a restorative approach to rehabilitation, with the theoretical goal of restoring underlying impairment through cognitive exercises (6). Repetitive drill and practice style activities are purported to result in everyday functional gains, although there remains no robust evidence of this transfer (6). By contrast, MSG interventions take a compensatory approach to rehabilitation with a theoretical aim of lessening the disabling impact of impairment (7). In addition, the format of delivery differs. CCT training tasks are generally completed individually, with associated well-recognized advantages of low cost, wide availability and potential for at personalized use at home (8). MSG intervention is facilitated by a trained clinician and is delivered face-to-face in a group format, due, in part, to increased recognition of the multifaceted nature of memory dysfunction and limited economic resources (9).
While a number of comprehensive reviews have explored best-practice recommendations for cognitive impairment following acquired brain injury (10, 11), only a minority of studies included in these reviews were conducted in stroke-only samples. Consequently, the long-held view that MSG training is the treatment of choice in rehabilitating memory has been largely speculative post-stroke and appears to have been based on an absence of evidence, rather than evidence of absence for the effectiveness of CCT (5). The aim of this study was to compare the effectiveness of CCT and MSG training in community dwelling survivors of stroke in achieving individualized, functional memory goals. A further aim was to explore the effect of training on secondary measures of objective, neuropsychological memory tasks and subjective memory ratings. In addressing these aims, we intended to maintain ecological validity by evaluating the interventions as they are clinically implemented (rather than transforming them to be experimentally matched with each other on characteristics such as group vs individual format), with the goal of facilitating clinical translation. We hypothesized that intervention participants (i.e. CCT and MSG) would show greater improvement in performance on outcome measures than waitlist control participants (WC). Given the proposed mechanism of action of each approach, we also hypothesized participants in the CCT group would show greater improvement on neuropsychological tests of memory, while participants in the MSG would show greater improvement on functional measures of memory and strategy use.
This study was a parallel, 3-group, single-blind randomized controlled trial with outcomes assessed up to 3 months following randomization. Initial power analysis for a 3 × 3 multivariate analysis of variance (MANOVA) was conducted using G*power (v3). Analysis indicated that 52 participants would be necessary to detect a medium effect size (f = 0.35) (12) with power of 0.80 and alpha of 0.05. With an anticipated attrition rate of 20%, a total sample size of 65 participants was indicated. Community dwelling survivors of stroke were recruited through advertising in local newspapers, community clinician referrals and the Australian Stroke Clinical Registry between January 2015 and January 2017 (AuSCR) (13). Responding individuals completed a telephone screen to check whether the eligibility criteria were met.
Inclusion criteria were: history of stroke confirmed by neurological examination and brain imaging at least 3 months previously, and self or close other (i.e. relative) reported everyday memory complaints. Exclusion criteria were: (i) physical impairment preventing access to intervention, (ii) inadequate computer proficiency limiting computer use, (iii) severe cognitive or communication deficits (secondary to aphasia or English as a second language) impacting engagement and (iv) history of other neurological or psychiatric condition impacting cognition. Exclusion criteria were determined on the basis of clinical judgment, aided by review of available medical records by a researcher trained in the study protocol. In cases where eligibility was unclear, consultation occurred with DW and RS who are both experienced clinical neuropsychologists and researchers. Participants were not compensated financially for their time, but were provided the intervention free of charge.
Ethical approval to conduct the study was granted by relevant ethics committees and the project was registered with the Australian New Zealand Clinical Trials Registry (ACTRN 12616001056482). The data that support the findings of this study are available from the corresponding author on request.
At baseline, all participants completed measures of cognitive functioning, computer proficiency, and everyday functioning. Neuropsychological measures included the Test of Premorbid Functioning (TOPF) (14) to estimate premorbid intelligence and the Montreal Cognitive Assessment (MoCA) (15) to provide a gross measure of general cognitive functioning. The short form of the Computer Proficiency Questionnaire (CPQ) (16) was used to assess computer proficiency, while the Nottingham Extended Activities of Daily Living scale (NEADL) (17) was used as a measure of daily living functional independence.
Attainment of personal, memory-specific rehabilitation goals was assessed using Goal Attainment Scaling (GAS) (18). GAS was selected as the primary outcome measure due to its flexibility in managing heterogeneous outcomes and ability to explore functionally meaningful change; which arguably represents the fundamental goal of rehabilitation, irrespective of theoretical approach (19). Goals were developed collaboratively with participants using SMART principles (Specific, Measurable, Attainable, Realistic, Timely) according to established guidelines for clinical use (20). Participants were encouraged to set 2 memory-specific goals with a trained researcher. The scoring method originally proposed by Kiresuk & Sherman (18) was adopted due to its established sensitivity to change in rehabilitation outcomes following stroke (21). Accordingly, a standard 5-point scale (–2; a lot less than expected, 0; at expectation, +2; a lot more than expected) was employed. In line with current recommendations for use (20), baseline achievement was set at –1 to allow for deterioration, unless there was no clinically conceivable worse outcome, in which case baseline performance was set at –2. Raw achievement scores were aggregated across memory goals and converted to a standardized T-score (20). All goals were set with participants prior to randomization to minimize bias. Common participant goals are presented below in Table I.
Table I. Commonly described memory goals and example baseline attainment
Neuropsychological Measures of Memory. The Rey Auditory Verbal Learning Task (RAVLT) (22) and the Brief Visuospatial Memory Test-Revised (BVMT-R) (23) were used to measure verbal and visual learning and memory, respectively. Total words recalled over learning trials (total learning), and number of items spontaneously recalled following a 30-min delay (delayed recall) were examined. All raw scores were converted to standardized z-scores using age- and education-based normative data to enhance clinical translation (22, 23). The Royal Prince Alfred Prospective Memory Test (RPAProMem) (24) was used to explore prospective memory. This measure consists of 2 time- and event-based prospective memory tasks, assessed at short (i.e. within the assessment session) and long (i.e. after the session) time intervals. Responses were scored out of 3 for each task (maximum total score of 12). Parallel forms of all aforementioned measures were used across sessions to minimize practice effects. Finally, the Symbol Span subtest from the Wechsler Memory Scale–IV (WMS-IV) (25), and Digit Span Backward subtest from the Wechsler Adult Intelligence Scale-IV (WAIS-IV) (26) were used to examine spatial and verbal working memory, respectively. Raw scores were converted to age-scaled scores using manual norms.
Subjective memory. Subjective memory failures were measured using the Everyday Memory Questionnaire- Revised (EMQ-R) (27) and Part A of the Comprehensive Assessment of Prospective Memory (CAPM) (28). The EMQ-R is a 13-item scale developed as a self-report measure of memory failures in everyday life, evaluated with a 5-point Likert scale with higher scores representing greater memory complaints. The CAPM part A is a 32-item questionnaire designed to evaluate everyday prospective memory lapses in individuals with acquired brain injury. Each item is rated on a 5-point Likert scale, with higher scores representing more frequent memory failures. Both participants and a significant other completed the CAPM. On both subjective memory questionnaires, raw scores were summed to derive a total score reflecting the frequency of everyday and prospective memory failures. Lastly, total number of internal and external strategy use was examined using a questionnaire of strategies implemented in daily life (29).
Following informed consent, enrolled participants completed baseline assessment and were randomized into 1 of 3 treatment arms; MSG, CCT or WC. Waitlist participants were offered a memory intervention of their choice following project completion. Randomization was performed with an online random sequence generator (http://www.randomization.com) in advance of the study and transcribed into randomly permuted fixed block sizes of 6 by an independent researcher. Participants were assessed immediately following intervention and at a 6-week follow-up by a researcher independent of intervention delivery and blinded to treatment arm allocation. Assessment occurred at participants’ homes.
Making the Most of your Memory: An Everyday Memory Skills Program (29). An adapted version of this manualized memory group was selected as the compensatory intervention. The group programme involved 6 2-h sessions (including breaks) held weekly at a university psychology training clinic (see Table SI1 for session outline). Sessions were facilitated by an experienced neuropsychologist (DW) with the assistance of 2 provisional psychologists. Groups included a minimum of 3 and maximum of 8 participants and all sessions were video-recorded. Group facilitators were blinded to participants’ individual GAS results and the manualized intervention was not modified to specifically address these goals. Treatment fidelity was assessed using a checklist of key objectives for each session, with all treatment objectives achieved across groups.
LumosityTM was selected as the computerized cognitive training intervention due to its popularity (30) and adaptability for research. LumosityTM is a commercially available CCT programme accessible online (www.lumosity.com). Game complexity increases and decreases systematically based on the individual’s performance (i.e. is adaptive). Training materials for the current research were prepared and funded by Lumos Labs in collaboration with researchers. Only those games targeting memory functioning were selected (see Table SII1 for game description). The order in which games were presented was varied across training days to maximize engagement. Participant compliance was monitored remotely through weekly examination of total days trained. To maximize compliance, researchers were in weekly phone contact with participants. Dose was set at 30 min a day, 5 days a week for 6 weeks (31).
In line with Consolidated Standards of Reporting Trials (CONSORT), analyses were conducted using an intention-to-treat approach. Data analyses were conducted using Stata Statistical Software v14.2 (StataCorp., Texas, USA). Demographic, prognostic, and baseline memory performance across all outcome measures were compared across groups using 1-way analyses of variance (ANOVAs), and χ2 analyses. Random-effects regression was used to compare the trajectory of change in outcome measure performance over time between groups. Models were fitted with assessment time-point and group allocation as fixed effects, while participants were modelled as a random effect. A 2-sided alpha value of less than 0.05 was considered statistically significant. Pairwise comparisons and ANOVAs with Bonferroni correction were computed to explore between-group differences at each time-point. Treatment effect size, defined as the magnitude of change from baseline within groups, was estimated with Cohen’s d, based on output from regression models (32).
A total of 136 individuals responded to the advertisement (30% recruited via AuSCR, see Fig. 1). Seventy-one individuals were excluded from participation (52% exclusion). The remaining 65 individuals consented to participate and were randomized into MSG (n = 24), CCT (n = 22) or WC (n = 19) groups. There was a 21% rate of attrition at the 6-week follow-up (27%, 25% and 11% drop-out rate for CCT, MSG and WC, respectively).
Fig. 1. Flow of participants through each stage of the study. CCT: computerized cognitive training; MSG: memory skills group; WC: waitlist control.
While all participants self-reported memory difficulties, 64.6% also displayed evidence of memory impairment on neuropsychological measures, defined as at least 1.5 standard deviations (SD) away from premorbid estimates on at least 1 memory task. Groups were matched on demographic and baseline memory performances (see Table II). However, there were significantly more left hemisphere stroke survivors in the MSG and a significantly greater proportion of patients with haemorrhages in the CCT training condition relative to other groups. To account for this, these stroke characteristics were included as covariates when modelling outcomes.
Table II. Participant demographic, stroke and baseline memory variables
With respect to treatment adherence, 2 participants missed one MSG session, while the remaining participants attended all sessions (83%). Participants allocated to CCT training completed a mean of 25 training sessions (83%; SDtraining=16.01; range 3–43 sessions). The majority (74%) of WC participants preferentially selected LU as their intervention of choice following completion of the project.
Attrition analysis suggested that those participants who withdrew or could not be re-contacted for assessment reported significantly more prospective memory failures than completers (see Table SIII). No other significant differences were seen.
Primary outcome: goal attainment. There was a statistically significant interaction between group and time-point when modelling change in goal attainment scores in favour of the MSG (Table III, Fig. 2). Post-hoc analysis demonstrated that participants allocated to the MSG showed significantly greater attainment of individualized memory goals between baseline and post-intervention assessment relative to WC (see Table SIV1). Gains were maintained at follow-up, with participants allocated to the MSG displaying significantly greater attainment of memory goals relative to both CCT and WC participants. Descriptive analysis found that 83% of participants in the MSG reported attaining at least one memory goal (40% achieved both memory goals), while 60% and 70% of participants in WC and CCT described attaining a memory goal, respectively.
Table III. Estimated marginal means and effect sizes for goal attainment
Fig. 2. Estimated marginal means (±SE) of goal attainment T scores by group controlling for aetiology and hemisphere of infarction. **Significance at p≤0.01.
Objective memory. Visual and verbal new learning and memory performances did not significantly differ across groups following intervention (see Table IV). Regarding verbal WM, there were no significant interaction effects when modelling outcomes. There was a significant interaction between intervention and time when modelling visual WM outcomes, whereby participants allocated to the MSG demonstrated significant improvement from baseline performance at post-intervention and follow-up. However, the performance of MSG participants did not differ significantly from WC or CCT participants at any time-point.
Table IV. Estimated marginal means and effect sizes for objective memory outcomes
With respect to PM, there was a significant interaction between group and time. Post-hoc analysis demonstrated that participants allocated to the MSG showed significantly greater improvement in PM between baseline and post-intervention relative to CCT participants. However, this effect was not maintained at follow-up. Model significance for objective measures can be found in Table SV1 and is shown in Fig. S11.
Objective outcomes were analysed using both raw and standard scores with minor discrepancies noted. Specifically, aetiology of stroke was no longer a significant covariate when modelling outcomes on the RAVLT total learning, while hemisphere of infarction was a significant covariate when modelling change in verbal working memory. No other differences in outcome were found. The decision was made to present findings as standard scores, in line with the clinical translation goals of this paper.
Subjective memory. There was a significant interaction between group and time-point when modelling change in subjective everyday memory (see Table V). Post-hoc analysis established that participants in the MSG showed a significant reduction in the frequency of everyday memory complaints following the intervention. This interaction was, however, no longer significant at follow-up and did not differ from WC or CCT participants. Subjective PM did not significantly differ between groups following intervention. However, a significant group by time interaction was found when modelling change on relatives’ reported PM failures, whereby participants allocated to CCT intervention displayed a significant reduction in frequency of close-other reports of PM failures following intervention. Improvement was not maintained at follow-up.
Table V. Estimated marginal means and effect sizes for subjective memory outcomes
Regarding self-reported strategy use, there was a significant interaction seen when modelling change in frequency of internal strategy use. Although all participants reported a significant increase in strategy use at post-assessment, this improvement was only maintained at follow-up for participants allocated to the MSG. While all participants described improvement in external strategy use over time, there was no significant interaction. Model significance for subjective measures can be found in Table SVI1 and is shown in Fig. S21.
To our knowledge, this study is the first phase II RCT comparing real-world rehabilitation outcomes of CCT and MSG rehabilitation in stroke survivors. Participants in the MSG reported significant improvement in goal attainment above WC following intervention. These gains were maintained at a 6-week follow-up, with participants showing significant improvement beyond both CCT and WC participants at this primary time-point. The magnitude of group differences suggested a large treatment effect (see Table III). These findings provide preliminary support for the generalization of MSG outcomes to real-world improvements in memory functioning; a finding not reported previously. While participants in the CCT group described some increase in goal attainment, performance did not improve beyond WC at any time-point. These results do not support the generalization of training to real-word benefit; a finding consistent with recent commentary (6, 8). Within the context of equivocal memory rehabilitation outcomes to date (10), this study meaningfully contributes to the extant body of literature through confirmation of real-world improvement following group intervention training the use of compensatory memory strategies and highlights the potential utility of MSG in clinical practice. We acknowledge that multiple cognitive deficits may affect memory functioning after an acquired brain injury, such as stroke. Unlike CCT, which specifically targets an isolated domain of cognition, the MSG provides a more holistic approach to rehabilitation and may be better for addressing the multifaceted nature of memory deficits following stroke. There is promising evidence to indicate that CCT may be effective in remediating impairment in attention and executive functioning in acquired brain injury (33); 2 cognitive domains known to be necessary for everyday memory functioning. Future research should seek to explore the real-world benefit of more globally targeted CCT on everyday memory functioning.
Regarding secondary outcome measures, participants in the MSG displayed a significant improvement in performance on visual WM and PM tasks, showing greater improvement than CCT participants following intervention. However, group differences ceased to be significant at follow-up. Findings do not provide support for the sustained effects of either intervention on neuropsychological measures of memory. Although non-significant, this finding is not unexpected within the theoretical framework of compensation. By contrast, results are surprising within the framework of restoration; whereby reduction in memory impairment represents a necessary precursor to the transfer of training (6). Findings are discrepant from previous CCT studies in which improvement in objective memory has been described (34–36). Possible explanations for inconsistency in findings may relate to discrepancies in training platforms, samples and design of these studies. Most previous CCT studies have used CogMed QM training, which selectively targets WM. In addition, previous studies have commonly used mixed aetiology samples (35, 36), which limits generalization to stroke. Moreover, the most widely cited stroke CCT study (34) failed to incorporate follow-up assessment, an active control or blinded assessors. Limitations are particularly pertinent given the vulnerability of CCT to placebo effects (6) and may account for disparate findings. Given that LumosityTM is arguably the most popular and widely recognized CCT programme currently available (30) and purports to remediate everyday memory, its effectiveness requires ongoing empirical validation.
There were short-term effects of MSG intervention on subjective ratings of everyday and memory failures and CCT close other ratings of PM difficulties, though these were not seen at follow-up. Within this context, it is possible that the inclusion of “booster sessions” to consolidate treatment gains may be necessary to maintain the benefits of the MSG intervention over time; a finding previously described in brain-injured samples (37). Regarding self-reported strategy use, while all participants reported a significant increase in strategy use over time, improvement was only maintained for participants allocated to the MSG. This interaction was not seen for external strategy use. These findings suggest that MSG, but not CCT, may be effective in improving the frequency of internal strategy use; a finding supported by recent qualitative analysis (38). Group discrepancies in strategy use may relate to the context in which this information is acquired. While participants in the MSG were taught strategies in a structured group format and actively encouraged to apply them to everyday tasks, participants in the CCT intervention appeared to spontaneously implement internal strategies to improve their task performance. This adoption of strategies in CCT has been previously described, and has been suggested as contributing to the transfer of computerized interventions to untrained activities (39). Nevertheless, the likely variable manner in which participants implemented these strategies to everyday tasks may account for their lack of sustained effectiveness and everyday applicability. Findings are consistent with qualitative feedback from CCT participants who considered strategy use as “cheating” and failed to see the generalization to real-world strategy use (38). Future research should seek to explore the efficacy of combined CCT with compensatory memory strategy training to encourage generalization of spontaneously implemented strategy use.
Some methodological limitations of this study are acknowledged. Importantly, the study compared group, centre-based training of compensatory strategies with individual, home-based computer training. Consequently, we were unable to control for the effects of group socialization not present in CCT. Thus, we cannot rule out the possibility that some of the improvement evident in MSG participants may have resulted from group participation, rather than group content per se. However, this was a deliberate decision on behalf of researchers to maintain ecological validity through delivery of the interventions as they are clinically intended, to facilitate the translation of findings. Similarly, although the MSG is a manualized intervention, participants allocated to this condition may have had the opportunity to raise specific goals, not seen in CCT participants. Future research should seek to explore the impact of group delivered CCT to assist in delineating the influence of content vs medium of delivery.
The subjective nature of several outcome measures may be prone to measurement error. Regular interaction with researchers for intervention, but not WC participants may also have led to Hawthorne effects, particularly given the subjective nature of outcomes (40). However, these effects do not explain differences between MSG and CCT groups, which remains the aim of this paper. Similarly, participants in the study often had difficulty specifying memory goals, particularly given their abstract nature. Notwithstanding, participants appeared to understand the process of goal setting, and potential difficulties were controlled for across groups. Interestingly, the majority of WC participants described achieving a memory goal in the absence of a structured intervention. Results highlight the potential therapeutic effect of goal setting but also support the added benefit of MSG training beyond these benefits. Findings further demonstrate the need for a control condition to robustly explore the impact of health interventions.
In addition, eligibility was not limited to individuals with objective memory impairment, which may explain the relatively mild nature of memory impairment in this sample. The inclusion criterion of subjective memory complaints was selected deliberately to reflect the patient population that is most likely to present for memory rehabilitation services. Access to memory rehabilitation services is not usually contingent on objective memory impairment from a clinical perspective. Our primary aim was to understand if these interventions improved everyday memory function irrespective of the underlying cause of change. Nonetheless, findings may not be generalizable to individuals with more severe memory impairment. Future research should seek to explore factors that may impact treatment response (e.g. mood and severity of objective impairment).
Lastly, our sample size and exclusion criteria limit generalizability. Although the sample size was considered sufficient to power this Phase II exploration, replication in a Phase III trial with a larger sample remains an important goal. Our modest sample size may also account for chance differences on prognostic factors (i.e. hemisphere and aetiology of infarction), which may mediate the relationship between intervention and outcome (41). Predictors of treatment response including location and aetiology of stroke will be examined in a separate study. In addition, exploration of the cost-effectiveness of these 2 interventions is being explored separately and will further assist in facilitating ecological translation.
These limitations noted, the results of this study support the use of MSG training to improve everyday memory functioning for survivors of stroke. These Phase II data indicate MSG rehabilitation was effective in improving functional goal attainment and internal strategy use. Importantly, gains were maintained and consolidated for 6 weeks after the intervention was completed. In contrast, CCT did not result in a significant improvement on functional, objective or subjective measures of memory. Given our somewhat modest sample size, we view this as preliminary evidence for the use of compensatory approaches to memory rehabilitation after stroke.
The authors would like to acknowledge all the participants who very generously gave their time for the project. In addition, we disclose that the CCT intervention was provided free of charge by Lumos Labs. However, all aspects of design, analysis and reporting were undertaken independently.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize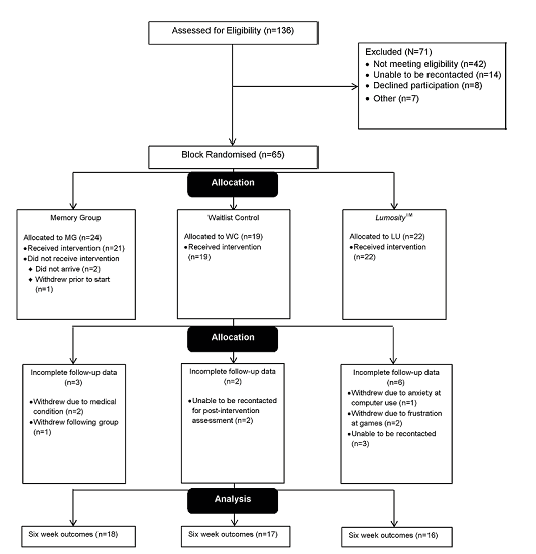 Click to show fullsize
Click to show fullsize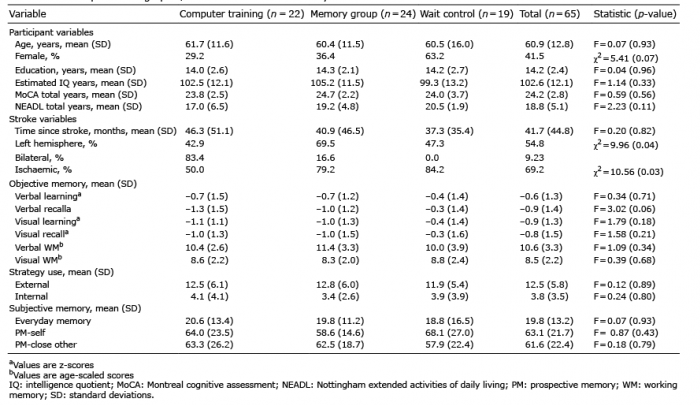 Click to show fullsize
Click to show fullsize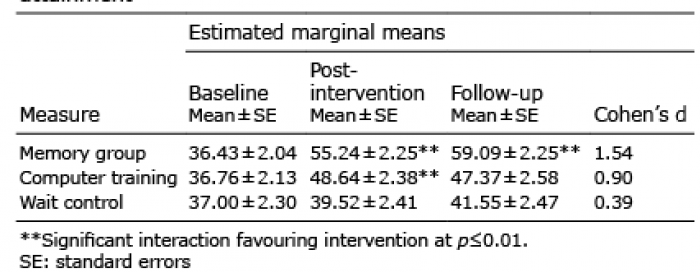 Click to show fullsize
Click to show fullsize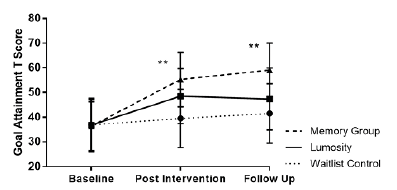 Click to show fullsize
Click to show fullsize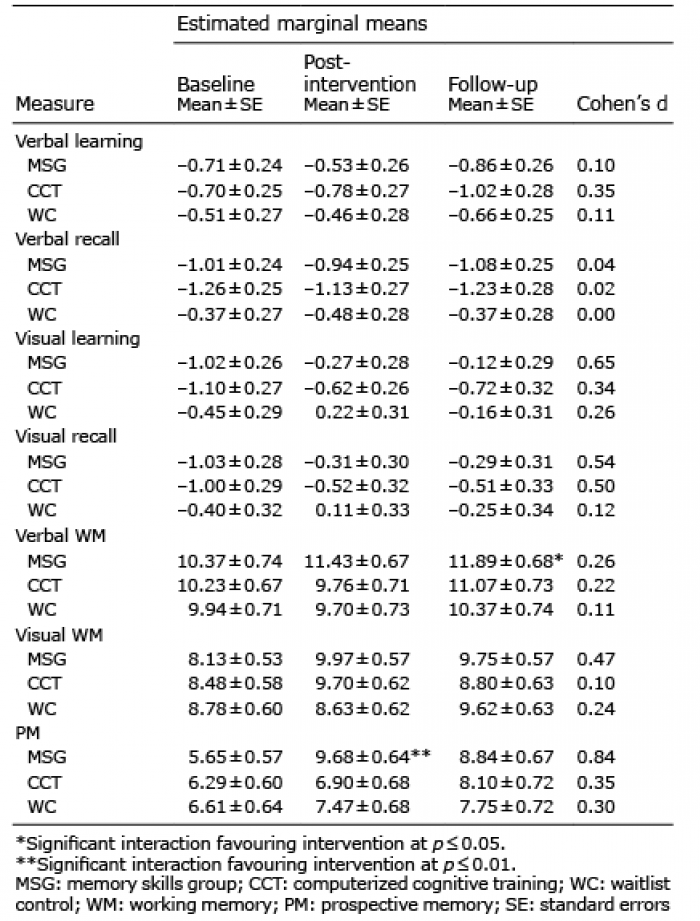 Click to show fullsize
Click to show fullsize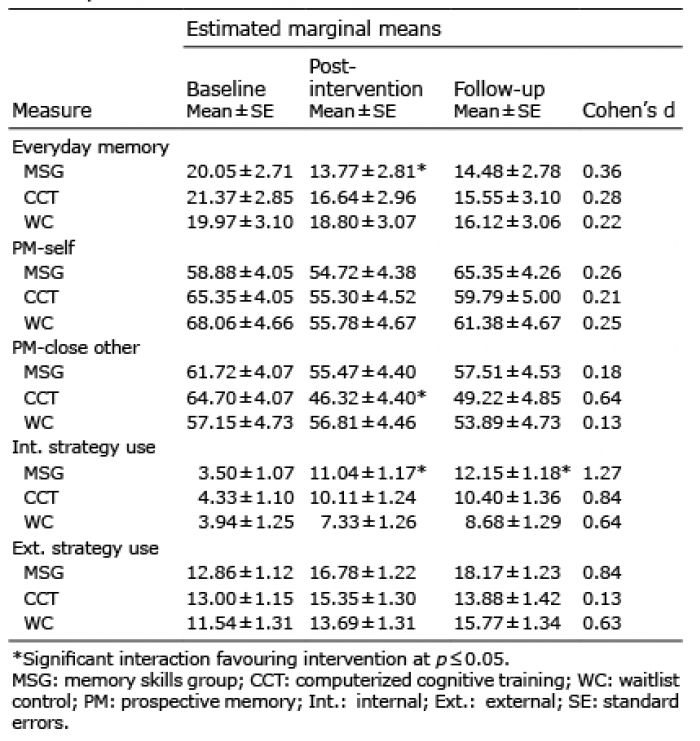 Click to show fullsize
Click to show fullsize